
Remember me







The high prevalence of diseases of the cardiac electrical conduction system and arrhythmias has led to an increase in the indication of cardiac implantable electronic devices (CIEDs).1–3 Currently, between 35% and 45% of these patients are under oral anticoagulation treatment with vitamin K antagonists, new oral anticoagulants (NOACs), or oral antiplatelet agent (OAA), leading to a higher risk of hematoma in this population group.4
Pocket hematoma is a frequent complication with CIEDs, affecting 2.1% to 9.5% of patients, and is the main cause of CIED infection.5 In general, a pocket hematoma can be treated conservatively. However, its evacuation, which is required in 0.3% to 2% of cases, is associated with a 15 times higher risk of infection, longer hospitalization periods, and increased mortality (2% compared with 0.7%).6 Many hematomas can be avoided using careful hemostasis and optimal perioperative management of antithrombotic treatment.7–9
Applying pressure on a wound reduces both the accumulation of extracellular liquid and hemorrhage. In addition, hypothermic treatment of a surgical wound contributes to capillary vasoconstriction, accelerating the process of cicatrization. The use of compression bandaging and/or the application of a local cold source have been established as useful techniques to reduce edema and prevent the onset of hematoma.
For CIED-related postsurgical wounds, an electrophysiology laboratory nurse performs dressing changes and wound follow-up. Thus, the nurse has a fundamental role in the early detection of the signs and symptoms of complications.10 Although pressure and hyperthermic treatment are common practice among patients with device implants and a high risk of bleeding, the authors found no studies in the literature examining the efficacy of either method in relation to preventing the onset of hematoma.
The aim of this study was to determine if the use of a hypothermic compression bandage (HCB) following device implantation or replacement is as safe as a conventional compression bandage (CCB) in patients at high risk of thromboembolic events. The primary comparison was the incidence of CIED pocket bruising over a 10-day period after the procedure. The secondary objectives were to assess the incidence of hematomas by type of intervention (implantation or replacement), sex, type of CIED (pacemaker [PM], implantable cardioverter defibrillator [ICD], or cardiac resynchronization therapy [CRT]), and oral anticoagulant (OAC)/NOAC or OAA treatment.
METHODS Research Study DesignThis was a controlled, randomized study, carried out in the third-level center Hospital Clinic of Barcelona. The research study design is outlined in Figure 1.
 Figure 1.:
Figure 1.: STUDY FLOW DIAGRAMAbbreviations: CCB, conventional compression bandage; HCB, hypothermic compression bandage.
ParticipantsThe study consecutively included all adult patients taking an OAC and/or OAA who underwent a CIED implantation or replacement due to battery depletion.
The exclusion criteria were (a) insertion of drainage in the wound, (b) not adhering to the presurgical antithrombotic protocol, (c) elevated therapeutic international normalized ratio (>3.5), (d) not undergoing implant follow-up in the same center, (e) patients with coagulation and hemostasis disorders, (f) device replacements for reasons other than battery depletion, and (g) age younger than 18 years.
All patients who met the inclusion criteria and none of the exclusion criteria were invited to participate in this study.
Device Implantation and Postprocedure ManagementThe CIED device implantation or replacement was performed by an electrophysiologist with more than 5 years of professional experience in an electrophysiology laboratory, where more than 200 patients are operated on every year. Further, all nurses who participated in the study had more than 3 years of experience in the unit. For every implantation or CIED replacement, providers followed the guideline of the European Society of Cardiology for management of antithrombotic presurgical treatment.1
After administering antibiotics and local anesthesia, a pectoral incision was performed to create the device’s pocket. Venous access was obtained through a puncture of the subclavian vein, and the cables were implanted under a fluoroscopic light. The atrial and right ventricular leads were of active fixation. As for CRTs, for pacing of the left ventricle, the passively fixed lead was implanted in the coronary sinus. The leads were not manipulated in the replacement of the CIED.
Intraoperative hemostasis was ensured through the meticulous use of the electrocautery and sterile, radiopaque, cotton sanitary napkins. The incision closure was performed using an internal absorbable suture and skin staples. A sterile hydrocolloid dressing was applied to all patients to cover the wound. The laboratory nurse was responsible for applying the compression bandage just after finishing the procedure.
Control groupA CCB was applied for the control group participants. The nurse applied three elastic bandage strips to compress the surgical wound using the weight of a 10 × 10 cm gauze pack. The bandage was removed after 8 hours. The ipsilateral arm was immobilized for 24 hours using a sling.
