
Remember me










Because of the large heterogeneity of prostate carcinoma (PCa) some patients may have an indolent disease without any progress in the patients’ lifetime while in others, the disease could have a very aggressive and lethal course [1]. Active surveillance is an optional approach for patients with very low- or low-risk PCa. This approach aims to distinguish patients with a latent, slow-progressing disease who would not benefit from any active therapy, from those with progressive disease, in whom early active treatment would prolong their survival. For localized PCa, therapeutic options include radical prostatectomy (RP) or definitive radiotherapy (RT). Both of them have comparable outcome but differ mainly in acute and late toxicity [2]. In 25%–33% patients after RP, relapse occurs later in the course of the disease [3, 4]. The risk of relapse after RP increases up to 50%–80% in patients with positive surgical margin (PSM), pT3a-extraprostatic extension (EPE), pT3b-seminal vesicle invasion (SVI), pathologically proven pelvic nodal involvement, and Gleason score (GS) 8–10/International Society of Urological Pathology (ISUP) Group 4–5 [5, 6].
Risk Status After Radical ProstatectomyAdjuvant Radiotherapy as a Standard of CareFor a long time, adjuvant radiotherapy (ART) with or without androgen deprivation therapy (ADT) has been the standard of care for patients with the above-mentioned risk factors. The effects of ART have been studied in four major prospective trials (EORTC 22911, SWOG 8794, ARO96-02, FP-FINROG-0301), several smaller studies, and their meta-analyses [5, 7–10]. The benefit of ART has been consistently demonstrated only for biochemical relapse-free survival (bRFS) (hazard ratio - HR 0.47, p < 0.001) and locoregional relapse-free survival (lrRFS) (HR 0.54, p < 0.001). The studies and their meta-analysis also demonstrated higher overall toxicity (between 11% and 18% of patients) and severe genitourinary (GU) and gastrointestinal (GI) toxicity of ≥ Grade 3 (G3) by 1%–17% in the ART group compared to control arm [7]. The interpretation of the major four trials and their meta-analysis is complicated by inconsistent inclusion criteria, especially where staging and the requirement of a prostate-specific antigen (PSA) decline to zero after RP are concerned. The requirement of a zero PSA value after RP was implemented only in the ARO 96-02 study; the other three studies included 30%–70% of patients with PSA persistence [5, 7–10]. Besides, older techniques (2D or 3D RT) with nowadays insufficient doses (60 Gy) complicate the overall assessment of the results. Although the toxicity of multimodal therapy is significantly higher, neither individual studies examining the benefit of ART nor their subsequent meta-analysis have demonstrated a clear benefit of this therapy regarding overall survival (OS) and cancer-specific survival (CSS). The risk of overtreatment with ART is estimated by some authors to be as much as 35%–60% [7]. The results of another meta-analysis by Tao et al., which evaluated 15 smaller retrospective studies with a cumulative total of 5.586 patients, demonstrated a statistically significant benefit of ART versus salvage radiation therapy (SRT) in both 5 and 10 years bRFS and 5 years OS [4]. Based on these studies and their meta-analyses, the attitude towards ART and SRT remains inconsistent both among and within professional societies. While the European Society of Clinical Oncology (ESMO) no longer recommends ART as standard therapy, the recommendations of the European Urological Association (EAU) and the American Society of Clinical Oncology (ASCO), American Society for Radiation Oncology (ASTRO), and American Urological Association (AUA) remain more restrained in their recommendations and advocate considering ART after RP to patients with risk factors [2, 6, 11].
