
Remember me

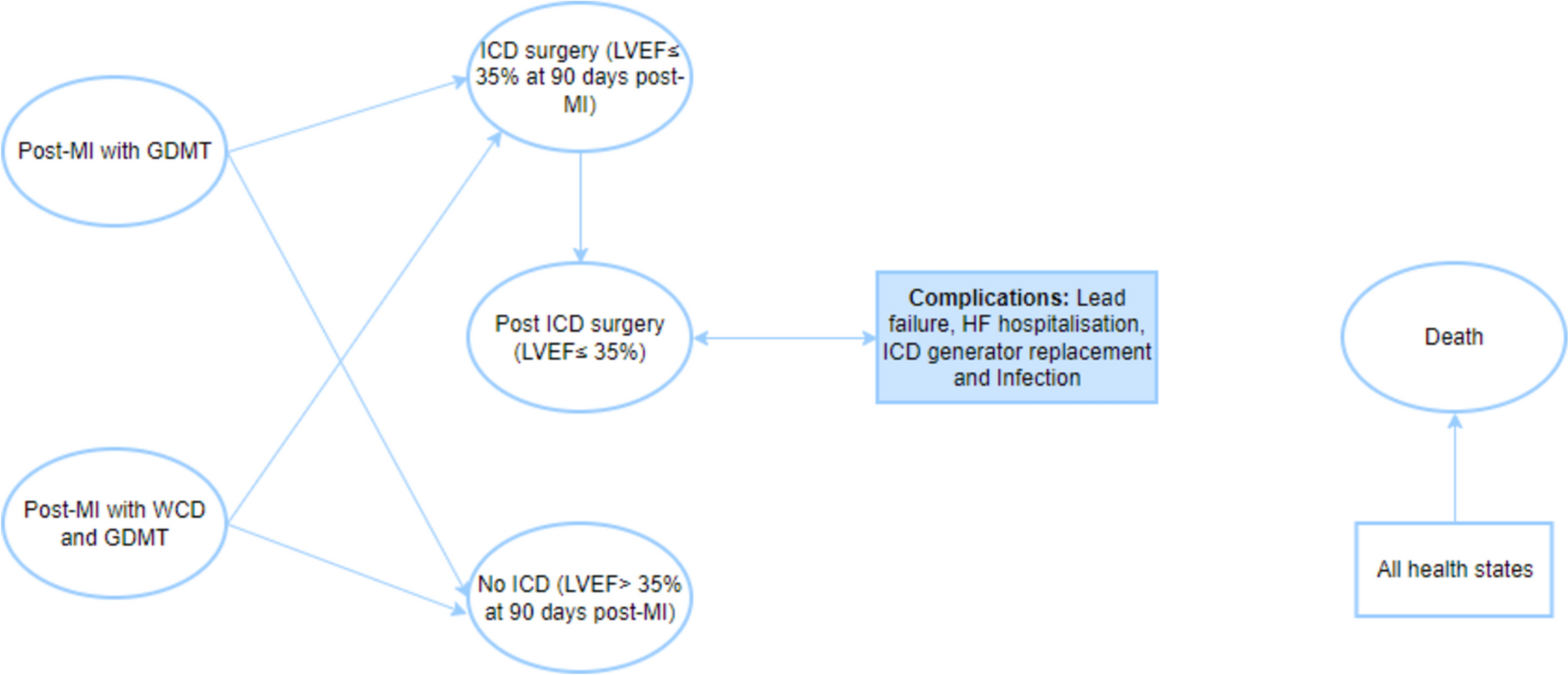

The budget impact model (BIM) provided by AstraZeneca was developed in Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA, USA); the model has been reviewed, validated and adapted to the Argentinian setting. Figure 1 displays the analytical structure of the model. The BIM considers a hypothetical third-party payer with 1,000,000 male individuals who were covered to estimate two scenarios: the current scenario (without olaparib) and the projected scenario (incorporation of olaparib). A comparison of the current and projected scenarios provided an estimate of the budget impact over a 5-year time horizon for the coverage of olaparib for the management of patients with HRR-mutated castration-resistant metastatic prostate cancer previously treated with NHA. The perspective of the analysis was the third-party public payer, the third-party social security payer, and the third-party private payer in the Argentinian health system. In Argentina, the healthcare system is decentralized and fragmented into three sectors: public, social security, and private. The social security sector is the largest and provides healthcare coverage to approximately 46% of the Argentine population, 16% are covered by the private sector, and approximately 38% of the population is covered by the public sector [17].
