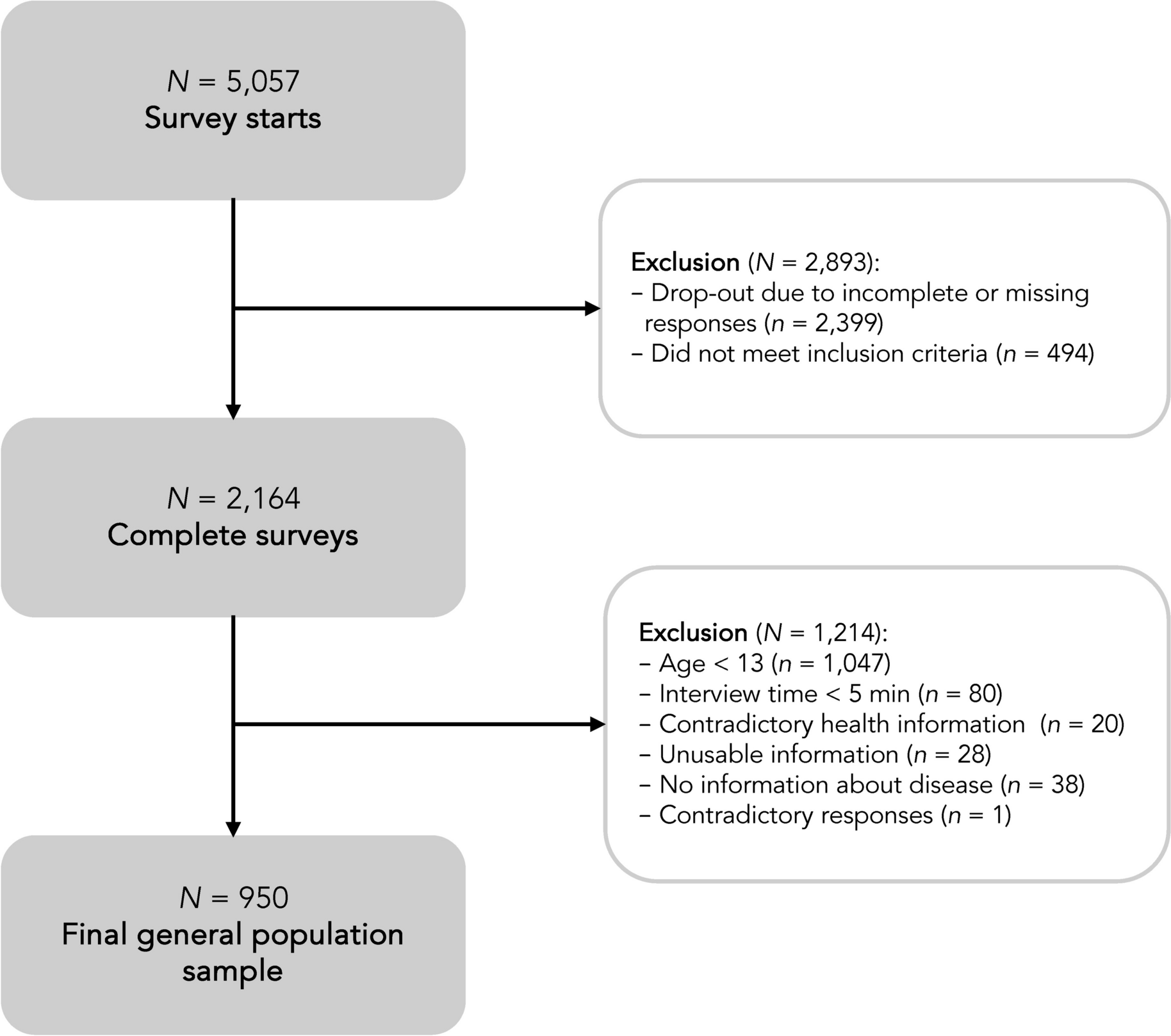
Twenty semi-structured interviews were completed with three fathers and 17 mothers. All parents agreed with the summary, and no additions were required to be included in our analyses. Therefore, no changes were required. Characteristics of the participants and their children are provided in Table 1. Themes and categories were developed. The main themes that parents of children with CCHD reported were: (1) “impact of diagnosis and disease on the family system,” (2) “parental concerns from diagnoses and beyond,” (3) “the need for information,” and (4) “the need for individualized and family-centered care.” The main themes can be divided into several sub-themes. The results are described in detail below.
