Population study
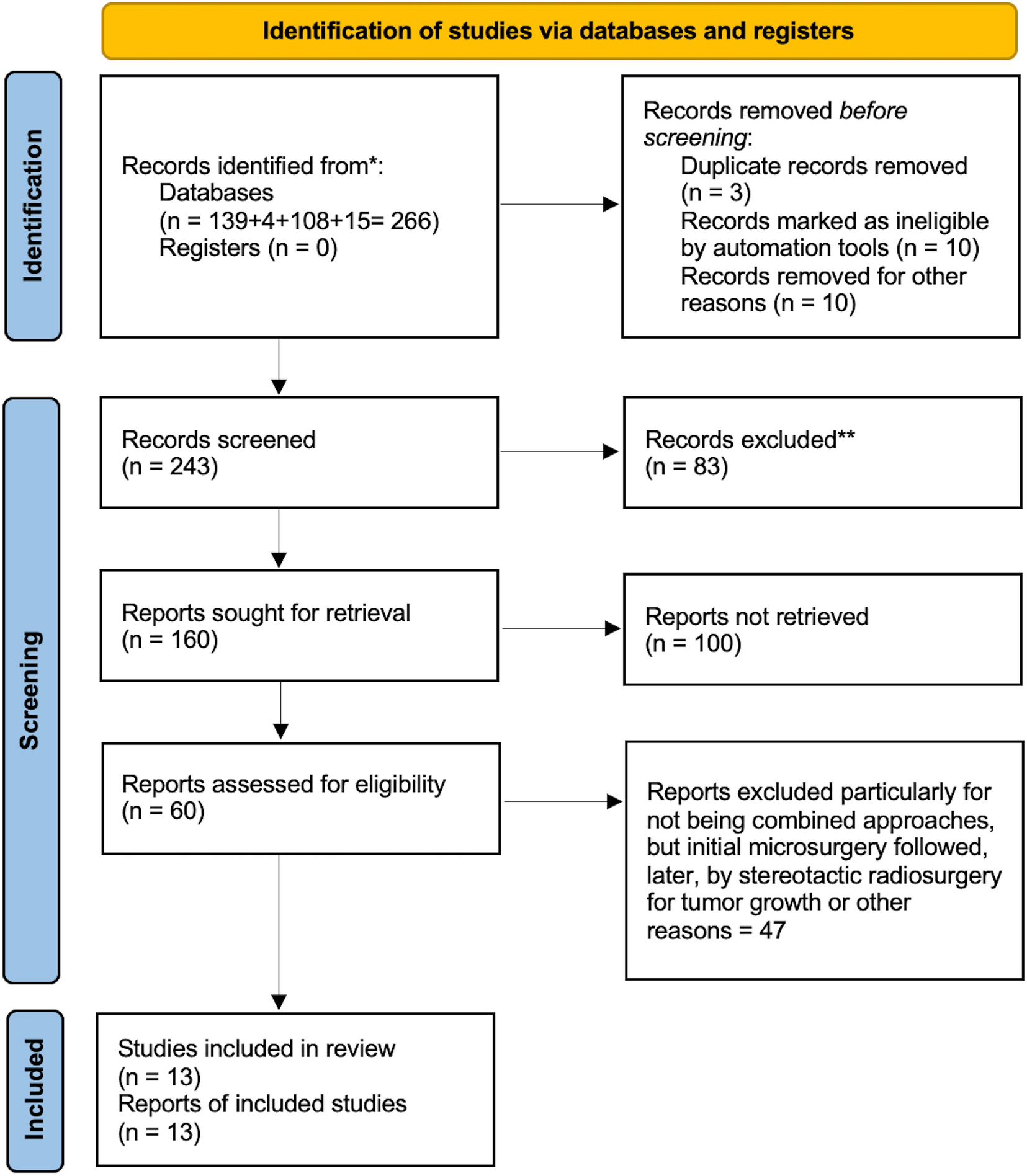
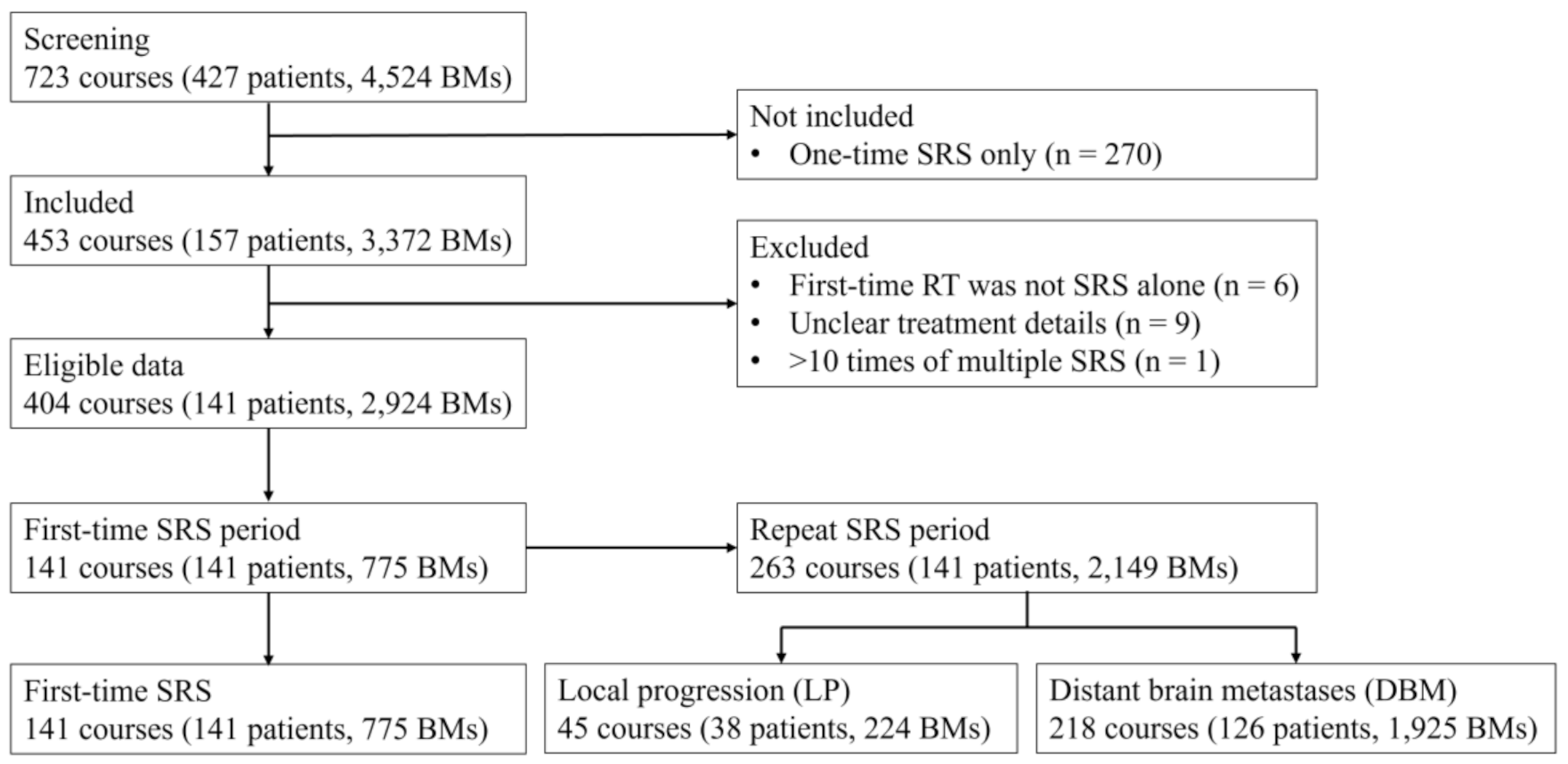
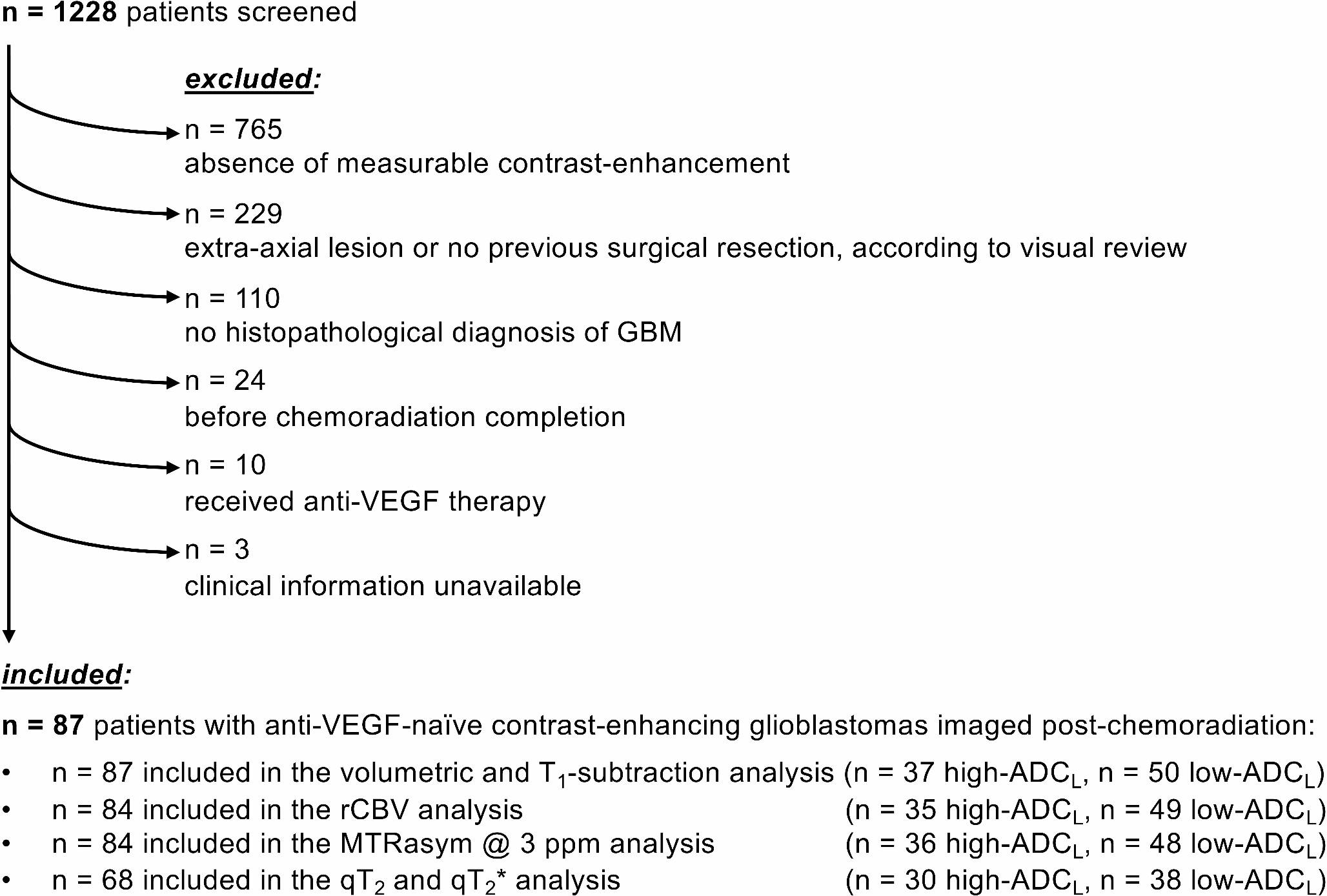
196 patients underwent surgery for radiologically suspected intracranial gliomas. Applying inclusion and exclusion criteria, the final collection includes 118 patients (Fig. 2). The population consisted of 78 males (66.1%) and 40 females (33.9%), with a mean age of 60.6 years (min = 18, max = 80). 82 patients were found to have HGGs (WHO 4, 69.5%), and 36 patients had LGGs (WHO 1,2,3, 30.5%). All details on patient demographics, clinics and group analysis are summarized in Table 1.
Radiological and clinical outcome
The mean tumor volume was 29.1 cm3 with no significant differences regarding grading (26.9 cm3 in HGGs, SD = 11.45 and 34.1 cm3 in LGGs, SD = 21.61, respectively, p = 0.22). The mean volume of PBE was 26.05 cm3, with a significant difference between HGG and LGG groups (28.8 cm3 SD = 2.42 versus 14.9 cm3 SD = 14.39, respectively, p = 0.05). There were no significant differences in tumor-edema ratio (310 versus 180, p = 0.25). The mean percentage of ki67 is 27%, with a significant difference between grading (35% in HGGs and 7.5% in LGGs, p < 0.001, respectively). EGFR is expressed in 18% of the population, and p53 was over-expressed in 25 patients (21.2%), both in the HGGs group. From the clinical outcome point of view, patients had a mean preoperative KPS of 85 with no significant difference in grading (85 for HGGs versus 90 for LGGs, p = 0.12). The mean KPS had significant differences between the two groups at postoperative, post-adjuvant therapy and at the last follow-up (65 versus 90), with HGGs presenting consistently lower values.