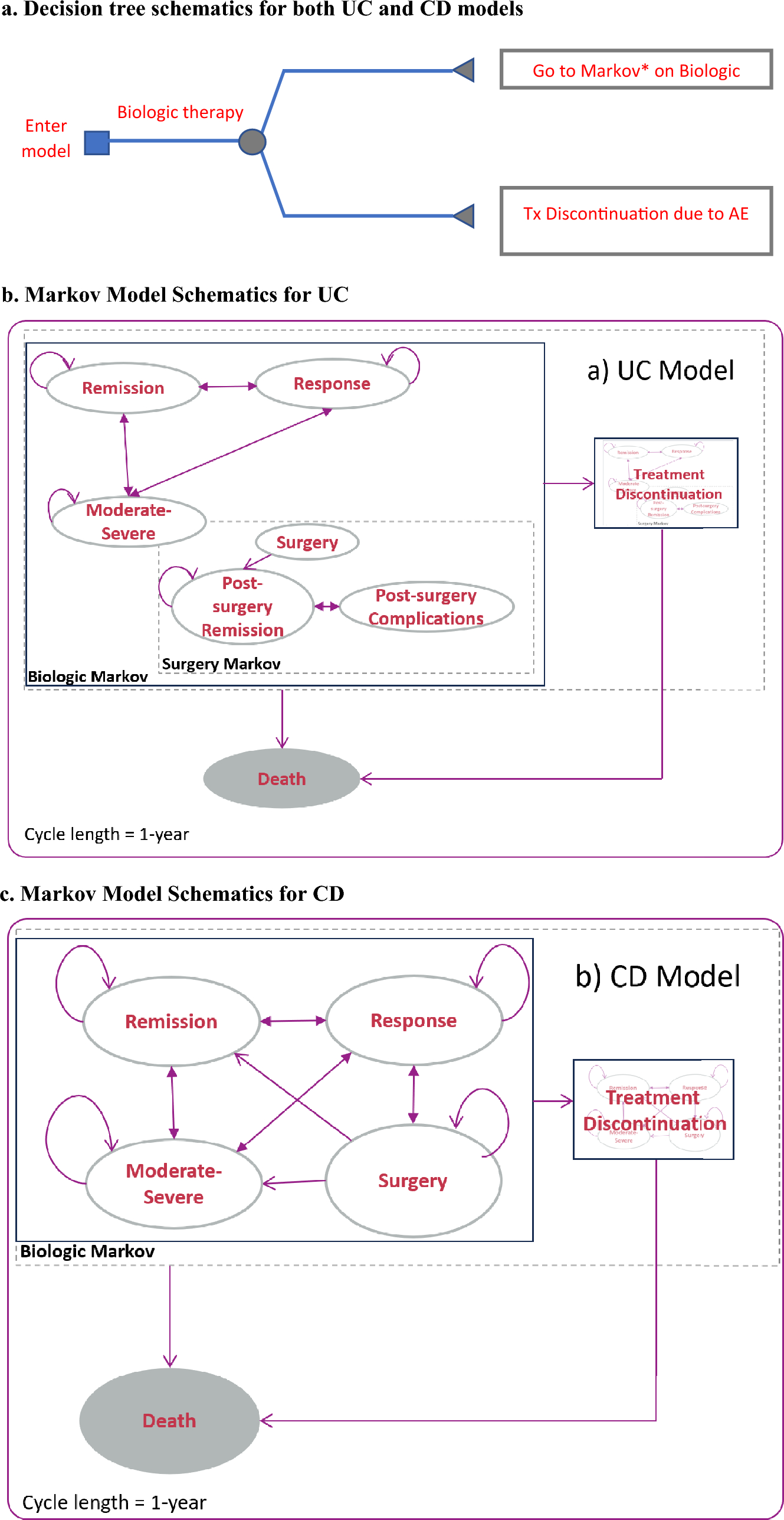
Fig. 1
Analytical structure of the model. mCRPC metastatic castration-resistant prostate cancer, NHA new hormonal agents, HRR homologous recombination repair gene
Budget impact outcomes were presented in absolute and relative terms and per member per month (PMPM) calculations. We followed the principles of good practice in budget impact modeling to elaborate this report, published by the Professional Society for Health Economics and Outcomes Research (ISPOR) task force [18]. The epidemiological data were sourced from the literature; however, for data not available in the literature, we consulted and validated the data with a local oncology expert.
