
Remember me


This work was a cost-utility analysis (CUA) performed alongside a retrospective cohort study, which focused on adult T2D patients who had previously been diagnosed with HF and exhibited a range of baseline New York Heart Association (NYHA) and left ventricular ejection fraction (LVEF) values. To represent T2D-HF patients in Thailand, this study used claims data from the National Health Security Office (NHSO), which is the largest universal coverage provider in Thailand, accounting for approximately 72% of the Thai population [12], for the period from 1 January 2015 to 31 December 2022. Patients entered the model at 60 years, reflecting the average age of Thai T2D-HF cases, which was approximately 62 years according to the NHSO databases.
2.2 Intervention and ComparatorThe potential intervention consisted of all available SGLT2i in Thailand, including dapagliflozin, empagliflozin, canagliflozin, and luseogliflozin. These agents were added to the SoC for T2D-HF patients. The SoC encompassed lifestyle modifications, rigorous glycemic and blood pressure control, and optimal medication management, including diuretic, angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs), β-blockers, and mineralocorticoid receptor agonists (MRAs). Dapagliflozin was approved for use in Thailand in 2014, whereas empagliflozin and canagliflozin were approved in 2015; however, luseogliflozin did not have randomized controlled trials (RCTs) conducted in T2D-HF patients and was therefore not included in the analysis. The SGLT2i group was developed to evaluate the cost-effectiveness of all available SGLT2i, excluding luseogliflozin, using our SRMA pooled efficacy data and the average price of all SGLT2i.
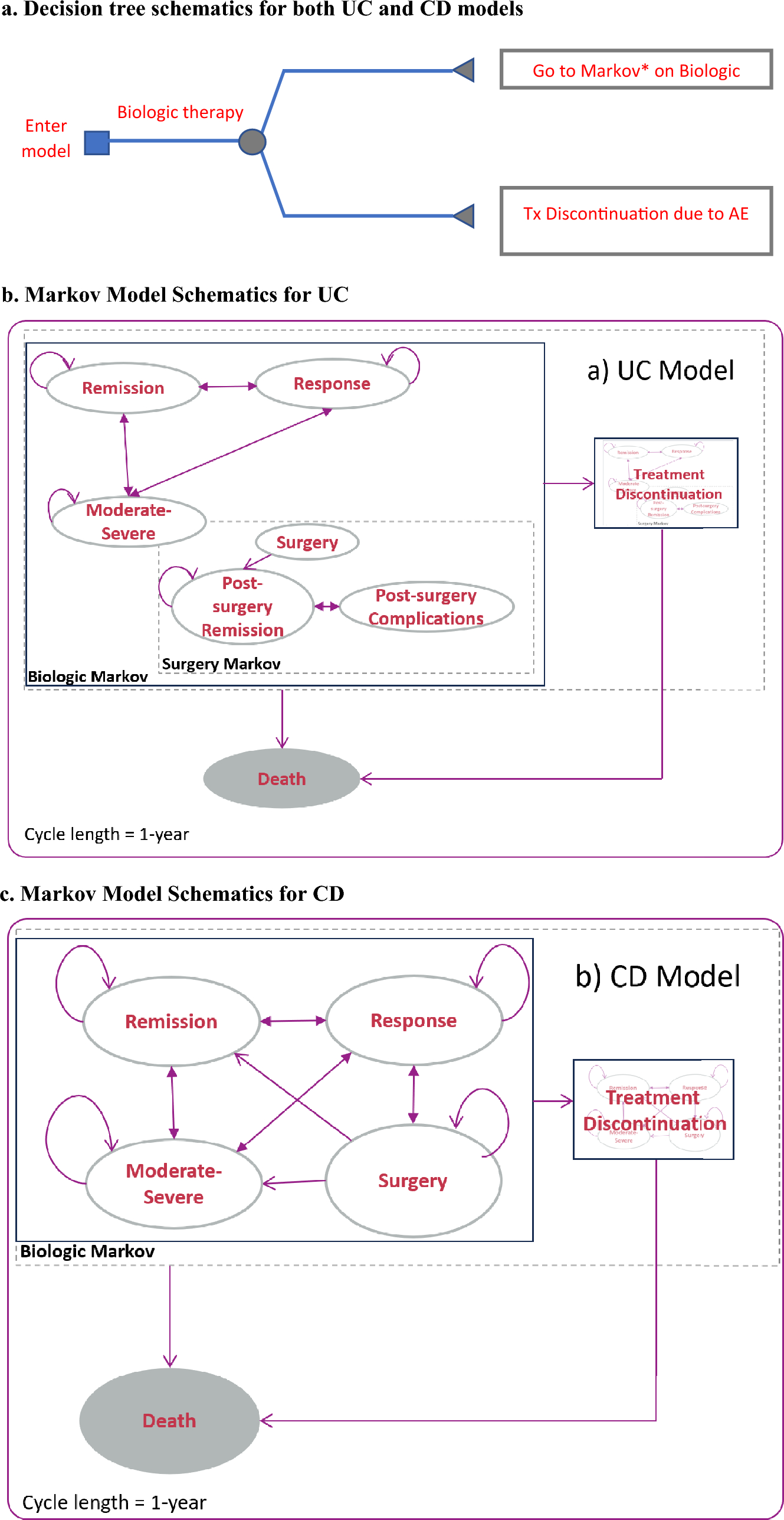
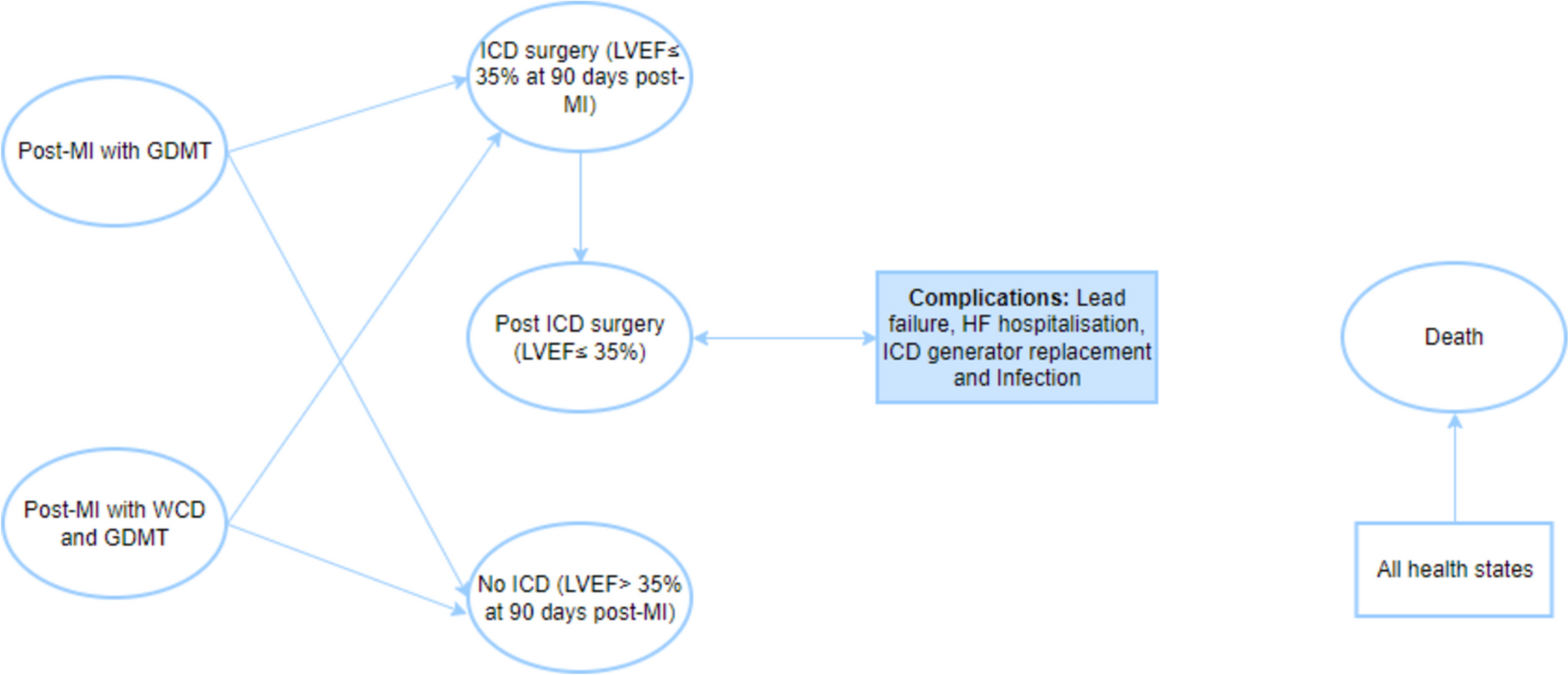
