Faster sputum cultures could simplify patient care and increase cost-effectiveness. Shortening the processing time of sputum cultures is important from a public health perspective, as MDR/RR-TB patients with positive sputum cultures are contagious and may spread the disease to contacts. It is crucial to investigate the factors that predict early and interim sputum culture un-conversion in a high TB burden country like China.
This study was conducted in eight institutions located in various regions of China, including the East, West, South, North, and Central region. This geographical diversity was beneficial in minimizing any imbalances in demographic characteristics. The study conducted a multivariable analysis to collect common risk factors associated with culture conversion and treatment outcomes which covering various aspects including socio-demographic characteristics, epidemiology, clinical features, comorbidities, DST patterns, and treatment regimens from previous studies [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] to reduce the impact of confounding factors. Additionally, the study collected retrospective clinical data from 2018 to 2022, coinciding with the introduction of BDQ to China under the New Drug Introduction & Protection project. The findings from this study can help identify possible predictors for early and interim culture un-conversion and contribute to the future implementation of BDQ-containing regimens and related short-course regimens (such as the 6-month BPaLM regimen or the 9-month all-oral regimen [27]) in China.
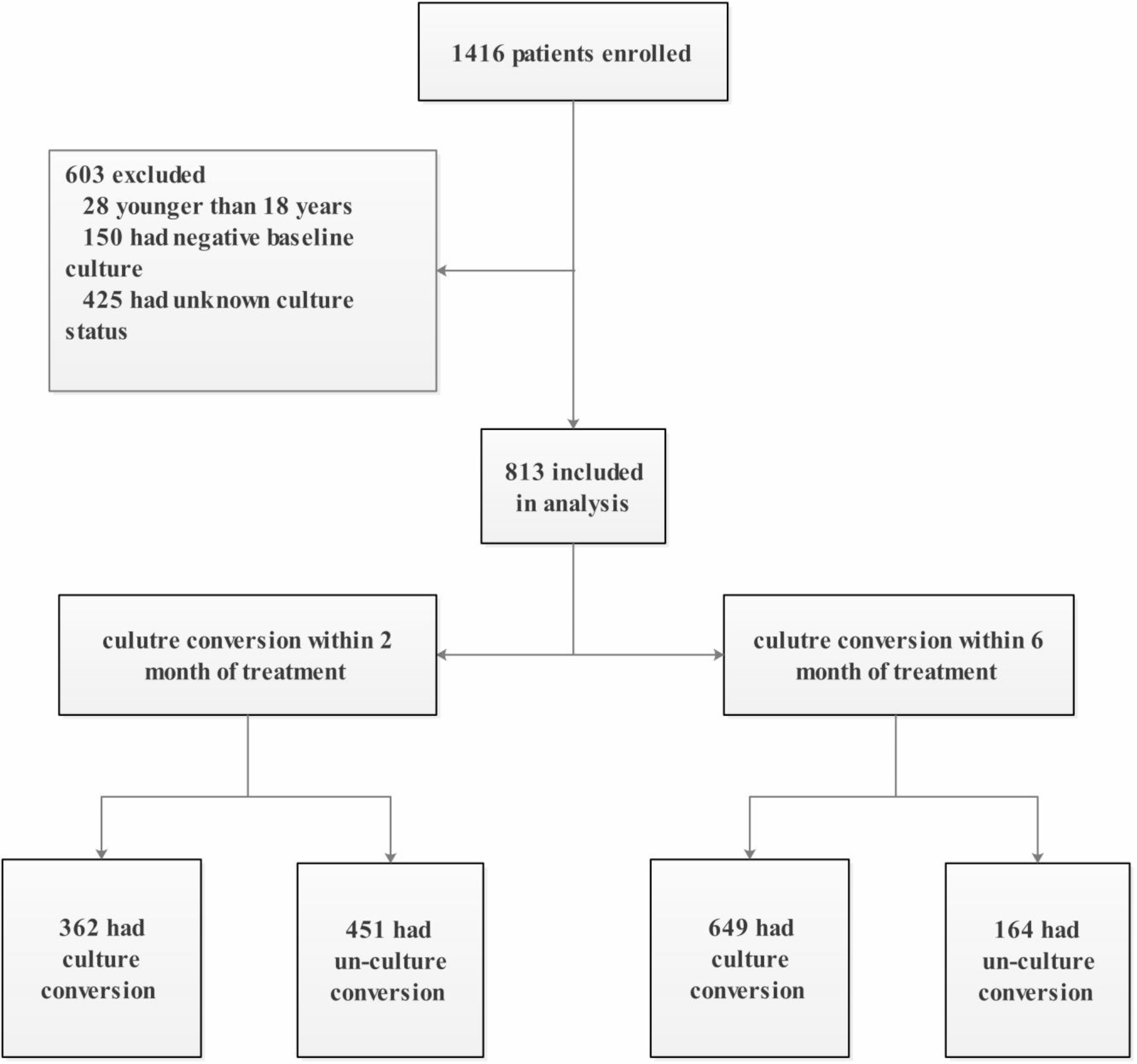
In this study, 44.5% of the overall MDR/RR-TB patients achieved culture conversion within 2 months, in line with the previous studies of MDR-TB (ranging from 30%~57.4% [3, 5, 9, 35]). About 79.8% (649/813) patients achieved culture conversion within 6 months of treatment, consistent with previous studies (ranging from 70%~90%) [8, 22, 29, 35,36,37]. The median time for conversion was 2.00 (1.50, 3.00) months within 6 months of treatment, which falls within the duration reported in previous studies (31 days to 91.5 days [3, 6–7, 13, 15–16, 39,40,−41]).