Paradigm Shift From ART to SRTBoth ART and SRT aim to eradicate the microscopic disease that may lead to future macroscopic relapse. SRT, unlike ART, is indicated if PSA exceeds 0.2 ng/mL from postoperatively undetectable values (PSA-recurrence or biochemical relapse [BCR]; occurs in approx. 27% of patients after RP) or if PSA levels persist at ≥ 0.1 ng/mL for 4–8 weeks after RP (PSA-persistence, in 5%–20% of patients) [5, 6, 12]. The need for adequate assessment of the role of ART has been recently fulfilled with published results of head-to-head studies, comparing the effect of ART to that of SRT (RADICALS-RT, TROG 08.03/ANZUP RAVES, GETUG-AFU 17) and their meta-analysis (ARTISTIC) [3, 13–15]. The RADICALS–RT trial, conducted at several European, UK, and Canadian centers, randomized a total of 1,396 patients with risk factors for recurrence in a 1:1 ratio to groups with immediate ART after RP and a group referred for SRT when PSA rose again above 0.4 ng/mL. With a median follow-up of 4.9 years, the OS and metastasis-free survival (MFS) data have not been sufficiently mature at the time of publication. While this study reported a significant reduction in GU and GI toxicity due to SRT and improved patient-reported Quality of Life (QoL) in the SRT arm, it failed to show any difference in the 5 years bRFS (85% for ART vs. 88% for SRT, p = 0.56) [13]. The Australian TROG 08.03/ANZUP RAVES trial, which randomized 333 patients, demonstrated a 5 years bRFS survival in 86% of patients in the ART arm and 87% in the SRT arm, respectively, thus demonstrating non-inferiority of SRT (HR 1.12, pnon-inferiority = 0.15), along with a significant absolute reduction in GU toxicity ≥ Grade 2 (G2) by 16% [3]. The third study was the French GETUG-AFU trial 17, which randomized 424 patients to ART or SRT in conjunction with a 6 months ADT with triptorelin. This study found no significant difference in the 5 years event-free survival (EFS) (92% in the ART arm and 90% in the SRT respectively, HR 0.81, p = 0.42), again with the significant benefit of lower acute and late toxicity in the SRT arm (by approx. 20% absolute) [14]. The ARTISTIC meta-analysis confirmed no benefit in EFS (HR 0.95, p = 0.7) for ART, thus shifting the therapeutic paradigm towards early SRT [15]. Table 1 summarizes the characteristics and results of the main phase 3 studies with 1:1 randomization to ART and WW (EORTC 22911, SWOG 8794, ARO96-02, FP-FINROG-0301) and studies with randomization into ART and SRT arm (RADICALS-RT, TROG 08.03/ANZUP RAVES, GETUG-AFU 17).