Impact of diagnosis and disease on the family system
A CCHD appears to have an impact on various levels within a family system: (1) “impact on the patient,” (2) “impact on families (parents and siblings),” and (3) “impact on parental perceptions of child vulnerability and parenting style.”
Impact on the patient
Most parents indicate that their child functions above expectations and that the impact of the CCHD on the child is smaller than expected.
It has exceeded our expectations as I never thought he could play football for so long and that he can keep it up like this. (M5)
The impact is more significant when there are developmental problems. Accordingly, parents indicate that they are surprised that having a CCHD can influence so many areas. At the same time, they wonder whether the problems are the impact of the heart defect or whether this is innate and would also exist without a heart defect. According to their parent, children with a CCHD appear to experience merely few obstacles themselves, partly because the child does not know any better.
The impact on families
The impact of the heart defect may be more prominent for the parents and siblings than for the patient himself, as all parents indicated that the impact on themselves is enormous. The child’s condition can impact work, relationships, and the psychosocial well-being of parents. The impact on families is most significant in the first months to years after diagnosis, depending on the number of operations and additional problems and complications (e.g., tube feeding, protein losing enteropathy, allergies, or stagnant growth and development).
Parents describe the diagnosis, the subsequent choice to terminate or continue the pregnancy, the stress of childbirth, concerns surrounding the operation(s) and recovery, and the fear of possible additional problems as an uncertain rollercoaster phase. Parents report that they have endured this stressful roller coaster, which has lasted for months to years, in a kind of survival mode.
Especially at the beginning, it greatly impacts your daily life. It affected his brother, who had to sleep at Grandpa’s and Grandma’s. It affects your work. I was less concentrated, especially when things were not going well. You get some tough news yourself, which also takes a toll on you psychologically, so you must learn to deal with that. Furthermore, as a couple, you also must work together again. My husband deals with it differently than I do, So, in the end, it turns our lives upside down. (M11)
When it comes to the impact of the heart defect at the time of the interviews, several parents indicate that they always have to take the heart defect into account in their daily activities: they always have to think a few steps ahead (e.g., is there is a hospital nearby?), and they must be alert to overload or deterioration of cardiac function, and flexible in unexpected situations.
Additionally, the heart defect and associated hospital admissions and operations also have an impact on siblings. There are emotions like anger, anxiety, and sadness about the absence of parents during admissions, and older brothers and sisters are often extra alert but also concerned about the patient’s well-being. In the beginning, especially with more care-intensive children, much attention is paid to the patient, which sometimes leaves a mark on the family in the long term. Parents try to ensure that “the patient” is not given a special place within the family and that brothers and sisters receive sufficient attention. However, a CCHD must always be considered when planning activities and days out.
There is always a piece of extra alertness and, yes, also from the oldest children. There is always that extra bit of care: “Oh X, do not get on that climbing frame or you might fall out,” and taking her into account: Where are we going? Is it suitable for X? (M0)
Impact on parental perception of child vulnerability and parenting style
Parents reported that they perceive their child as more vulnerable, even though there is not always a reason to do so. In the case of more care-intensive children, it is difficult to let go of children and leave the daily care to others. These parents also indicate that this may limit their children’s actions, partly due to increased bleeding tendency due to blood-thinning medication in the event of falls and fear of overexertion. Regardless of the child’s overall functioning, parents indicate that they are overprotective, worry more quickly, and are more alert than sibling, for example, when children have a fever or a cold that they consult a doctor more quickly.
X was slow in developing large motor skills, and I linked everything to the heart defect, everything! With every cough, every vomit, I thought, oh no, her heart! While it was just the stomach flu. That was, of course, also my perception as an overprotective parent… (M1)
Parental concerns from diagnoses and beyond
Results regarding parental concerns were divided into three subthemes: (1) “navigating concerns per phase”, (2) “embracing limitations in an uncertain future,” and (3) “continued concerns in the face of brain injury, declining cardiac function and future surgeries, and reduction of concerns through reassuring information.” Details are described below.