2.3 Model StructureA Markov model was constructed using a lifetime horizon from a societal perspective to predict the cost-utility of adding SGLT2i to the SoC compared with SoC alone in T2D-HF patients. The model is composed of three health states: stable HF (SHF), HFH, and all-cause death, as seen in Fig. 1. The study patients entered the model in the SHF state and could progress to HFH or death. Following a non-fatal HFH, individuals in the model population could either be at risk of a further HFH event (readmission within 90 days), return to SHF, or pass into death. Patients could transition between different health states every 3 months, which corresponds to the cycle length. These transitions continued until the end of a patient’s lifetime horizon. Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used to construct the model.
Fig. 1
A lifetime Markov model for type 2 diabetes patients with heart failure. The possible health states applied to both the standard of care alone and the standard of care plus sodium-glucose cotransporter-2 inhibitors. Cycle length of 3 months with a lifetime horizon
A number of assumptions were built into the model. First, T2D-HF patients received the SoC in order to manage their conditions. Second, patients did not experience adverse effects that would lead to drug discontinuation. Third, in the absence of real-world evidence based on transitional probabilities for both NYHA classification and LVEF values in the Thai HF population, a stratified analysis according to these factors could not be performed. Thus, we assumed that the efficacy, cost, and utility of patients in each health state were comparable.
Regarding the adverse effects of SGLT2i, a recent SRMA study [13] reported slight increases in the risk of urinary tract infections, genital infections, and diabetic ketoacidosis. However, these drugs were also able to significantly reduce the risk of serious adverse events and acute kidney injury [13]. Additionally, a real-world study in Thailand found that none of the patients developed diabetic ketoacidosis, while exhibiting low incidence rates for urinary tract infections and genital infections [14]. With little difference in the incidence of non-serious conditions at low treatment costs and only minimal impacts on patient utility, this study did not include the adverse effects of SGLT2i in its analysis.