Analysis of DTI metrics
We examined the values of FAmean, FA max, FA min, MD, and TI grade in the BAT, comparing it with the surgical series’ clinical, radiological, and outcome parameters.
We identified that there is a significant inverse relationship between the FAmean value and grading (FA mean 0.313, SD = 0.11 for LGGs versus FA mean 0.218, SD = 0.007 for HGGs, p = 0.001), showing that a low-grade lesion is likely to result in more significant distortion/anisotropy of WM fibers than the aggressive HGGs (Fig. 3A).
In contrast, the relationship appears to be directly proportional regarding MD values (0.875 in LGGs, SD = 0.14 versus 1.767 in HGGs, SD = 0.71, p = 0.003, Fig. 3B) and TI values (8.44 in LGGs SD = 2.5 versus 11.14 in HGGs, SD = 2.2, p = 0.005, Fig. 3C).
In a multivariate analysis, FA mean, MD, and TI values are not influenced by the surgical site and tumor characteristics such as hemorrhage, necrosis, and cystic aspect (p = 1).
FA mean and MD values are susceptible to significant variations concerning tumor size and volume. Tumor volume correlate linearly with the value of FA (Pearson correlation= -0.360, p = 0.01). Edema volume correlate with the FAmean value (Pearson correlation = -0.351, p = 0.05) and MD value (Pearson correlation = 0.063, p = 0.05). In this evaluation, FA mean and MD values correlate with each other in a significant proportional manner (Pearson correlation=-0.516, p = 0.02).
Specific analysis for TI parameter
TI showed an independent relationship with the degree of aggressiveness of the tumor regardless of tumor radiological features and dimensions, with a direct relationship with grading, ki67% (p = 0,05), and PFS (p < 0.001, Fig. 3D).
In LGGs, there is a significant relationship between TI value and EOR, with a higher percentage of GTR for higher TI values (Mean 11.2 SD = 1.93 for GTR versus Mean 8.9 SD = 2.13 for NTR, p < 0.01). This is probably because high TI values correspond to areas of altered WM texture and density capable of guiding the surgeon into marginal resection. WM enveloping the tumor and distorting surrounding bundles in terms of evident high TI values also has a significant clinical impact on tumor onset with seizures (patients with clinical onset of seizure have TI mean 14.46 compared to focal onset or incidental diagnosis with TI mean = 7.98).
We identified an optimal cutoff value for TI of 10, suggesting a higher risk of reduced PFS and KPS in patients with a score values > 9.
To evaluate whether the TI value ≥10 is an independent prognosis-related factor, we conducted an independent prognostic analysis for the performance status and PFS for the two groups (group TI < 10 and group TI≥10). The prognostic analysis used univariate and multivariate Cox regressions.
The univariate prognostic analysis showed that the value of TI with threshold 10 was an independent factor affecting the prognosis (p < 0.001). The multivariate prognostic analysis showed that the TI≥10 (p = 0.02), EOR (p < 0.001) and tumor grading (p = 0.04) were independent factors affecting the prognosis. In the TI≥10 group of patients, both univariate and multivariate prognostic analysis showed that the risk score was an independent factor affecting the PFS and KPS after surgery (Fig. 4A and B, p < 0.05). In the model values we obtained a cross-validated area under curve (AUC) of 0.31, CI 95% (p = 0.03, DeLong’s test) and single-validation AUC for KPS after RT (or at 6 months clinical evaluation for LGG without post-operative RT (95% CI, 0.4– 0.78), 0.583 (p = 0.03, DeLong’s test) for KPS at the last evaluation (95% CI, 0.44– 0.76), 0.541 (p < 0.001, DeLong’s test) and PFS (95% CI, 0.37– 0.709 p < 0.01, Fig. 4C).
Furthermore, performing a binomial analysis for the achievement of GTR between the two groups, we observed that in cases where total tumor resection was achieved, the TI value measured in the BAT more frequently showed a TI value ≥10. This difference was significant (Pearson chi-square p = 0.048) and could be dependent on greater tumor aggressiveness (with a high correlation with the presence of intratumoral necrosis, (Fig. 4D).


Comments (0)