
Remember me




This was a prospective randomized study that was carried out at Kasr Alainy hospitals, Cairo University between December 2022 and March 2024. The study was notarized by the research committee of ethics with code N-126. All participants were given a full elaboration on the study’s objectives and methods, and finally, a written consent was obtained from each participant.
The study comprised all patients aged ≥ 18 years old with isolated upper polar renal stones ≥ 20 mm in the maximal dimension while, patients with concomitant urinary tract stones or with prefixed ureteral stents or with active urinary tract infection were excluded. The participants were evaluated clinically, by full preoperative labs, urine analysis with treatment of infection if exists till clearance, and CT urography unless contraindicated. The patients underwent either percutaneous nephrolithotomy (group P) or retrograde intra-renal surgery with laser lithotripsy (group R) according to a preoperative computer-generated block randomization.
For group (P), after premedication with IV midazolam and pre-oxygenation at fraction of inspired oxygen (FIO2) 0.8, induction of general anesthesia was performed using propofol, fentanyl, and atracurium. Through the direct laryngoscopy, a double lumen endotracheal tube was inserted then checked by a fiberoptic bronchoscopy. During achieving the renal access, one lung ventilation (OLV), unless contraindicated, was conducted on a tidal volume of 6 ml/kg, respiratory rate at 16–20/min, and CO2 level up to 45mmHg. Before and after achieving the renal access, conventional two lung ventilation was performed. The patients were monitored thoroughly by electrocardiogram, pulse oximetry, capnography, and non-invasive blood pressure manometry.
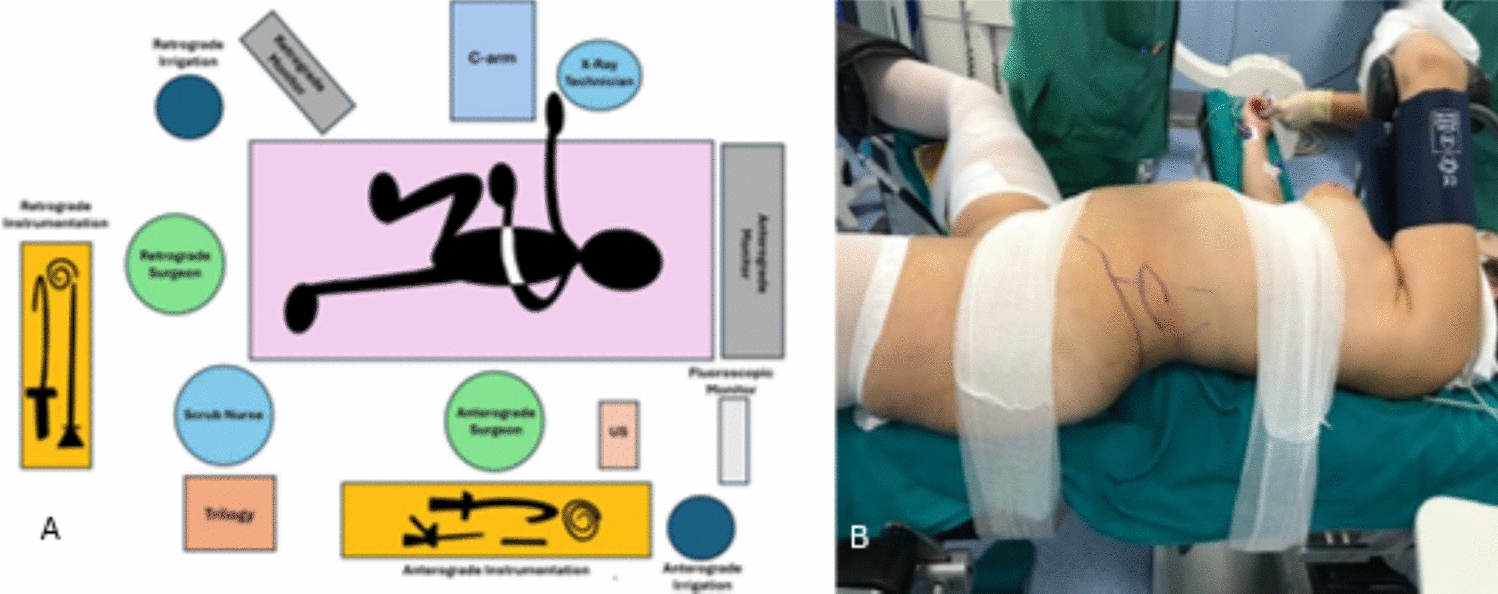
Under lithotomy position, cystoscopy and ipsilateral retrograde ureterography were carried out and an external ureteral catheter was inserted then the patients were put in the standard prone position. After surface marking of the last three ribs, paraspinal muscles, and the posterior axillary line, a 4.2 MHz abdominal transducer probe connected to a Siemens Acuson ultrasound (P500) was used to delineate the safe plane between the lung with its pleural covering, pleural recess and the upper pole of the kidney through the longitudinal plane approach. To preclude the renal parenchymal avulsion and pleural recess injury, the puncture site was always medial to the posterior axillary line and the puncture needle was directed to the calyx harboring the stone, targeted calyx, travelling through the renal parenchyma into the calyceal fornix, the renal papilla by the ultrasound view (Supracostal Ultrasound Guided Approach, SUGA). A J tip guidewire was then pushed gently through the targeted calyx to the renal pelvis. One cm transverse skin incision, at the lower half of the intercostal space and close to the puncture needle, was made then the tract was radially dilated by an Olbert balloon dilator (NephroMax 30Fr, inflated up to 20atm) and maintained by sliding an Amplatz sheath over the balloon, Fig. 1.