2.4 Model Inputs2.4.1 Efficacy of Individual Sodium-Glucose Cotransporter-2 InhibitorsA systematic review and network meta-analysis (SRNMA) was conducted to assess and indirectly compare the efficacy and safety of individual SGLT2i following the Preferred Reporting Items for Systematic review and Meta-Analyses (PRISMA) statement [15]. This work was registered in PROSPERO (CRD42022353754). Three electronic databases, namely PubMed, Embase, and the Cochrane Central Registry of Controlled Trials, were searched from inception to 20 July 2023, without language restrictions. Search terms were constructed in accordance with the population, intervention, comparator, outcome, and study design format for each database, as described in Appendix A. Retrieved titles and abstracts were reviewed by two independent reviewers (TK and PH) and disagreements were discussed with a third reviewer (PL). RCTs or their subgroups and post-hoc analyses of SGLT2i in T2D-HF patients that compared SGLT2i with the SoC and had outcomes of interest were retained. The same two reviewers independently extracted the data. Stata (Stata Statistical Software: Release 17. StataCorp LLC, College Station, TX, USA) was used for all analyses and a significance threshold p-value of <0.05 was adopted.
A total of 7952 articles were retrieved, of which 14 articles from 11 studies were finally included (Appendix B). Characteristics for the included studies are shown in Appendix C. Because sotagliflozin and ertugliflozin were not available in Thailand during the study period, the SRNMA only pooled results for dapagliflozin, canagliflozin, and empagliflozin, which are registered for medical use in Thailand. An analysis of the treatment outcomes for T2D-HF patients using SGLT2i in conjunction with the SoC was conducted. The outcomes were measured in terms of HFH and all-cause mortality.