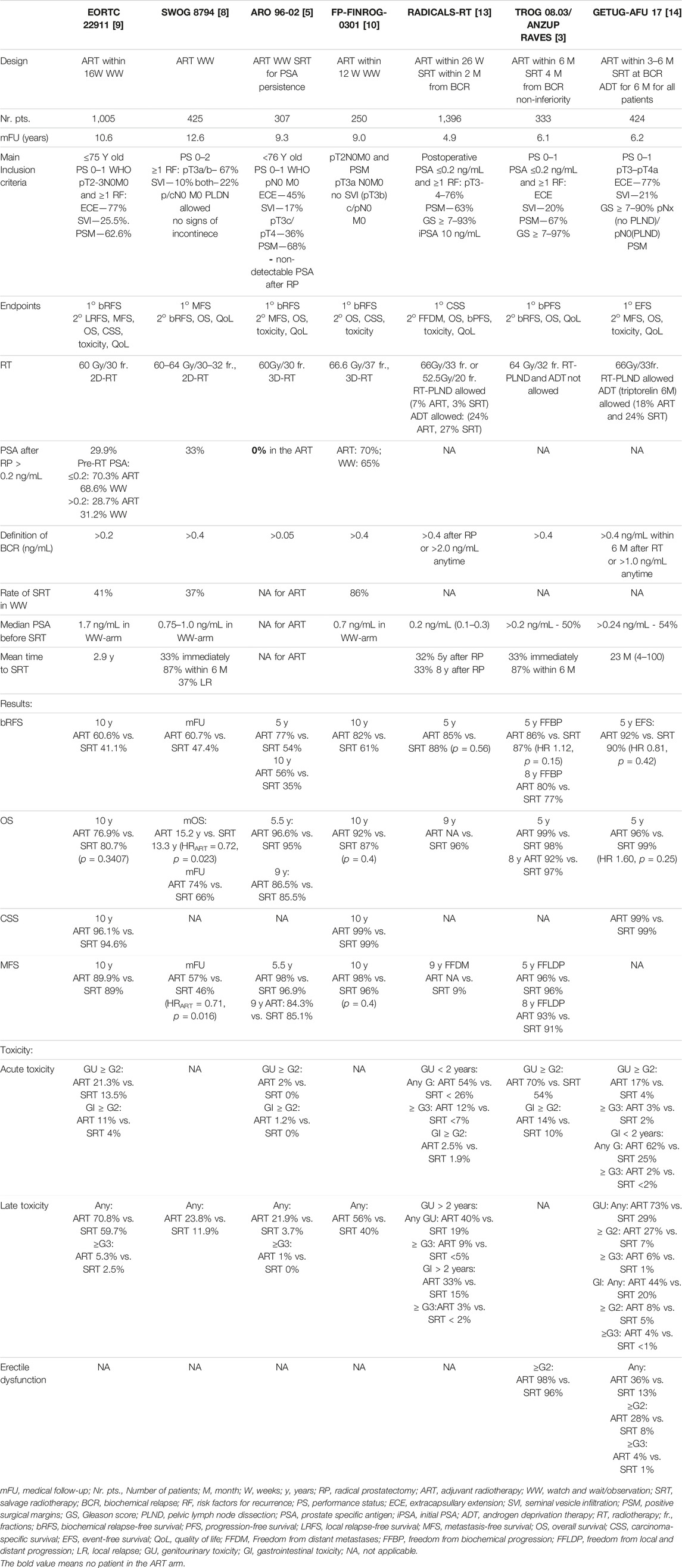
TABLE 1. Characteristics of the principal prospective studies focusing on ART versus SRT.
Addition of ADT to SRTThe basis for combining SRT with ADT was laid by two main studies. The RTOG 9601 trial that compared survival in men with PSA persistence or recurrence (PSA 0.2–0.4 ng/mL) after RP and with high-risk factors for relapse, in whom SRT (64.8 Gy) was indicated with or without a 2 years ADT with bicalutamide, 150 mg/day. At a 13 years follow-up, the group with ADT addition demonstrated a statistically significant improvement in 12 years OS (76.3% vs. 71.3%, HR 0.77, p = 0.04) and an 8.5% reduction in 12 years mortality due to prostate cancer (14.5% vs. 23.0%, p = 0.005), with no other statistically significant increase in toxicity except for gynecomastia (67.9% vs. 10.9%, p < 0.001). A subgroup analyses revealed that the greatest benefit from the addition of ADT was observed in patients with pre-SRT PSA levels >0.7 ng/mL, GS 8–10, and PSM [16]. The French GETUG-AFU 16 trial compared the effect of the addition of short-term ADT with gosereline for 6 months to the SRT therapy (66 Gy) in 743 patients with high-risk factors for relapse and pre-SRT PSA of 0.2–2 ng/mL after RP. In that study, no statistically significant benefit for overall survival was demonstrated, nevertheless, a significant reduction in 5 years bPFS (80% vs. 62%, HR 0.5, p < 0.0001) as well as a reduction in MFS (HR 0.73, p = 0.034) was demonstrated in the ADT group with no significant increase in late toxicity. A 112 months follow-up demonstrated that the addition of short-term ADT leads to persistent reduction of biochemical progression 10 years bPFS (64% vs. 49%, HR 0.54, p < 0.0001) compared with SRT alone [17, 18]. Based on a retrospective analysis of 1,125 patients and the main factors of clinical recurrence (≥pT3b, GS ≥ 8 and pre-SRT PSA > 5 ng/mL), Fossati et al. recommended the administration of short-term ADT (for one risk factor, RF) or long-term ADT (for two or more RFs) [6, 19]. The results from a study by Dess et al. suggested that pre-SRT PSA level > 0.6 ng/mL should be a prognostic biomarker for OS-benefit of ADT administered with SRT [20]. Although the data available so far, do not prove the necessity of the addition of standard ADT to SRT, they suggest that it might be considered especially in patients with the abovementioned risk factors.
