
Remember me





This prospective cohort study was approved by the Ethics Committee of Nihon University School of Dentistry (Permit No. EP16D013) and was conducted in accordance with the 1975 Declaration of Helsinki as revised in 2013, as well as in accordance with the guidelines for observational/descriptive studies on enhanced reporting of observational studies in epidemiology [20]. The cohort of this study comprised patients who attended the Department of Dental Implantology at Nihon University Dental Hospital for maintenance treatment between January 2016 and February 2024.
Case selection criteriaTo avoid interoperator bias, a single periodontist (KS) diagnosed and planned the treatment of all patients. Patients were provided with periodontal treatment, implant surgery, prosthetic treatment, and maintenance as necessary. The inclusion criteria were as follows: (1) implants previously placed in our clinic, (2) patients aged 40 years or older who visited the clinic for implant maintenance or new implant placement in 2016 or later when the study was initiated, (3) patients who had not been treated with AOMs at the beginning of the study period, (4) patients who had been undergoing regular maintenance treatment for at least 1 year after the placement of the superstructure. Exclusion criteria were: (1) no record of clinical parameters at the time of maintenance treatment, (2) no dental X-ray or digital panoramic radiography (DPR) images at the time of re-evaluation, (3) patients who had not visited the hospital since 2016 (for reasons including death and relocation) (Figs. 1 and 2).
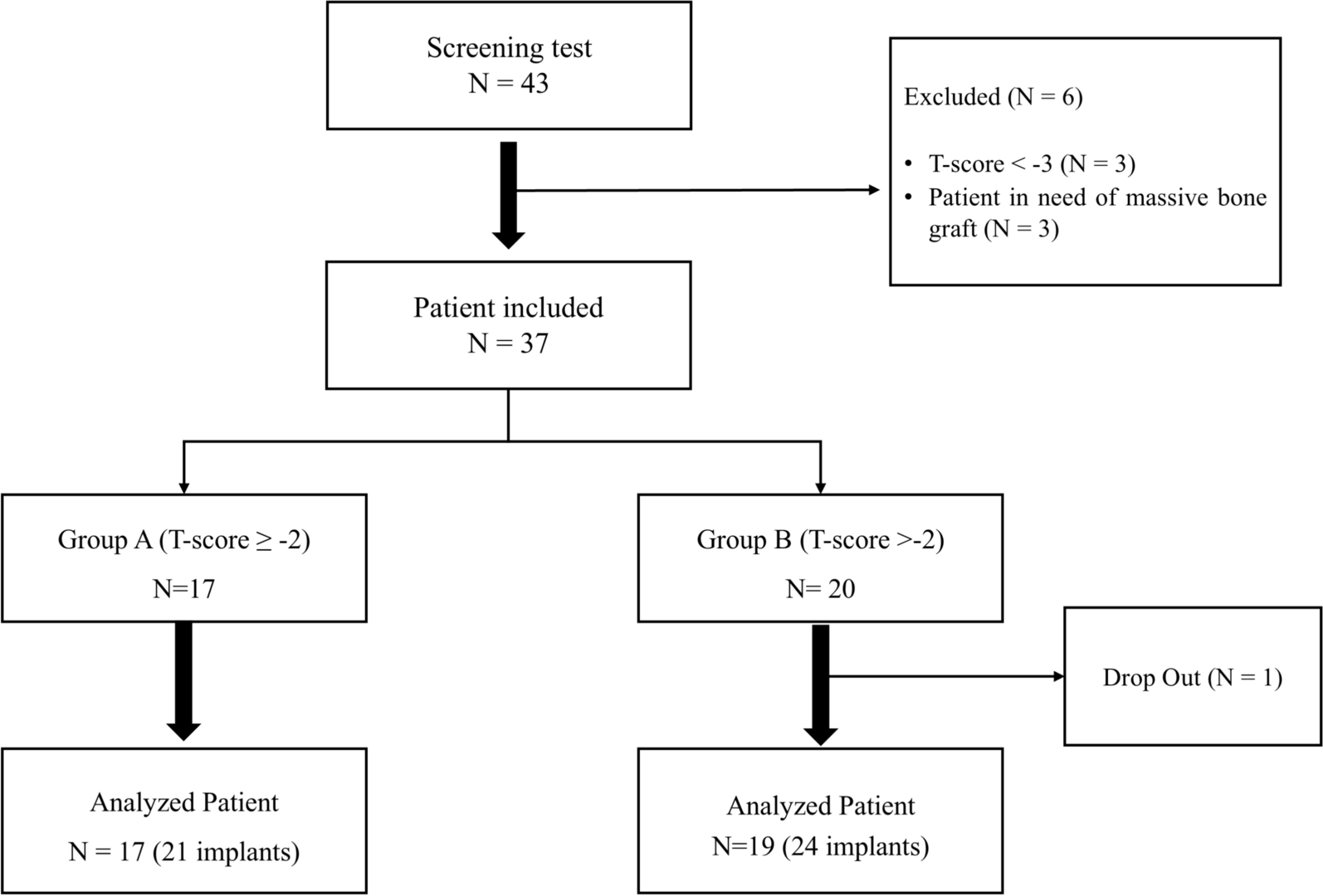
Fig. 1
Flowchart of the study population
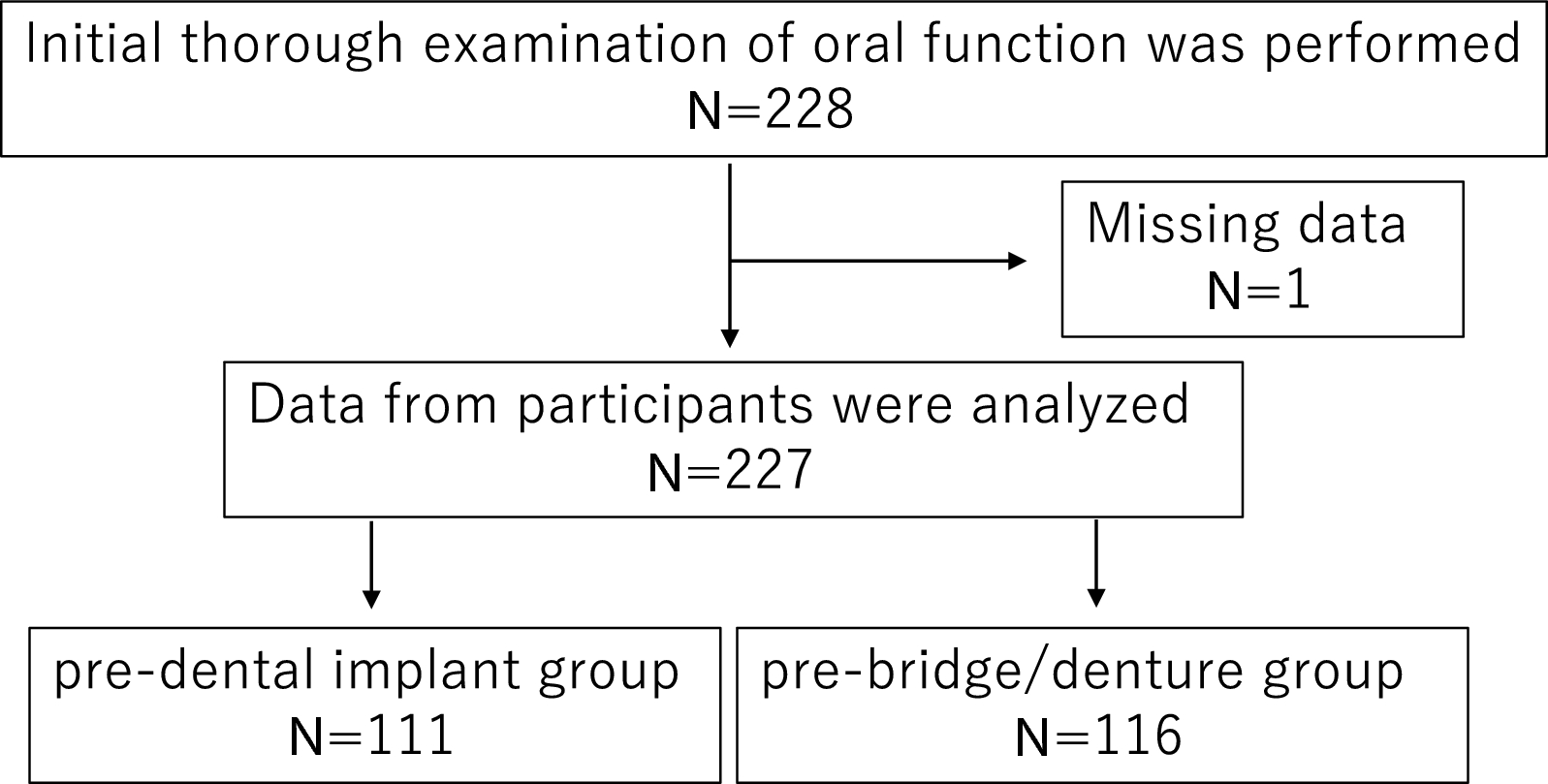
Fig. 2
Inclusion and exclusion criteria
Implant placement protocols and prosthetic designAll implant surgeries were performed with a two-staged approach and according to the manufacturer’s instructions under either local anesthesia alone or with intravenous sedation. For implant sites with insufficient bone mass, simultaneous bone grafting with autogenous or artificial bone was performed at the time of implant placement. Postoperative medications were