
Remember me
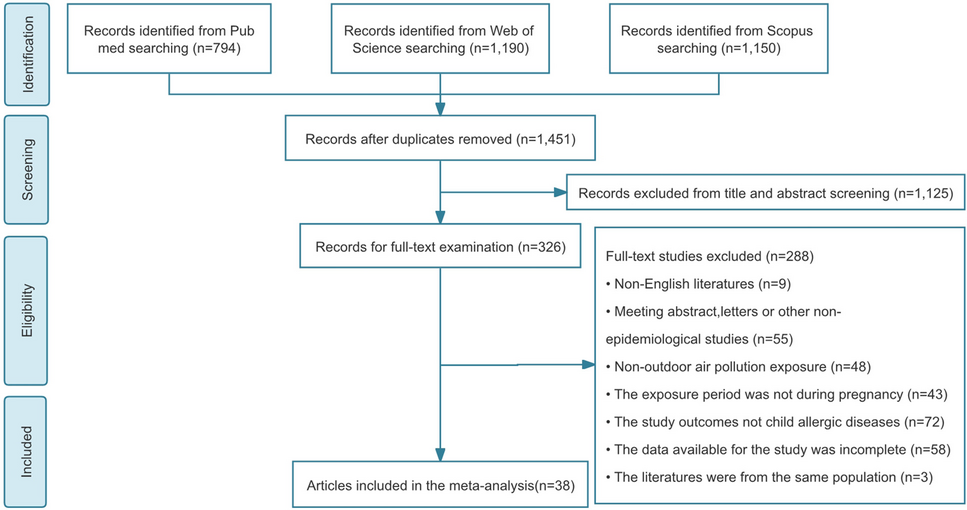





The initial PubMed search returned 2612 records, and the updated search identified an additional 179 records (Fig. 1). Of these, 58 publications describing 45 primary studies published between January 1, 2002, and May 15, 2023, met the inclusion criteria and were included in the present review. Of the 45 primary studies, 13 were RCTs (8 were phase 3 RCTs, 4 were phase 2 RCTs, and 1 was a phase 1b RCT), 7 were open-label studies, and 25 were observational studies (12 retrospective case series or chart reviews, 10 prospective cohort or registry studies, and 3 patient surveys). In the quality assessment of the 45 primary studies, 10 RCTs were assessed as having a low bias risk and 2 had a moderate bias risk; 1 non–placebo controlled pediatric RCT was assessed as having a high bias risk (Table S1. Supplementary Material). Of the 25 observational studies, 12 were considered high quality (≥ 6 of 8 stars), 7 moderate quality (4 or 5 stars), and 6 low quality (≤ 3 stars).
Fig. 1
PRISMA flow diagram of included studies. HAE-C1INH, hereditary angioedema with deficiency (type I) or dysfunction (type II) of the C1 inhibitor protein; LTP, long-term prophylaxis
Proportion of Patients Who Received LTP Who Were Attack-freeFor pdC1INH, 38% and 40% of participants aged ≥ 12 years were attack free after 16 weeks treatment with SC pdC1INH 40 IU/kg (n = 43) and 60 IU/kg (n = 43) twice weekly, respectively, in the phase 3 COMPACT trial (N = 90) [9] (Table 1), and 44% of participants were attack free after ≥ 52 weeks with SC pdC1INH 60 IU/kg twice weekly in the COMPACT open-label extension (N = 63) [13] (Table 2). No placebo-controlled RCT data reporting the attack-free rate were identified for IV pdC1INH. However, in the phase 3 CHANGE-3 open-label extension (N = 146), 35% of participants were attack free with IV pdC1INH 1000 U every 3 to 7 days across a median treatment period of 248 days [14] (Table 2). The efficacy of IV pdC1INH was directly correlated with the interval between administration (twice weekly versus once weekly) but not with historical attack frequency or duration of treatment [14]. Simulated pharmacokinetic modeling of functional C1INH from the COMPACT phase 2 trial predicted lower peak-to-trough ratios and higher trough values following SC pdC1INH administration than with IV pdC1INH [15], and may explain why a trend toward greater freedom of attacks was reported with long-term use of SC pdC1INH 60 IU/kg twice weekly (44%, N = 63) versus IV pdC1INH 1000 U every 3 to 7 days (35%, N = 146) in open-label extension studies [9, 14].