2.2 Model AssumptionsThe incidence of prostate cancer was constant throughout the 5-year time horizon. For the current scenario, we assumed a constant market share for each treatment regimen. We also assumed that the access rate to olaparib for each healthcare sector was constant in the 5-year time horizon. Lastly, no discount rates or adjustment for inflation were considered.
2.3 Target PopulationMale patients with mCRPC whose disease had progressed during treatment with NHAs (enzalutamide or abiraterone) were included in the model. The incidence of prostate cancer was estimated to be 0.18% [1]. Of the total number of patients with prostate cancer, approximately 15% had metastatic prostate cancer resistant to castration [7]. Based on the local clinical oncologist expert opinion, approximately 60% of patients are treated with NHAs. Moreover, approximately 90% of prostate cancer patients progress to resistance, with the need to initiate a second line of treatment. It is estimated that 18% of patients will progress to mutated HRR (estimated based on data published by de Bono et al. [9], as mutations were detected in 778/4425 patients selected for screening), making them candidates for olaparib, and that 5.69 patients must be tested to identify one patient who tests positive for HRR [9]. Electronic supplementary material (ESM) S7 Fig. 3, presents the flowchart of prostate cancer patients eligible for olaparib treatment.
2.4 Intervention and ComparatorsThe intervention was olaparib monotherapy 300 mg twice daily. Comparators were chosen based on the clinical experience of the local oncologist expert. In Argentina, abiraterone, enzalutamide, cabazitaxel, and docetaxel are the currently commercialized and indicated therapies for patients with mCRPC whose disease has progressed during treatment with NHAs (enzalutamide or abiraterone). The dosages of the interventions and comparators were based on the published trial results [9, 19, 20].
2.5 Market ShareThe market share for each comparator and the intervention were calculated based on the opinions and projections provided by the local oncologist expert. In the current scenario, the olaparib market share was assumed to be zero.
The estimation of olaparib's market share penetration varies across different third-party payers, each attempting to capture the unique characteristics of the Argentine healthcare system in terms of high-cost drug access and coverage within distinct healthcare sectors. Based on local clinical expert opinion, the market penetration for olaparib during the first year was 7%, 25% and 32% for the third-party public payer, third-party social security payer, and third-party private payer, respectively. Market shares are reported in ESM Table S1.
2.6 Cost ComponentsDirect medical costs associated with treatment were considered for analysis, and included the acquisition costs of mCRPC drug treatments, administration costs, adverse event (AE) costs, monitoring costs, and HRR test costs. All costs were estimated in Argentinian pesos (ARS) and then converted to US dollars (US$) as at October 2022 (1 US$ = 152.59 ARS) [21].
The drug acquisition costs were obtained from public databases that report the retail price of drugs marketed in Argentina [22]. We used the most recent retail price to perform the analysis, and converted the retail prices to wholesale prices by applying the conversion factor (laboratory output price) suggested by the Argentinian Ministry of Economy [23]. For each drug, the total drug acquisition cost was estimated from the wholesale price, the dosage of the therapy administered, and the mean duration of treatment. For the estimation of treatment durations, 7.5 months was used for olaparib [9], 3.6 months was used for enzalutamide and abiraterone [9], 7 months was used for docetaxel [20], and 5.5 months was used for cabazitaxel [19]. It should be noted that the treatment durations for enzalutamide and abiraterone from the PROfound study were taken into account in order to homogenize the populations.
For all drugs, we assumed there was no wastage. We assumed that the drug acquisition costs were the same for the three perspectives of the analysis. For drugs administered according to weight, a mean patient weight of 80 kg was used [24]. The dosage, wholesale price per pack, and annual treatment costs per patient for olaparib and comparators are presented in Table 1.
Table 1 Dosage, wholesale price per pack, and annual treatment costs per patient for olaparib and comparators.The cost of each intravenous drug administration was obtained from the Institute for Clinical Effectiveness and Health Policy (IECS) unit cost database and is estimated for the third-party public payer, third-party social security payer, and third-party private payer at $72.54, $115.59, and $131.56, respectively [25]. This cost included the use of the oncologic room to administer the drugs. We assumed that oral administration has no cost.