Prognostic and Predictive Tools for SRTIn patients with PSA persistence, who have a worse prognosis compared to those with PSA recurrence, biochemical progression occurs in 50%–75%, but only about one-third of them develop distant metastases within 3 years of RP and almost 40% of them remain free of distant metastases even after 7 years [10, 12, 21–24]. Due to the aforementioned risk of overtreatment of ART, it has been suggested that approximately one–third to one-half of patients with PSA recurrence may not need RT at all or at least not so early considering all the consequences [7]. These assumptions are supported by sub-analyses of the RADICALS-RT study, according to which only one-third of patients in the SRT arm were indicated for therapy within 8 years of RP [7, 13, 24]. Results of other studies imply that only 30% of BCR patients manifest clinically and only 16% of them die of PCa progression [25–27]. Based on a meta-analysis of 77 studies with nearly 45,000 patients, the following clinical risk factors were identified as the primary negative prognostic factors for long-term survival: short PSA doubling time (PSA-DT), high postoperative GS, and short interval to biochemical relapse (IBR) [25]. The European Urological Association (EUA) has defined two risk groups for recurrence after RP—namely, a low-risk group (PSA-doubling time [PSA-DT] > 1 year and pathological GS < 8 and IBR > 18 months) and a high-risk group (PSA-DT < 1 year, pathological GS 8–10 and IBR < 18 months). Thus, the combination of parameters such as PSA-DT >1 year, BCR >3 years, stage ≤ pT3a, and ISUP grade 2/3 may help indicate postponing SRT while maintaining regular follow-ups [6, 25, 27]. Thus, all predictive tools that we have today, are based only on histological and biochemical parameters.
Advances in tumor-agnostic approaches in other cancers (e.g., melanoma or lung cancer), as well as the imperfect risk stratification leads to efforts to find molecular predictors that could, in combination with clinical factors, better stratify BCR patients according to the risk of clinical relapse, and thus help optimize therapy. These efforts have led to the development of three commercial multigene assays (Oncotype DX® Prostate Cancer Assay Decipher®Test, Prolaris Cell Cycle Progression Assay), which differ significantly from each other. They have not entered routine clinical practice due to lacking validation on large patient population [28].
A meta-analysis of ten trials showed a significant improvement in 5 years bRFS in the group of patients with pre-SRT PSA < 0.5 ng/mL, compared with patients with pre-SRT PSA > 0.5 ng/mL [29]. By the pre-SRT PSA level of 0.5 ng/mL, the chance of re-achieving non-detectable PSA levels after SRT is approximately 60%; a chance for a 5 years RFS is as much as 80% [29, 30]. Abugharib et al. studied 657 patients with SRT and proved a strong correlation of pre-SRT PSA levels with the effect of early SRT. In their study, the groups with pre-SRT PSA of 0.01–0.2, 0.2–0.5, and >0.5 ng/mL, respectively, showed gradually worse 10y-bRFS (62%, 44%, 27%, respectively), MFS (86%, 79%, 66% respectively), and CSS (93%,89%, 80% respectively) with the increasing pre-SRT levels [21]. According to the recommendations, the most appropriate pre-SRT PSA level for initiating SRT is up to 0.4–0.5 ng/mL, as patients with PSA > 0.5 ng/mL are at higher risk of distant dissemination [2, 6, 21]. Nevertheless, the questions of the appropriate timing of early SRT as well as the necessity of ADT and its duration remain largely unanswered.
DiscussionThe purpose of our overview was to summarize contemporary approaches to the patients with high risk (50%–80%) of recurrence after RP. Published studies suggest that one to two-thirds of patients will benefit from subsequent ART or SRT. Because of the large inter- and intra-tumoral heterogeneity of PCa, it has been suggested that at least one-third of these patients may be spared further multimodal therapy and the resulting consequences such as GU and GI toxicity.