Our SRNMA demonstrates that the administration of any SGLT2i (e.g., dapagliflozin, canagliflozin, or empagliflozin) in addition to the SoC significantly reduces the HFH rate when compared with the SoC alone (relative risk [RR] 0.74, 95% CI 0.67–0.81, I2 = 25.23%). In addition, overall all-cause mortality is also significantly reduced (RR 0.91, 95% CI 0.84–0.98, I2 = 0.0%); however, only the dapagliflozin results showed statistical significance (Table 1).
Table 1 Transition probabilities and clinical efficacy parameters used in the model2.4.2 Transitional ProbabilitiesThe NHSO data were quality checked by ensuring that the visit date was not after the date of death, the age at the time of service increased over time, the date of admission was smaller or equal to the date of discharge, and there were no admissions to hospital after the date of death. Additionally, the length of stay in hospital was positive, the gender remained consistent each time, and duplicate, nested, or overlapping records were detected and corrected. For HFH, the initial index case was only determined from the visit of HFH patients to ensure the diagnosis of HFH. Patients with T2D-HF were included if they had International Classification of Diseases, Tenth Revision (ICD-10) codes E11.x and I50.x. The index date was the hospitalization date with HF. Patients who died before the next visit or lacked follow-up after discharge were excluded. SHF was defined as no urgent care or HFH within 3 months post-discharge. A parametric survival model with the Weibull or Gompertz distribution was applied to estimate the transitional probabilities for SHF → HFH, SHF → death, and HFH → death using NHSO data covering 120,861 T2D-HF patients. The model fitting was tested using Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) values to compare Gompertz and Weibull distributions. The distribution with the lower AIC and BIC values was considered to provide a better statistical fit to the data. This approach ensures that the selected distribution minimizes information loss and avoids overfitting, thereby optimizing the model’s predictive performance. Stata was used for the survival analysis, as detailed in Appendix D. The baseline characteristics of the cohort population are shown in Appendix E.
2.4.3 CostThe Thai Health Technology Assessment (HTA) guidelines suggest employing a societal perspective when conducting economic evaluations, both to determine the impact of new interventions and to consider the inclusion of those interventions in the national benefits packages [16]. This approach makes use of direct medical costs and direct non-medical costs in the analysis, while indirect costs were excluded to avoid duplication of both expenses and impacts from the interventions. The direct medical costs for T2D-HF treatments include the cost of a patient’s care and any drug prescriptions. The treatment costs for outpatient department (OPD) visits and inpatient department (IPD) care were obtained from claims data in the NHSO database, tracking health coverage for the largest segment (72%) of Thailand’s population [12], from 1 January 2015 to 31 December 2022. The prices of all SGLT2i were derived from the Drug and Medical Supply Information Center (DMSIC) website, which is maintained by the Ministry of Public Health [17]. Based on the doses administered in the clinical trials [18,19,20,21], the daily doses in this study included dapagliflozin 10 mg/day, canagliflozin 100 mg/day, and empagliflozin 10 mg/day.
Direct non-medical costs, including accommodation, supplements, informal care, medical equipment, and home renovation, were obtained through interviews with patients or caregivers who had visited or were hospitalized at hospital from 1 October 2022 to 31 March 2023 (n = 54), using a structured questionnaire. Travel, food, and caregiver’s productivity loss costs were acquired from the current reference unit of the standard cost list for Thailand’s HTA [22]. The costs were adjusted to the year 2022 using the Consumer Price Index (CPI) in the corresponding medical care categories [23] and were converted to US$ with an exchange rate of 35.06 THB per US$ [24]. Based on Thailand’s HTA guidelines, a discount rate of 3% per year was applied [16]. All cost data are shown in Table 2.
