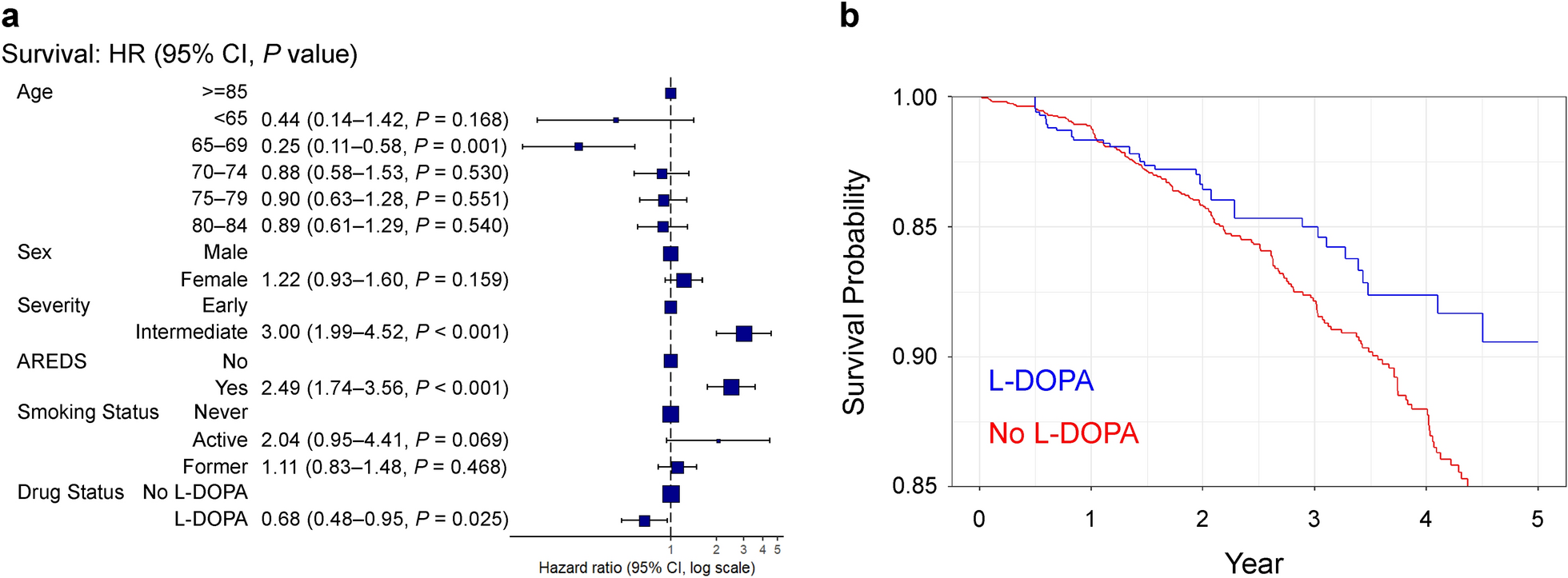
We found that L-DOPA exposure was associated with a 32% risk reduction in new-onset GA detection over a period of 1–5 years. These results support the hypothesis that L-DOPA exposure may reduce the likelihood of GA development. Since complement pathway inhibitors, such as pegcetacoplan or avacincaptad pegol, only reduce GA growth by 15%–20% [5, 6] and have the potential for devastating complications like occlusive retinal vasculitis [7], alternative treatments to prevent GA onset are important for the future of dry AMD treatment.
There are several potential mechanisms that may explain the effects of L-DOPA exposure on the development of GA. The pathophysiology of GA is multifactorial and includes oxidative stress at the RPE, complement-induced inflammation, exosomes, and choriocapillaris loss [2, 19,20,21]. Exogenous L-DOPA dilates the choroidal vasculature via the D1/D5 dopamine receptor in animal studies [17]. In agreement, patients with Parkinson’s disease taking L-DOPA demonstrate significantly greater choroidal thickness compared to age-matched controls without Parkinson’s disease [18]. Since choriocapillaris loss predicts drusen accumulation and GA progression [19, 20], it is possible that L-DOPA treatment improves choriocapillaris perfusion through choroidal dilation. Additionally, Parkinson’s disease patients have inner retinal atrophy compared to age matched controls [18]. It is possible that inner retinal atrophy leads to greater perfusion of the outer retina from the retinal circulation, improving relative ischemia and preventing GA. Furthermore, exosomes are secreted from the apical and basolateral surfaces of the RPE and contribute to drusen development and AMD progression [21]. Since L-DOPA agonism of GPR143 reduces exosome release from the RPE [11], L-DOPA exposure may protect from GA progression via reduced exosome production. Finally, L-DOPA can reduce oxidative stress in RPE cells [16], which is another potential mechanism of L-DOPA protection against GA.
Time to GA development was 1.7 years in control eyes and 2.1 years in L-DOPA exposed eyes (Table 1). We hypothesize that since the majority of L-DOPA exposed eyes developed GA in the first 2 years (26 of 40 total eyes) that L-DOPA exposed eyes were referred at a later disease time point to a retinal specialist compared to control eyes. Unfortunately, we do know how long these eyes were exposed to L-DOPA prior to referral to a retinal specialist. Therefore, future studies are needed to investigate the timing between L-DOPA exposure and GA development.
In addition to L-DOPA exposure, we identified younger age as a protective factor and intermediate AMD as well as AREDS2 use as risk factors for new-onset GA detection. Drusen types that would be classified as intermediate rather than early AMD are associated with GA incidence and progression [22,23,24]. Similarly, older age is associated with new-onset GA [22, 24]. Contrary to our data, AREDS supplements do not have a significant effect on the development or progression of GA [4]. We suspect that this is a confounding result where intermediate AMD stage and the use of AREDS2 vitamins are highly correlated and their individual effects cannot be deciphered.
There were several limitations with our study. First, like all database studies, the accuracy of our results is dependent upon the quality of data available in the Vestrum Health Retina Database. Since fundus photos, optical coherence tomography, and fundus autofluorescence were not available for confirmatory review in the Vestrum deidentified database, our results are reliant on diagnosis coding. Second, patients with Parkinson's disease may not return to the eye clinic for follow-up appointments because of reduced mobility, which would reduce the detection of new-onset GA, and/or mortality. However, our use of PSM matched the control and L-DOPA exposed groups so that each group had an identical follow up period (Table 1, 2.6 years for control and 2.5 years for L-DOPA), partially negating this limitation. Third, our analysis only controlled for age, sex, smoking status, AREDS use, and AMD stage as covariates. We cannot rule out the influence of other covariates like co-existing retinal disease or systemic factors. Fourth, because many of the systemic past medical histories were incomplete, it is unknown how the stages of Parkinson's Disease were distributed; thus, the impact of Parkinson’s Disease stage on new-onset GA is unknown. Finally, since patients with Parkinson’s disease are frequently prescribed L-DOPA, we cannot rule out that Parkinson's disease and not L-DOPA medication reduces new-onset GA through improved choroidal perfusion.







Comments (0)