A randomized phase III trial ESTABLISH (NCT05232578) that may clarify the need for early salvage radiotherapy in patients with BCR after RP with high-risk factors for relapse in the “gray zone” of PSA value 0.2–0.5 ng/ml has been initiated in the Czech Republic. Current prognostic and predictive factors based only on clinical parameters (stage, GS, PSA, PSA-DT, IBR) are insufficient for accurate stratification of patients to multimodal therapy. Clear predictive and prognostic molecular genetic tests facilitating this stratification and the choice and timing of the therapy for an individual patient have not yet been established in clinical practice. It seems, that the interplay of clinical and molecular prediction could be the right key to an accurate patient-oriented therapy. The suitability or even necessity of initiating early SRT and its balancing with associated toxicity in the PSA range 0.2–0.5 ng/mL remains an unresolved “grey zone” that poses a challenge in everyday clinical practice.
Author ContributionsSA, MV, OC, and LL have participated in the conception and design of the review, SA reviewed the literature and wrote the first draft of the manuscript, MV, OC, and LL participated on preparing of the manuscript. All authors contributed to the article and approved the submitted version.
FundingThis article was supported by the Ministry of Health of the Czech Republic (MH CZ-DRO, General University Hospital in Prague—VFN, 00064165) and by institutional funding of the Charles University in Prague (Cooperatio, Medical Diagnostics and Basic Medical Sciences, Oncology and Haematology).
Conflict of InterestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
AcknowledgmentsWe would like to express our special thanks to Prof. MUDr. Luboš Petruželka, CSc. for his stimulating input, guidance, and final critical review of our manuscript. We thank our colleagues at work and coworkers for their personal and administrative support.
References2. Parker, C, Castro, E, Fizazi, K, Heidenreich, A, Ost, P, Procopio, G, et al. Prostate Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol (2020) 31:1119–34. doi:10.1016/j.annonc.2020.06.011
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Kneebone, A, Fraser-Browne, C, Duchesne, GM, Fisher, R, Frydenberg, M, Herschtal, A, et al. Adjuvant Radiotherapy Versus Early Salvage Radiotherapy Following Radical Prostatectomy (TROG 08.03/ANZUP RAVES): A Randomised, Controlled, Phase 3, Non-Inferiority Trial. Lancet Oncol (2020) 21:1331–40. doi:10.1016/s1470-2045(20)30456-3
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Tao, R, Dai, J, Bai, Y, Yang, J, Sun, G, Zhang, X, et al. The Prognosis Benefits of Adjuvant versus Salvage Radiotherapy for Patients After Radical Prostatectomy With Adverse Pathological Features: A Systematic Review and Meta-Analysis. Radiat Oncol (2019) 14:197. doi:10.1186/s13014-019-1384-z
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Wiegel, T, Bartkowiak, D, Bottke, D, Bronner, C, Steiner, U, Siegmann, A, et al. Adjuvant Radiotherapy Versus Wait-And-See After Radical Prostatectomy: 10-Year Follow-Up of the ARO 96-02/AUO AP 09/95 Trial. Eur Urol (2014) 66:243–50. doi:10.1016/j.eururo.2014.03.011
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Mottet, N, van den Bergh, RCN, and Briers, E EAU-EANM- ESTRO-ESUR-SIOG Guidelines on Prostate Cancer 2020. In: European Association of Urology Guidelines. Arnhem, The Netherlands: European Association of Urology Guidelines Office (2020).