oral antibiotics (cefuroxime axetil, cefcapene pivoxil hydrochloride hydrate, and amoxicillin hydrate) three times a day for 3 days after surgery to prevent infection. Analgesics (diclofenac sodium and loxoprofen sodium hydrate) were prescribed as needed. Seven days after each surgery, all sutures were removed, and the patients were instructed to maintain good oral hygiene. After a sufficient period of soft tissue healing, the superstructure was fabricated. In the past, gold alloy custom abutments were combined with metal-ceramic restorations, but in recent years, titanium bases or titanium abutments with zirconia crowns have been used. The type of prosthetic fixation was determined by the direction of implant placement, the location of access holes, esthetics and cleanability, and whether fixation was by screw or cement.
Investigation of clinical parameters of peri-implant tissueThe baseline for recording the clinical parameters of the peri-implant tissues was at the start of maintenance after placement of the final prosthesis. However, for the cases in which prosthetic treatment had been completed at our clinic and maintenance had already started, we used the examination data from the earliest visit within the study period. At the time of re-evaluation, data from the last visit within the study period were evaluated. The clinical parameters measured for each individual implant are set out below. Data collection and analysis were performed by two operators. Statistical analysis of the final dataset was then performed by a secondary operator, who remained blind to the study objectives and methods.
Implant probing pocket depthTo standardize the probing pressure (0.15 N), the operator's measured pressure was calibrated many times using an electronic scale. The operator inserted a periodontal pocket probe (11 Colorvue® Probe Kit, Hu-Friedy, Chicago, IL, USA) into the peri-implant pocket with a force of 0.15 N and measured the depth in 1-mm increments at six points. The mean depth and the deepest point were calculated from the six pocket depths. The implant probing pocket depth (iPPD) was calculated as the difference in depth between the baseline and the last visit (last visit minus baseline).