Table 1 Proportion of patients who received long-term prophylaxis who were attack free in phase 3 randomized placebo-controlled trialsTable 2 Proportion of patients who received long-term prophylaxis who were attack free in phase 3 non-placebo-controlled trials and real-world observational studiesFor lanadelumab, 39%, 31%, and 44% of participants aged ≥ 12 years were attack free after 6 months of treatment (150 mg every 4 weeks [Q4W; n = 28], 300 mg Q4W [n = 29], and 300 mg Q2W [n = 27], respectively) in the phase 3 HELP trial (N = 125) [8] (Table 1). In a post hoc analysis of steady state between day 70 and day 182 (n = 120), the attack-free rate reached 77% with use of lanadelumab 300 mg Q2W (n = 26) [8, 16]. In the HELP open-label extension (N = 209), 37% of patients were attack free with lanadelumab over a median 33 months of treatment [24] (Table 2). Similar attack-free rates were reported for rollover patients (defined as patients who participated in the HELP RCT and who continued into the HELP open-label extension) and non-rollover patients (defined as newly enrolled patients who had not participated in the HELP RCT) [24]. The attack-free rate was 35% in rollover patients (n = 106), who received a single dose of lanadelumab 300 mg at entry into the extension study and only received regular lanadelumab dosing (300 mg Q2W) after experiencing their first HAE attack in the study. Non-rollover patients (n = 103) received lanadelumab 300 mg Q2W from study entry onwards and had an attack-free rate of 37% [24]. Data on the real-world attack-free rate for lanadelumab are limited: in a single-center retrospective chart review, 56% of 9 patients were attack free with lanadelumab 300 mg Q2W or Q4W over a median 36 weeks of treatment [26]. However, only 25% of 12 patients were attack free following 12 months of treatment with lanadelumab 300 mg Q2W in a retrospective chart review of patients from Canada [25].
For berotralstat, 0%, 43%, 21%, and 39% of participants aged ≥ 18 years were attack free following 28 days of treatment (62.5 mg [n = 7], 125 mg [n = 14], and 250 mg [n = 15], and 350 mg [n = 18] QD, respectively) in the phase 2 APeX-1 trial (N = 75) [33]. The absence of a significant difference in attack-free rates was reported between participants who received berotralstat 150 mg QD (n = 40), berotralstat 110 mg QD (n = 41), and placebo (n = 39) across 24 weeks in the phase 3 APeX-2 trial (N = 121) [10]. However, the absolute attack-free rates in the APeX-2 phase 3 RCT and the subsequent APeX-S open-label extension were not reported [10, 34, 35].
No RCTs that reported attack-free rates were identified in the search window for patients who received LTP with androgens or TA. In observational studies, 24%-38% of patients who received danazol and ≤ 20% of patients who received TA for ≥ 1 year were attack free [28,29,30,31] (Table 2).
Attack Location in Patients Who Received LTPAttacks at all anatomic locations, including laryngeal attacks, continued to occur in patients who received LTP, regardless of the LTP agent [8,9,10, 18, 24, 30, 31, 36,37,38,39,40]. Of note, both interventional and observational studies reported that laryngeal attacks accounted for between 2%-7% of all attacks in patients who received LTP with pdC1INH, lanadelumab, danazol, or TA [8, 9, 18, 24, 36]. The occurrence of laryngeal attacks in patients receiving LTP with berotralstat was also reported in phase 2 and phase 3 trials [10, 34, 35]; however, the proportion of attacks with laryngeal involvement for each treatment group was not reported.