Navigating concerns per phase
Parents’ concerns about their child with a heart defect include short-term concerns and long-term concerns and depend on the different phases they and their child go through. At the time of the prenatal diagnosis, concerns initially lie in the long term. Concerns about the short term dominate around postnatal diagnosis, birth, the operation, and in the first years afterward. When CCHD was diagnosed prenatally, parents reported that their main concern was whether the diagnosis was operable and whether there was a good chance of everyday life and adequate quality of life afterward.
After the diagnosis, we only asked ourselves one thing, and that was: how likely is it that he can just live a normal life? That was also the question that finally made us proceed with the pregnancy. We want him to function as much as possible as a normal child. (M6)
The concern that the heart defect was part of an underlying genetic disorder that would affect the child’s long-term functioning was also raised after diagnosis. After the decision has been made to continue the pregnancy, the fear of loss during pregnancy, delivery, or surgery arises. Another concern was the risk of complications that could affect long-term functioning, such as oxygen deficiency and its impact on the brain. After birth, in the run-up to the operation, and the period until discharge, parents indicate that they have lived from day to day, regardless of whether the diagnosis was made antenatal or postnatal. Worries were mainly about the short term: the fear of loss and the worry about complications surrounding the operation. There were not many expectations or concerns about the long term: they were trying to keep their child alive and survive themselves. After discharge, during the baby-toddler phase, parents continue to look in the short term and do not look too much ahead "from school age towards puberty, more concerns about the long-term arise again".
Initially, you are not concerned with the future at all. You are only concerned with the fact that my child has a heart defect and has to undergo an operation, and you have no idea how that works or what it is like. You have no room to think. It is still a life-or-death story in your head and has nothing to do with the future. You are just surviving and making sure your child stays alive. That is your biggest priority, and then you do not think about the future yet. You do not even want to think about the future because you are happy that you can take her home from the hospital. (M0)
Embracing limitations in an uncertain future
After discharge relief and joy prevail that their child is still alive, or their worries have not come true. Furthermore, parents indicate that they do not have high expectations of their child or consider functioning relative to healthy peers important, as the child’s well-being is most important in this phase, and it is unfair to compare their child with other children. Every child has a different medical history and usually develops in their own way and at their own pace.
If she wanted to become a pilot, that would not be possible because she has that abnormality. Well, if that is it… Not a top athlete either well… I do not think she has that ambition, either. So, you know, if that is it. (M4)
At school age, when there is more comparison with peers, when difference with peers increases, and towards puberty, more concerns and questions arise about the future. Concerns are reported regarding future functioning: “what can my child physically handle in the future,” “what can we expect from him,” and “ what problems will my child encounter when he gets older.” Also, concerns terms of mental well-being: “how much impact will the heart defect have on my child when he or she becomes a parent?” and concerns regarding independency are mentioned. Most concerns do not dominate but come up sometimes for most parents.
Continued concerns in the face of brain injury, declining cardiac function and future surgeries and reduction of concerns through reassuring information
Parents of children who have ended up in a resuscitation setting or who have had brain damage detected on postoperative MRI are more concerned about the future in terms of development and overall functioning in the period shortly after the operation.
In the beginning, mainly whether he would have a syndrome and what it would look like after birth. A bit of uncertainty, but later, after the operation and the cardiac arrest, more of: what will the future look like for him in terms of development? (F8)
Concerns about future functioning are also more significant and longer present among parents of children, of which it is expected they need cardiac interventions in the future. They wonder what the impact of declining heart function or new risky interventions on the child’s functioning will be.
With every operation, you will be told in advance what can go wrong, the risks, etcetera. However, yes, there were a lot of them… I have to say that the biggest concern for me was that she could not do anything afterward, that she had suffered from a lack of oxygen or that she could not walk or talk anymore, that you, yes, no, having a child back… that was my biggest fear, with every operation. (M13)
On the other hand, concerns are reduced in all phases by the absence of a genetic abnormality, a successful outcome of the operation, a good MRI, good functioning compared to peers, and a good assessment by a doctor or during follow-up assessments.
The need for information
The results reflect three aspects of parent’s need for information: (1) “the varying need for information and information source,” (2) “informed future: setting expectations with phased and individualized insights,” and (3) “insight into the neurodevelopment of children with heart defects and their incomparability with (healthy) peers.”
The varying needs for information and information sources
The interviews indicated that the need for information differs significantly between parents and, like concerns, changes by phase. When the heart defect is diagnosed antenatally, there is first a need for information on whether the heart defect is operable. Subsequently, information about the prospects of children with similar heart defects, both positive and negative, is needed to make a sound decision regarding continuing the pregnancy and to provide hope and reassurance.