7. Bhindi, B, Lokeshwar, SD, Klaassen, Z, Klotz, L, and Wallis, CJ. Systematic Review and Meta-Analysis of Trials Evaluating the Role of Adjuvant Radiation After Radical Prostatectomy for Prostate Cancer: Implications for Early Salvage. Can Urol Assoc J (2020) 14:330–6. doi:10.5489/cuaj.6440
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Thompson, IM, Tangen, CM, Paradelo, J, Lucia, MS, Miller, G, Troyer, D, et al. Adjuvant Radiotherapy for Pathological T3N0M0 Prostate Cancer Significantly Reduces Risk of Metastases and Improves Survival: Long-Term Followup of a Randomized Clinical Trial. J Urol (2009) 181:956–62. doi:10.1016/j.juro.2008.11.032
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Bolla, M, van Poppel, H, Tombal, B, Vekemans, K, Da Pozzo, L, de Reijke, TM, et al. Postoperative Radiotherapy After Radical Prostatectomy for High-Risk Prostate Cancer: Long-Term Results of a Randomised Controlled Trial (EORTC Trial 22911). The Lancet (2012) 380:2018–27. doi:10.1016/s0140-6736(12)61253-7
CrossRef Full Text | Google Scholar
10. Hackman, G, Taari, K, Tammela, TL, Matikainen, M, Kouri, M, Joensuu, T, et al. FinnProstate Group: Randomised Trial of Adjuvant Radiotherapy Following Radical Prostatectomy Versus Radical Prostatectomy Alone in Prostate Cancer Patients With Positive Margins or Extracapsular Extension. Eur Urol (2019) 76:586–95. doi:10.1016/j.eururo.2019.07.001
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Sanda, MG, Cadeddu, JA, Kirkby, E, Chen, RC, Crispino, T, Fontanarosa, J, et al. Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline. Part II: Recommended Approaches and Details of Specific Care Options. J Urol (2018) 199:990–7. doi:10.1016/j.juro.2018.01.002
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Plousard, G, Staerman, F, and Pierrevelcin, J. Committee of Cancerology of the Association of French Urology. Predictive Factors of Oncologic Outcomes in Patients Who Do Not Achieve Undetectable Prostate Specific Antigen After Radical Prostatectomy. J Urol (2013) 190:1750–6. doi:10.1016/j.juro.2013.04.073
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Parker, CC, Clarke, NW, Cook, AD, Kynaston, HG, Petersen, PM, Catton, C, et al. Timing of Radiotherapy After Radical Prostatectomy (RADICALS-RT): A Randomised, Controlled Phase 3 Trial. The Lancet (2020) 396:1413–21. doi:10.1016/s0140-6736(20)31553-1
CrossRef Full Text | Google Scholar
14. Sargos, P, Chabaud, S, Latorzeff, I, Magné, N, Benyoucef, A, Supiot, S, et al. Adjuvant Radiotherapy Versus Early Salvage Radiotherapy Plus Short-Term Androgen Deprivation Therapy in Men With Localised Prostate Cancer After Radical Prostatectomy (GETUG-AFU 17): A Randomised, Phase 3 Trial. Lancet Oncol (2020) 21:1341–52. doi:10.1016/s1470-2045(20)30454-x
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Vale, CL, Fisher, D, Kneebone, A, Parker, C, Pearse, M, Richaud, P, et al. Adjuvant or Early Salvage Radiotherapy for the Treatment of Localised and Locally Advanced Prostate Cancer: A Prospectively Planned Systematic Review and Meta-Analysis of Aggregate Data. The Lancet (2020) 396:1422–31. doi:10.1016/s0140-6736(20)31952-8
CrossRef Full Text | Google Scholar
16. Shipley, WU, Seiferheld, W, Lukka, HR, Major, PP, Heney, NM, Grignon, DJ, et al. NRG Oncology RTOG: Radiation With or Without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med (2017) 376:417–28. doi:10.1056/nejmoa1607529
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Carrie, C, Hasbini, A, de Laroche, G, Richaud, P, Guerif, S, Latorzeff, I, et al. Salvage Radiotherapy With or Without Short-Term Hormone Therapy for Rising Prostate-Specific Antigen Concentration After Radical Prostatectomy (GETUG-AFU 16): A Randomised, Multicentre, Open-Label Phase 3 Trial. Lancet Oncol (2016) 17:747–56. doi:10.1016/s1470-2045(16)00111-x