Table 2 Cost and utility parameters used in the model2.4.4 UtilityThe Thai value set for EQ-5D-5L questionnaire (registration ID 59225) [25] was used to prospectively assess the utility of each health state in T2D-HF patients treated at hospital. The sample size was calculated using the formula [26] n = [Z2ασ2]/e2, where mean and standard deviation (SD) values were used from previous studies [27, 28]. A total of 23 SHF patients were interviewed, of whom the mean age was 74.1 ± 10.9 years and 72% were female. Additionally, 80% had hypertension, 50% had dyslipidemia, and 16% had a history of stroke. Mean duration of T2D was 4.7 ± 2.1 years, with an average HbA1C level of 7.4 ± 1.2%. Furthermore, 77.7% of the patients were classified as NYHA class II and the average LVEF value was 63.2 ± 11.2%.
For the HFH health state, 31 patients were prospectively interviewed. These study participants had an average age of 73.5 ± 10.7 years, with 37% being female. Among these patients, 77% had coexisting hypertension, 23% had dyslipidemia, 3% had a history of stroke, and 20% had coronary artery disease. The average HbA1C level was 7.3 ± 1.6%. Additionally, 44.4% of patients were classified as NYHA class III and the average LVEF value was 53.7 ± 15.3%. The utility data were derived from a sample that included a typical distribution of comorbidities seen in the broader T2D-HF population [3], ensuring that the utility scores reflect real-world patient conditions.
2.5 Uncertainty AnalysisTo measure the level of confidence in the incremental cost-effectiveness ratio (ICER) and analyze the uncertainty in key model input parameters, univariate, scenario, and probabilistic sensitivity analysis (PSA) methods were applied. The influence of parameter uncertainty was assessed by one-way sensitivity analysis, which uses the lower and upper bounds of parameter distributions to reveal the important ICER value determinants.
The scenario analysis was conducted to evaluate the use of utility scores from a literature review as opposed to those obtained through direct interviews. Because our hospital is a tertiary hospital, participants may have more severe diseases and multiple comorbidities. The utility results might be lower than those from hospitals at other levels of health care and might not fully represent the entire country. However, no previous utility scores were reported in Thailand; thus, we applied utility scores from the literature review. The EQ-5D questionnaire was used to measure the utility of T2D patients with HF in the United States during the Translating Research Into Action for Diabetes (TIRAD) study, which reported a utility (mean±SD) of 0.72 ± 0.21 [27]. This was compared with the utility obtained from our cohort (0.64 ± 0.38). The utility of patients with HFH was derived from a post-hoc analysis of the ASCEND-HF trial, which reported a utility (mean±SD) of 0.56 ± 0.23 [28], compared with the direct interviews of participants in our cohort, which reported a utility of 0.40 ± 0.39 for HFH.
For the PSA, 1000 iterations of a second-order Monte Carlo simulation were performed. Beta distribution was used for parameters that ranged from 0 to 1, such as probabilities and utilities. For cost parameters that had positive values, a gamma distribution was employed. For RR parameters, a log-normal distribution was applied. The discount rate varied from 0 to 6% based on Thailand’s HTA guidelines [16].
2.6 Budget Impact AnalysisBudget impact analysis (BIA) is conducted to forecast the financial implications from the government’s perspective if SGLT2i are included in the NLEM for the treatment of T2D patients with HF. This study assumes that upon inclusion in the NLEM, all T2D-HF patients aged 60 years and above will have access to the treatment.
2.7 Study ProcessWe organized two expert meetings to scope and verify the results of our study. The committee included cardiologists, endocrinologists, diabetologists, modeling experts, representatives from pharmaceutical companies, and representatives from governmental institutions in Thailand. The first meeting was held to finalize the model, define the scope of the study, and identify input parameter sources, while the second meeting was conducted to assess and validate the preliminary results. We incorporated all valuable comments from the experts to refine and strengthen our study.
2.8 Compliance with Ethics GuidelinesThis study retrospectively reviewed data from the NHSO database to calculate transitional probability and direct medical cost values. Direct non-medical cost and utility were prospectively collected through interviews with patients or caregivers. The study protocol was approved by the Institutional Review Board of our hospital (MU-MOU CoA 628/2022 and MU-MOU CoA 650/2023). Informed consent agreements were obtained from all participants.
Comments (0)