In phase 3 studies of lanadelumab and berotralstat, there appeared to be a differential reduction in peripheral attacks compared with abdominal and laryngeal attacks [8, 10, 24]. In the HELP RCT, the proportion of peripheral attacks decreased from 72% (56 of 78 attacks) during the 4-to-8 week run-in period to 43% (20 of 46 attacks) during the 26-week treatment period for participants who received lanadelumab 300 mg Q2W. Conversely, the proportion of abdominal attacks increased from 27% (21 of 78 attacks) during the run-in period to 50% (23 of 46 attacks) during the treatment period, and the proportion of laryngeal attacks increased (1% [1 of 78 attacks] during the run-in period to 7% [3 of 46 attacks] during the treatment period) [8], suggesting that the prophylactic effect is more pronounced in peripheral attacks than in abdominal and laryngeal attacks. Further, abdominal attacks were the most prevalent on-treatment attack location in participants who received lanadelumab (all dose levels and administration frequencies) in both the phase 3 HELP trial and open-label extension study (60% and 61%, respectively) over peripheral attacks (38% and 36%) and laryngeal attacks (3% and 4%) [8, 24]. In the phase 3 ApeX-2 trial there was a larger difference in the normalized monthly peripheral attack rate for berotralstat 150 mg QD versus placebo (0.5 vs 1.2) over the abdominal attack rate (0.2 vs 0.4), laryngeal attack rate (0.1 vs 0.2), and mixed-location attack free (0.6 vs 0.7) [10]. Baseline and on-treatment attack location data in patients receiving IV or SC pdC1INH were not reported in the pivotal phase 3 RCTs or open-label extension studies identified in this review [9, 13, 14, 41,42,43,44].
Attack Severity and Duration in Patients Who Received LTPA lower attack severity compared with placebo was reported in phase 3 placebo-controlled trials of SC and IV pdC1INH [9, 42]. In these trials, attack severity was assessed using an attack severity score based on a 3-point scale, with 1 indicating mild, 2 indicating moderate, and 3 indicating severe [9, 42]. The mean (SD) attack severity score was 1.6 (0.6) for SC pdC1INH 60 IU/kg twice weekly versus 1.9 (0.5) for placebo in the COMPACT trial (P value not reported) [9] and 1.3 (0.9) for IV pdC1INH 1000 U every 3 to 4 days versus 1.9 (0.4) for placebo in the LEVP2005-1 trial (P < 0.001) [42] (Table 3).
Table 3 Attack severity in patients who received long-term prophylaxis in phase 3 randomized placebo-controlled trialsThe phase 3 trial for lanadelumab (HELP) reported a significantly lower number of moderate or severe attacks per month versus placebo (P < 0.0001 for lanadelumab 300 mg Q2W) and a lower proportion of patients with a maximum attack severity of ‘severe’ versus placebo [8] (Table 3). However, the change in average attack severity from baseline during treatment with LTP was not reported. Attack severity data were not published in the phase 3 APeX-2 trial for berotralstat [10, 35]. Although significant differences for attack severity versus placebo were reported for IV pdC1INH and lanadelumab (Table 3), none of the pivotal phase 3 RCTs identified in this review reported a significant reduction from baseline in attack severity for any LTP agent [8,9,10, 35, 42].
Findings from phase 3 non-placebo-controlled trials (e.g., open-label extension studies) and observational real-world studies generally supported a reduction in attack severity from baseline with LTP use [20, 23, 24, 27, 36, 37, 45,46,47,48], although many are limited by small sample sizes (Table S2). The mean (SD) number of severe attacks per month decreased from 7.2 (7.1) at baseline to 0.4 (1.4) after 6 months and 0.3 (0.7) after 12 months of treatment (P < 0.0001) in a real-world audit of 62 patients commencing on lanadelumab 300 mg Q2W in the United Kingdom [45]. Berotralstat 150 mg QD for 4 to 6 months reduced the mean attack severity compared with the 3-month period preceding commencement of berotralstat (P < 0.0001) in a real-world patient survey of 54 patients in the United Kingdom [47]. However, no significant reduction in attack severity was reported for patients who received LTP with C1INH, androgens, or TA, compared with patients who received treatment with on-demand therapy only in 448 patients participating in a prospective icatibant registry study [36]. In a prospective cohort of 49 patients from Australia, a numerically lower proportion of attacks were rated as severe or significant in patients who received lanadelumab compared with patients who received on-demand therapy only, but the proportion of attacks rated as severe or significant was similar or higher in patients who received SC or IV C1INH or danazol compared with patients receiving on-demand therapy only [
Comments (0)