Through a multivariate analysis, we discovered various factors that independently predicted early and interim culture un-conversion. Patients who had a positive AFB smear, cavities, bilateral disease, and viral hepatitis were found to have a higher probability of experiencing culture un-conversion within 2 months of treatment. Additionally, male patients with a history of smoking, previous treatment for TB, bilateral disease, viral hepatitis, and those who received a regimen without BDQ were more likely to experience culture un-conversion within 6 months of treatment. Part of the predictors of early and interim culture un-conversion were overlapped. Notably, the relationship between sputum culture conversion and a successful outcome was found to be significantly stronger at 6 months compared to 2 months [2]. As a result, it is important to give more consideration to the independent risk factors that influence the interim sputum culture conversion.
The presence of an initial positive or a high grade AFB smear, which indicated a relatively high bacillary burden, was a known predictor of a longer time for sputum conversion in patients with pulmonary tuberculosis [8, 13, 15, 38, 39], and a single center study in Korea found that an initial positive AFB smear was associated with culture un-conversion within 3 months of treatment [40]. These findings are consistent with our study. Notably, a positive AFB smear might had a greater influence on early culture conversion compared to interim in our study.
Historically, patients with MDR-TB [9] and drug-susceptible tuberculosis (DS-TB) [10] who had cavities have been found to have a higher risk of culture un-conversion within 2 months of treatment compared to patients without cavities, which was consistent with the findings of our study. Cavities have long been recognized as a risk factor for delayed culture conversion and treatment failure in TB [4, 6,7,8, 16, 38, 39, 41,42,43]. The presence of cavities might hinder the penetration of drugs and consequently reduce the effectiveness of antimicrobial agents [21].
In a prospective cohort study on MDR-TB in America, it was found that bilateral disease (OR 1.90, 95% CI 1.20–3.01) was identified as an independent risk factor for a poor treatment outcome [17]. Our study also found a similar association between bilateral disease and early /interim culture un-conversion. Patients with more extensive lung lesions may experience a longer duration for culture conversion. It is important to note that while bilateral cavitations have often been considered as a potential risk factor for poor treatment outcomes or culture conversion [4, 6], our study separated the lesion scope and cavity, reducing the mutual influence of objective predictors.