I have looked up many things, which can sometimes confuse. You wonder: Is this article and what I am reading now correct? Anyway, you also take some advice from other parents about the experiences you read. (M9)
When it was decided to continue the pregnancy, the baby was born, and the operation completed, the need for information about the prospects of their child declines, and they do not look too much ahead. Information about future functioning can create unjustified expectations, but also unnecessary worries. Parents indicate that they have questions but realize that no one can predict how their child will develop. More questions arise about the heart defect’s future and overall functioning from school age onwards.
Now I would like to know: what are the life expectancies and experiences? Because we are now several years further, I am always curious about how children like that develop. How long do they live? And, of course, with age, more questions arise… Sometimes, I think about puberty. Can she get her period? Can they have children? Do you know all kinds of things for the future? That remains an unknown terrain for me, and maybe I will… Yes, I think she will also come up with all those questions herself later. But I know little about the future; what are the statistics, so to speak. (M13)
Informed future: setting expectations with phased and individualized insights
Information needed in the hospital admission run-up is about what lies ahead in the short term. Parents indicate their need for preparation for the admission and operating room using photo albums or guided tours. “What can you expect during such a hospital admission? What does the Intensive Care Unit and nursing department look like, what facilities are there, and what can you find where?”.
She rang the doorbell, and she said: I have something very confrontational for you, but it will help you, she then arrived with a booklet with photos of her child's open-heart surgery, and I thought: What is happening here? But when X was done and went from the OR to the ICU, I knew what to expect… I liked that. I could look at my child, and I did not have to look at all those tubes and wires because I knew what that image looked like, things like that, you want that. That is very confrontational, but it will help you so much. (M0)
In addition, several parents indicate that they need more information about possible secondary problems to be better prepared for what might come. Parents mention here the possible dependence on tube feeding after surgery, the impact on relationships and work, and the possible impact of hospitalization and surgery on both the parent and the child, such as stress, fears, nightmares, and trauma and how to deal with this as a parent.
Parents also indicate that they still need periodic information in the form of a mailing, a blog, or a newsletter with the latest research results about the type of heart disease their child suffers from and information about what to expect regarding neurodevelopment and neurodevelopmental problems and how they can support their children as best as possible. Finally, parents indicate their need for reports of their child’s assessment results in understandable language to be able to read back and share with, for example, school and other stakeholders.
You would prefer to receive clear feedback on paper about what has been done and the results. And in such a way that you can pass it on directly to the childcare or the school so that they know better about “Hey, what is going on? what have they been looking at?” Should we do anything about this as a school or day-care? Or can we help the child with something?” I think that as parents, you can easily reread it, without medical terms. (M6)
Insight into the development of children with heart defects and their incomparability with (healthy) peers
There is a general feeling that children with a heart defect cannot be compared to healthy children or siblings and that his or her medical background should be considered when assessing development. If developmental problems arise, there is a solid need to be able to place these in the light of his or her heart defect. Many parents, therefore, wonder whether the problems they encounter are more common in children with a heart defect.
And that might take away some concerns, if you know this could be part of her heart defect, then you think: okay, then that is it! Yes, that also gives you a bit of peace and security. (M9)
On the other hand, there is a realization that as a parent, you will never know whether the problems would not have existed without the heart defect. However, the knowledge that the developmental problems their child experiences are common provides recognition, relief, resignation, understanding, trust, and confirmation.
Concentration, a full head, yes, stimuli are difficult: he is quite bothered by noise stimuli. Yes, we cannot say in black and white: that is due to the heart defect, so you treat him in the sense of ADHD, and it is nice that you can act that way towards him. You can never say whether it is a direct consequence, right. (M10)
The need for individualized and family-centered care
Regarding parental experiences and needs for neurodevelopmental care during hospital admission and after discharge, four subthemes emerged: (1) “setting and shifting priorities”; (2) “the essential role of a customized, multidisciplinary follow-up program across childhood”; (3) “promoting empowerment and trust”; and (4) “family well-being and the need for aftercare for parents and siblings.”
Setting and shifting priorities
In the phase surrounding neonatal cardiac surgery, there is a particular need to strengthen the parent–child relationship. Attention to attachment, facilitating breastfeeding, involvement, and thinking along with parents in care are considered very valuable. The focus should be on comfort, survival, and recovery. Neurodevelopment is not a priority during this period.