Implant bleeding on probingImplant bleeding on probing (iBoP) was evaluated 10 s after the six-point probing. No bleeding was quantified as negative (score: 0) and bleeding as positive (score: 1), and the mean value of the six points was calculated (final score range: 0–1). The iBoP was calculated as the difference between the baseline value and the value at the last visit (last visit minus baseline).
Evaluation of bone resorption over time on dental X-rayThe amount of marginal bone loss (MBL) around the implants was measured on dental radiographs taken using a paralleling technique (irradiated at 110 kV, 1–20 mA, and effective dose of 100 µSv). The distance from the proximal or distal platform of the implants to the bottom of the bone defect was measured on the obtained images (TechM@trix, SDS Viewer, Tokyo, Japan), and the amount of bone resorption per implant was averaged (Fig. 3). The MBL was calculated as the difference between the baseline value and the value at the last visit (last visit minus baseline).
Fig. 3
The amount of marginal bone loss was defined as the average of a and b. a: distance from the proximal platform of the bottom of the bone defect (mm), b: distance from the distal platform of the bottom of the bone defect (mm), p: implant platform
Diagnosis of peri-implantitisAfter the superstructure was placed, maintenance treatment was performed at intervals of 3–6 months according to the oral hygiene of each patient. Peri-implant disease was diagnosed by probing and radiographic examination of the peri-implant tissues during the subsequent follow-up re-evaluation. Peri-implantitis was diagnosed in accordance with the statement of the World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, considering inflammation of the peri-implant mucosa and progressive resorption of the supporting bone [21] (i.e., a deepened implant probing depth or radiographic bone resorption compared with baseline). Additional diagnostic criteria were: (1) probing depth greater than 6 mm, (2) drainage or bleeding during probing, and (3) radiographic evidence of bone resorption greater than 25% of the implant length.