Viral hepatitis was identified as an independent predictor for culture un-conversion within early and interim treatment in patients with MDR/RR-TB. This finding was consistent with a study in Armenia and Georgia, which showed that co-infection with hepatitis C virus (aOR 4.45, 95%CI 1.23–16.13) was associated with unsuccessful outcomes in MDR-TB patients who received BDQ through compassionate use [44]. However, the endTB observational study found no association between hepatitis C infection and conversion [8]. This lack of association could be attributed to differences in sample size, race, treatment regimen, and other factors. Notably, HCV co-infection was found to be linked with higher levels of drug-induced liver injury (DILI) in MDR-TB patients [45, 46]. Although we assessed the proportion of adverse effects in our study, we were unable to analyze the relationship between viral hepatitis and DILI due to the retrospective nature of the study and the lack of information on the timing of adverse effects occurrence, the specific type of viral hepatitis, and the antiviral treatment status. Additionally, there is currently no published data available on the effects of new treatments for HCV infection with direct-acting antivirals on mortality and hepatotoxicity in co-infected MDR-TB patients [44].
Substantial evidence exists suggesting that smoking delays culture conversion or associated with culture un-conversion in MDR-TB patients [15, 16, 47], consistent with our finding that smoking was an independent risk factor for interim culture un-conversion. Smoking has been linked to compromised immune mechanisms, such as a reduction in the phagocytic function of alveolar macrophages [48]. Therefore, in a country with a high burden of MDR-TB like China, it is suggested that a new approach to TB control should include a smoking cessation program to potentially reduce the time for culture conversion. The history of previous tuberculosis treatment has been identified as an independent predictor for delayed culture conversion [14] and poor treatment outcome [6, 17] in patients with MDR-TB. This finding aligns with our findings, which showed that previous treatment for tuberculosis was independently associated with interim culture un-conversion.
According to the guideline of WHO [32] and the consensus of China [28] in 2018 and 2019 respectively, BDQ has been designated as a Group A drug for the treatment of MDR/RR/XDR-TB. Regimens containing BDQ have shown potential in achieving early culture conversion [22] or increasing the conversion rate [23,24,25,26]. Since the use of BDQ is still limited in China, part of this study objective to determine whether a regimen containing BDQ can facilitate early and interim culture conversion. Our study found that regimens containing BDQ were an independent predictor for interim culture conversion, similar to previous studies [22,23,24,25,26]. In a study conducted in China, MDR-TB patients who received a BDQ-containing regimen achieved a culture conversion rate of 80.6% (108/134) at the 8th week and 96.8% (120/124) at the 24th week [49]. The culture conversion rate at the 24th week in this study was similar to our study (88.8% for patients who received BDQ-containing regimen within 6 months), suggesting that BDQ has the potential to achieve early culture conversion. In this study, only 5.6% (13/232) of patients who received a BDQ-containing regimen experienced a QTcF prolongation exceeding 500 ms. This suggested that BDQ-containing regimens have an acceptable level of cardiotoxicity. However, short-course regimens such as the 6-month BPaLM/BPaL regimen have not been utilized in China due to the unavailability of pretomanid. Additionally, the 9-month all-oral regimen containing BDQ has not been widely adopted. Therefore, it is crucial to promote the use of BDQ-containing regimens and encourage the adoption of shorter treatment regimens in China.
In addition to the independent predictors mentioned above, our study also identified several factors that were significantly associated with early or interim culture un-conversion. These factors included male, age, BMI<18.5 kg/m2, alcohol use, and anemia. These associations were observed in the univariate analysis. Two previous studies have shown that being male is an independent risk factor for 2-month sputum culture un-conversion [10, 12]. However, our study differs from these previous ones as they mainly focused on DS-TB, with only 3.8%~5.9% of the patients being MDR-TB [10, 12], and elderly patients with a mean age of 64.7 ± 19.2 years [12]. Additionally, age was found to be significantly associated with sputum smear conversion time in patients with new DS-TB [42]. Alcoholism [13] or drinking [15] were independent predictors of less likely conversion in MDR-TB patients. Baseline anemia was reported to be associated with an unfavorable treatment outcome [50, 51]. However, gender, age, alcohol use, and baseline anemia alone were not sufficient to be considered independent risk factors for early






Comments (0)