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Carrie, C, Magné, N, Burban-Provost, P, Sargos, P, Latorzeff, I, Lagrange, JL, et al. Short-Term Androgen Deprivation Therapy Combined With Radiotherapy as Salvage Treatment After Radical Prostatectomy for Prostate Cancer (GETUG-AFU 16): A 112-Month Follow-Up of a Phase 3, Randomised Trial. Lancet Oncol (2019) 20:1740–9. doi:10.1016/s1470-2045(19)30486-3
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Fossati, N, Robesti, D, Karnes, RJ, Soligo, M, Boorjian, SA, Bossi, A, et al. Assessing the Role and Optimal Duration of Hormonal Treatment in Association With Salvage Radiation Therapy After Radical Prostatectomy: Results From a Multi-Institutional Study. Eur Urol (2019) 76:443–9. doi:10.1016/j.eururo.2019.02.004
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Dess, RT, Sun, Y, Jackson, WC, Jairath, NK, Kishan, AU, Wallington, DG, et al. Association of Presalvage Radiotherapy PSA Levels After Prostatectomy With Outcomes of Long-Term Antiandrogen Therapy in Men With Prostate Cancer. JAMA Oncol (2020) 6:735–43. doi:10.1001/jamaoncol.2020.0109
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Abugharib, A, Jackson, WC, Tumati, V, Dess, RT, Lee, JY, Zhao, SG, et al. Very Early Salvage Radiotherapy Improves Distant Metastasis-Free Survival. J Urol (2017) 197:662–8. doi:10.1016/j.juro.2016.08.106
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Moreira, DM, Presti, JC, Aronson, WJ, Terris, MK, Kane, CJ, Amling, CL, et al. Natural History of Persistently Elevated Prostate Specific Antigen After Radical Prostatectomy: Results From the SEARCH Database. J Urol (2009) 182:2250–6. doi:10.1016/j.juro.2009.07.022
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Xiang, C, Liu, X, Chen, S, and Wang, P. Prediction of Biochemical Recurrence Following Radiotherapy Among Patients With Persistent PSA After Radical Prostatectomy: A Single-Center Experience. Urol Int (2018) 101:47–55. doi:10.1159/000488536
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Rogers, CG, Khan, MA, Craig Miller, M, Veltri, RW, and Partin, AW. Natural History of Disease Progression in Patients Who Fail to Achieve an Undetectable Prostate-Specific Antigen Level After Undergoing Radical Prostatectomy. Cancer (2004) 101:2549–56. doi:10.1002/cncr.20637
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Van den Broeck, T, van den Bergh, RCN, Arfi, N, Gross, T, Moris, L, Briers, E, et al. Prognostic Value of Biochemical Recurrence Following Treatment With Curative Intent for Prostate Cancer: A Systematic Review. Eur Urol (2019) 75:967–87. doi:10.1016/j.eururo.2018.10.011
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Pound, CR, Partin, AW, Eisenberger, MA, Chan, DW, Pearson, JD, and Walsh, PC. Natural History of Progression After PSA Elevation Following Radical Prostatectomy. J Urol (1999) 281:1591–7. doi:10.1001/jama.281.17.1591
CrossRef Full Text | Google Scholar
27. Boorjian, SA, Thompson, RH, Tollefson, MK, Rangel, LJ, Bergstralh, EJ, Blute, ML, et al. Long-Term Risk of Clinical Progression After Biochemical Recurrence Following Radical Prostatectomy: The Impact of Time From Surgery to Recurrence. Eur Urol (2011) 59:893–9. doi:10.1016/j.eururo.2011.02.026
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Pfister, D, Bolla, M, Briganti, A, Carroll, P, Cozzarini, C, Joniau, S, et al. Early Salvage Radiotherapy Following Radical Prostatectomy. Eur Urol (2014) 65:1034–43. doi:10.1016/j.eururo.2013.08.013
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Ohri, N, Dicker, AP, Trabulsi, EJ, and Showalter, TN. Can Early Implementation of Salvageradiotherapy for Prostate Cancer Improve the Therapeutic Ratio? A Systematic Review and Regression Meta-Analysis With Radiobiological Modelling. Eur J Cancer (2012) 48:837–44. doi:10.1016/j.ejca.2011.08.013
Comments (0)