Diagnosis of PI-MRONJPI-MRONJ was diagnosed when MRONJ developed in the tissue surrounding the implant. Patients were diagnosed with MRONJ when they had a history of taking bone resorption inhibitors or angiogenesis inhibitors, no history of radiation therapy of the jawbone, and bone exposure or osteonecrosis in the oral or maxillofacial region lasting more than 8 weeks [4]. Staging was classified as 0–3; stage 0 was defined as clinical symptoms persisting for at least 8 weeks without bone exposure, or bone exposure and persistence of symptoms for at least 4 weeks, and nonspecific clinical or radiological changes or symptoms without osteonecrosis.
Mandibular cortical index assessmentA blurred and rough appearance of the mandibular inferior cortical bone on DPR images has been reported to correlate with the severity of osteoporosis [22]. Using all DPR sample images, the mandibular inferior cortical bone morphology was classified into three types, according to the report of Klemetti et al. [23]. Class 1 has a smooth cortical bone inner surface, class 2 has an irregular inner surface of cortical bone with linear resorption, and class 3 has severe linear resorption and cortical bone rupture over the entire cortical bone. Two sites were evaluated per patient, one on the left side and one on the right side, and each was recorded. The mandibular cortical index (MCI) was assessed twice by a dentist (KS) who was trained in classification beforehand, and the second assessment was used. The higher MCI score (whether right or left side) was adopted as the representative value, and was used as the final MCI evaluation for each patient.
Data source and group settingsInformation on age, sex, body mass index (BMI), history of fragility fracture (excluding traumatic injuries caused by sports or accidents before adolescence) [24, 25], smoking habits, and history of moderate or severe periodontitis was collected from the initial examination records. From the records collected during the maintenance treatment, information was extracted on AOM treatment initiated after implant function, implant size and placement site, type of superstructure fixation (cement or screw fixation, including side screws), MCI classification, peri-implant clinical parameters (iPPD, iBoP, MBL), peri-implantitis, and MRONJ development. For all implants, the period from the day the superstructure was placed to the last visit was set as the observation period. The clinical parameters of implants removed as a result of peri-implantitis were taken from the data recorded most recently at the time of removal. Patients were divided into two groups: the AOM group (those who started AOM treatment after implant function) and the control group (those with implants who did not undergo AOM treatment).
Statistical analysisAll statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Japan), a graphical user interface of R (The R Foundation for Statistical Computing, Vienna, Austria, version 4.0.0) [26]. EZR is customized for easy analysis by incorporating R Commander, a package of additional functions of R. The software is designed to add statistical functions frequently used in biostatistics.
The required sample size calculated with a two-tailed test with an alpha error of 0.05 and power of 0.8 was 37 for the AOM group and 74 for the control group. Using the demographic data of the AOM and control groups obtained by descriptive statistics, we tested the statistical differences for each variable. Normality of the data distribution for continuous variable outcomes (age, BMI, follow-up period, iPPD, iBoP, and MBL) was determined by the Kolmogorov–Smirnov test, and P ≥ 0.05 was considered as a normal distribution. When the data followed equal variances and were normally distributed, Student’s t test was performed. When they did not follow a normal distribution, the Mann–Whitney U test was performed. Fisher's exact test or a chi-square test was employed for categorical variables (sex, history of fragility fracture, smoking habit, history of periodontitis, MCI classification, presence of peri-implantitis, and type of superstructure fixation).
To examine risk factors, univariate analysis was first performed using the items that differed between the two groups as explanatory variables and peri-implantitis as the objective variable, and crude odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A logistic regression model was used to measure the association between predictor and outcome variables while controlling for confounding factors, and adjusted odds ratios (aOR) were determined. P < 0.05 was considered to indicate a statistically significant difference. Even when multiple implants were present in a single patient, the health status of the host was expected to change because of the different timing of implant placement, prosthetic methods, and functional periods. Hence, for the purpose of examining the effect of AOM treatment on the clinical parameters of individual implants, the tests were analyzed on an implant basis (Fig. 4).
Fig. 4
Digital panoramic radiography imaging findings in case 5. A 70-year-old woman had been using alendronate orally for 4 years after implant function. The #16–#14 implants were removed as a result of peri-implant medication-related osteonecrosis of the jaw (PI-MRONJ), and it has been 7 years since the drug was changed to raloxifene hydrochloride (SERM). The #36 implant was diagnosed with peri-implantitis. The mandibular cortical index (MCI) classification was class 3 (arrowhead)
Comments (0)