The monitoring costs and costs of AEs were estimated using the microcosting approach. The identification, rate of use, and measurement of health resources used for disease management were estimated by the opinion of a local expert, the unit costs by health sector were obtained from the IECS unit cost database, and the drug acquisitions costs were obtained from public databases and converted to wholesale prices [22, 23, 25]. The health resources included medical consultations (oncologist), laboratory tests (blood count, testosterone, urea, creatinine, ionogram, hepatogram, and blood glucose) and images (chest computed tomography [CT] scan with contrast, and CT pelvis and abdomen with contrast). The cost of prednisone as an add-on drug to treatment with abiraterone, docetaxel and cabazitaxel was also considered. This cost was $5.95 per month. The unit cost per health resource and the quantities used in the monitoring costs are available in the ESM Tables S2 and S3.
On the other hand, the AEs included in the model were fatigue, hypertension, anemia, febrile neutropenia, thrombocytopenia, pneumonia, urinary tract infection, sepsis, pulmonary embolism, and vomiting. These AEs were grade 3/4 according to the Common Terminology Criteria for Adverse Events version 4 [26], and were in line with those reported in the clinical trials for each treatment [27,28,29]. The AEs excluded were dyspnea and asthenia, as their management does not require associated clinical practices. Prevalence rates per AEs are reported in ESM Table S4, and the monitoring costs and AE costs are presented in Table 2.
Table 2 Monthly monitoring costs per patient and adverse event costs, by healthcare sector.The cost of the HRR test for the private sector was obtained from a private laboratory in Argentina where the HRR test is currently performed, while the cost of the HRR test for the public and social security sectors were estimated by applying cost ratios between sectors, which were obtained from the IECS unit cost base [25]. We assumed a hypothetical scenario whereby all patients with mCRPC whose disease had progressed during treatment with NHAs are tested with HRR; there is no difference in the access rate by health sector. Finally, estimated HRR testing costs for the public, social security, and private sectors were $350.52, $673.27, and $680.00, respectively.
2.7 Decision Rule—Budgetary Impact ThresholdOur study employed the methodology utilized by the National Commission for Health Technology Assessment and Clinical Excellence of the Ministry of Health (CONETEC, acronym in Spanish), the local Health Technology Assessment, in the country to estimate a threshold of high budgetary impact. This approach is reported in the study by Pichon-Riviere and colleagues, which is particularly relevant for countries lacking their own estimates [30]. The reference value of the high budgetary impact threshold is estimated at 0.00016 health spending units (0.00008–0.00024). The estimation of the threshold of high budget impact in Argentina for 2022 was made using the reference value and updating the estimate of total health expenditure. The latter is estimated using the Gross Domestic Product (GDP) data and total population of Argentina, as well as the average of the last 10 available years of healthcare expenditure as a percentage of GDP [31, 32]. The threshold estimation was carried out for each healthcare sector using the per capita healthcare expenditures estimated and reported in the study by Espinola and colleagues [33]. Accordingly, it was estimated that the PMPM threshold of high budget impact was $0.0153 for the health system. In addition, the per capita healthcare expenditure values were used to quantify conversion factors and thus estimate the threshold of high budget impact for each healthcare sector. Therefore, the PMPM threshold of high budget impact was estimated at $0.0110 for the public sector, $0.0146 for social security, and $0.0261 for the private sector.
2.8 Sensitivity AnalysisTo evaluate the effect of uncertainty associated with the parameters of the model on the budget impact results, deterministic (one-way) sensitivity analyses (DSAs) for the base case were performed. The parameters varied from their default values by ±10%. For the cost of the intervention, a variation of ±25% was considered given the lack of information on its variability.
2.9 Scenario AnalysisAn alternative scenario was developed under the assumption that HRR testing is not accessible in the health system in Argentina, and consequently, it is necessary to have previously performed the BRCA test in order to provide olaparib. This scenario is not too distant from the reality in Argentina, given that the HRR is nowadays only available for a few private providers.
We estimated that 11% of the prostate cancer patients who progress to resistance will be BRCA receptor-positive, making them candidates for olaparib [9]. Moreover, 9.10 patients must be tested to identify one patient who tests positive for BRCA [9]. BRCA testing costs for the public sector, social security, and private sector were $351.24, $639.52, and $681.40, respectively. These costs were retrieved from the IECS unit cost database [25].
2.10 Model ValidationThe model structure and calculations were reviewed and validated by academic experts from the IECS, and all input parameters were initially reviewed and validated by a local oncologist expert. Suggestions for revision and/or adaptation were addressed prior to conducting the analysis.
Comments (0)