Fig. 1
by Ahmed Assem, ahmed.assem@cu.edu.eg, with all rights preserved
Demonstrates SUGA-PNL technique. A; shows the surface landmarks of last 3 ribs and the posterior axillary line, B; puncture needle placement supra-costal approach guided with ultrasound, C; ultrasound image shows the needle puncture through the targeted upper calyx harboring the stone, red arrow is the stone, white arrow is the puncture needle, blue arrow and yellow outline showed lung base, D: Fluoroscopic image of retrograde pyelography after needle placement in the targeted upper calyx. Notably, these figures are archived photos which were taken during the study, compiled
Through nephroscopy (KARL STORZ set, 26Fr operating sheath), the stones were disintegrated by pneumatic lithotripsy (Swiss LithoClast®, EMS) and retrieved by a nephroscopic forceps (KARL STORZ, 10.5Fr). The stone free status was checked by the nephroscopic vision and radiological control. Eventually, the Amplatz sheath, along with the external ureteral catheter, was removed without nephrostomy tube insertion. The indwelling jj stent was inserted only whenever indicated, i.e., inaccessible residual stones or pelvi-calyceal system injury. To assess the thoracic complications, an immediate postoperative chest x-ray was uniformly performed.
For group (R), under general anaesthesia, the patients underwent cystoscopy and ipsilateral ureterography in lithotomy position. A 7Fr (KARL STORZ) ureteroscope was advanced beside a previously passed guidewire to inspect the ureter and to assist the passive ureteral dilatation then a ureteral access sheath (UAS) (Navigator TM HD, 11/13Fr, 46 cm) was placed over the guidewire under fluoroscopic guidance. Ureteral tightness was considered if the small caliber ureteroscope could not be passed smoothly into the ureter and in such condition, the patient was ruled out. A single-use digital flexible ureteroscope (LithoVueTM, 9.5Fr, Boston Scientific) was advanced inside the UAS and laser lithotripsy (273 micron core diameter FlexiFib laser fibre connected to a high power Sphinx Holmium laser device, 80W) was implemented after stone identification through stone dusting (25–30HZ, 0.5J) alternating with stone fragmentation (5–8HZ, 2.5–3J) in a subjective continuum manner. A handful of stone fragments were retrieved by a Dormia basket (Zero Tip Nitinol Retrieval Basket, 3Fr, 120cm, Boston Scientific) for stone analysis. Lastly, the UAS was withdrawn under optical vision to inspect the entire ureter and the ureteral jj stent was only placed in case of significant ureteral injury in adherence to Traxer's Post Ureteroscopy Lesion Scale (PULSE, ≥ 3) [8].
The intraoperative parameters such as radiation time, total operative time, and irrigation fluid volume were monitored and compared between the two groups. In addition, the hospital stay, the catheterization time, and the pain score through the visual analogue scale (VAS) were documented. All intraoperative and postoperative complications were assessed and classified according to clavien-dindo scale. Postoperative systemic inflammatory response syndrome (SIRS) and sepsis were defined according to the National Institute for health and Care Excellence (NICE) guidelines [9].
During follow up, all patients were asked to visit the outpatient clinic after the first week of surgery then according to a scheduled regimen (at the 1st month, 3rd month and 6th month after surgery). A non contrast (NC) CT scan was planned at the 1st month visit to detect the stone free status where less than 2 mm residual stone was considered a stone free and the patients were then assessed for the need for auxiliary procedures. A urine analysis, kidney-bladder ultrasound, and serum kidney functions were also revised during the visits.
Comments (0)