When I am in the hospital, for my child who has had a heart operation, I would prefer that they take care of that. So I also think that care should be focused on correcting her heart, and I think it is very good that attention is also paid to other matters, but that is not why she is there. (M4)
However, parents indicate that good medical clinical care has contributed to the functioning of their child in the long term. Neurodevelopmental care and the availability of developmental experts, e.g., speech therapy, physiotherapy, and pedagogical care, are considered more important for more prolonged admissions or admissions are experienced as necessary, as well as the distraction and facilitation of being a child by giving information, tips, and tricks to parents about what they can offer their child to promote development as much as possible during hospital admission.
Where should I start? What should I do? Okay, she will sport, but is that enough? And what kind of sport is best for her? More focused... more advice focused on what suits her. (M13)
The essential role of a customized, multidisciplinary follow-up program across childhood
After discharge, there is a need for a more holistic approach to their child at the cardiology clinic, they examine his heart, conduct an ultrasound, and measure and weigh it. That heart is just a machine being fixed there, but it is a heart. Around it, there is a child doing all kinds of things. This is what I think: Yes, that is what the “Hart-op-Weg” outpatient clinic is focusing on – the bigger picture and further development. Every child must be monitored, not just regarding their heart, but also psychologically, developmentally, and the rest of the system, so to speak… from the machine. (M17)
There is a common need for a multidisciplinary, individual, customized follow-up program, where healthcare professionals monitor how their child functions and determine whether there is a need for additional diagnostics or support should be involved. When the child is doing well, there should be room for a shorter route or temporary follow-up stop with an option to resume or easily contact us if they have any questions or concerns. Parents prefer to assess their child by experienced developmental experts who know the child and the nature of their heart defect above a general practitioner. Parents value that their child is assessed in the light of his heart defect and that specific advice is given, taking their heart defect into account.
Well, very much of added value, because in our environment, such as a GP or regional hospital, they simply not know that much about heart defects, so they don’t watch and give advice in that way. And because many heart patients come together in the WKZ you can compare much better. You do not have a standard of healthy children but the standard of children with a CHD and… well, it really matters a lot how that’s compared. (M5)
Furthermore, parents need guidance in providing extra support and customized tips and tricks for daily life to support their child’s optimal development and how they can support children as best as possible.
Where should I start? What should I do? Okay, she will sport, but is that enough? And what kind of sport is best for her? More focused, more advice focused on what she, what suits her. (M13)
According to parents, development should be assessed at fixed moments around developmental milestones and other important milestones, such as attending school and choosing a sport. Lastly, accessible availability of health care professionals between appointments is appreciated.
Promoting empowerment and trust
Regardless of concerns about the child’s functioning, individual attention to the child’s functioning contributes to the need for confirmation and support. The follow-up meets the need for a place where someone thinks along, and questions and concerns can be discussed. The fact that healthcare professionals are available who watch and think along so that timely action can be taken gives parents relief. The regular checks provide reassurance and remove concerns, and positive reviews give hope for the future. If parents’ positive image is confirmed, it also gives them more self-confidence.
Yes, sometimes you just want confirmation of something. Or what a professional says about it because even though you hardly ever deal with it, there is always a bit of concern in your mind: if he is doing well and things like that. (F18)
According to parents, assessing the capabilities of older children also gives the child self-confidence and contributes to the feeling of being no different from other children.
A child can show during these tests that he is doing well, which is a huge incentive for the child. (M19)
Family well-being and the need for aftercare for parents and siblings
There is a strong need for attention to parents’ psychosocial well-being both during admission and afterward, with attention to possible traumas and guidance to give everything a place. Parents indicate that their well-being is essential to provide their children with the best possible guidance. Several parents suggest a structural follow-up meeting a few months after discharge, when peace has returned, to identify what is needed regarding psychosocial guidance for parents.
Maybe one more time for the parents, a conversation with a psychologist or something like that. Yes, yes, initially once, and then look from there: what extra care might be needed? (F18)
Parents also indicate that they need attention for the well-being of siblings. Furthermore, there is a need for information, tips, and tricks on how parents can guide, involve, and inform their other children about the situation and how they can respond to questions and concerns from siblings.


Comments (0)