Intervention groupIntervention group participants wore the HCB. In addition to the three elastic bandage strips, this technique adds an ice prosthesis to stimulate vasoconstriction in the compression bandage (Figure 2). This bandage was also removed after 8 hours, and the ipsilateral arm was immobilized for 24 hours using a sling.
 Figure 2.:
Figure 2.: PATIENT WEARING A HYPOTHERMIC COMPRESSIVE BANDAGE WITH IMMOBILIZATION OF THE LEFT UPPER EXTREMITY FOLLOWING CIED IMPLANTATIONA, Frontal view. B, Lateral view.Abbreviation: CIED, cardiac implantable electronic device.The patient provided consent for these images to be published.
EndpointsThe primary outcome variable was the onset of hematoma in the surgical wound of the implant or CIED replacement. Based on clinical findings, skin was classified as healthy (no evidence of inflammation, bleeding, or infection) or as having a hematoma. Hematoma classification is divided into three grades, from least to most severe.11
Grade IEcchymosis defined as mild bleeding in the cardiac device pocket with no signs of inflammation or pain (watch and wait).
Grade IIMild hematoma described as a protuberant and palpable mass of 2 cm or less above the implanted generator. Moderate bleeding in the CIED pocket causes a functional deterioration or pain in the cardiac device zone.
Grade IIISevere hematoma defined as a protuberant and palpable mass of greater than 2 cm. The hematoma evacuation if it causes tension in the skin with poor tissue perfusion that increases and generates major pain. It requires an immediate suspension of OAC or OAA use, and patient hospitalization is prolonged for more than 24 hours.
To study the secondary objectives, the researchers collected sociodemographic variables and patient care details, including the type of oral anticoagulation treatment used (OAC, OAA, or both), characteristics of the implanted CIED, and the technique used (implant or replacement).
Data CollectionData collection began in May 2018, and the required number of participants was reached in May 2019. Before device implant or replacement was performed, a nurse from the electrophysiology laboratory at the Hospital Clinic of Barcelona assigned each participant a random group using a random number list, and the assignment was saved inside opaque, sealed envelopes.
Nurses from the outpatient clinic at the Hospital Clinic of Barcelona who were blinded to the compression technique evaluated the wound and periwound skin condition 10 days after the surgical intervention.
Statistical AnalysisThe data were analyzed with the statistical software pack SPSS version 23.0 (IBM Corp). For comparisons between the randomly assigned groups, continuous data were analyzed with Pearson and Spearman correlations, and categorical data were analyzed with the χ2 statistic. A Student t test was used to compare the average between the two independent groups. Statistical significance was established if P ≤ .05.
Considering a P of 10% with a confidence level of 95% (α = .05) and a power of 0.8 for a difference of 10%, the researcher calculated that 141 patients were needed in each group. To avoid data losses, an extra 10% was added to the sample (n = 28). Therefore, the number of participants included in each group was 155 (N = 310).
Ethical ConsiderationsThis research study complied with the principles of the 2013 Declaration of Helsinki and was approved by the hospital’s ethical committee (HCB/2017/0150) and clinicaltrials.gov (NCT05500768). The informed results were adjusted to the revised Standards for Excellence and Reports of Quality improvements (EQUATOR) using a CONSORT diagram.12 All participants received verbal and written information about the study and provided informed written consent. If the patient was not able to communicate, the authorization was obtained from the patient’s legal guardian.
RESULTSA total of 310 patients participated in this study: 156 in the intervention group and 153 in the control group. There was no patient crossover between the assigned groups. The reasons for lack of follow-up were due to death (n = 2), patient not returning for follow-up (n = 5), and loss of the data collection sheet (n = 1). Following data losses, researchers analyzed a total of 149 control group participants and 153 intervention group participants. No adverse effects, such as infection, trauma, or allergy, were observed with either of the bandaging techniques applied.
Population DescriptionThe average age of the participants was 74 ± 11 years, and 75% were men. The average duration of the surgical intervention was 75 ± 42 minutes. Regarding anticoagulant therapy, 144 participants (47.7%) received OAA treatment, 140 (46.35%) received OAC, and 18 (5.9%) received both treatments. Further, 117 patients (83.6%) were anticoagulated with vitamin K antagonist, with a mean international normalized ratio of 1.9 ± 0.6.
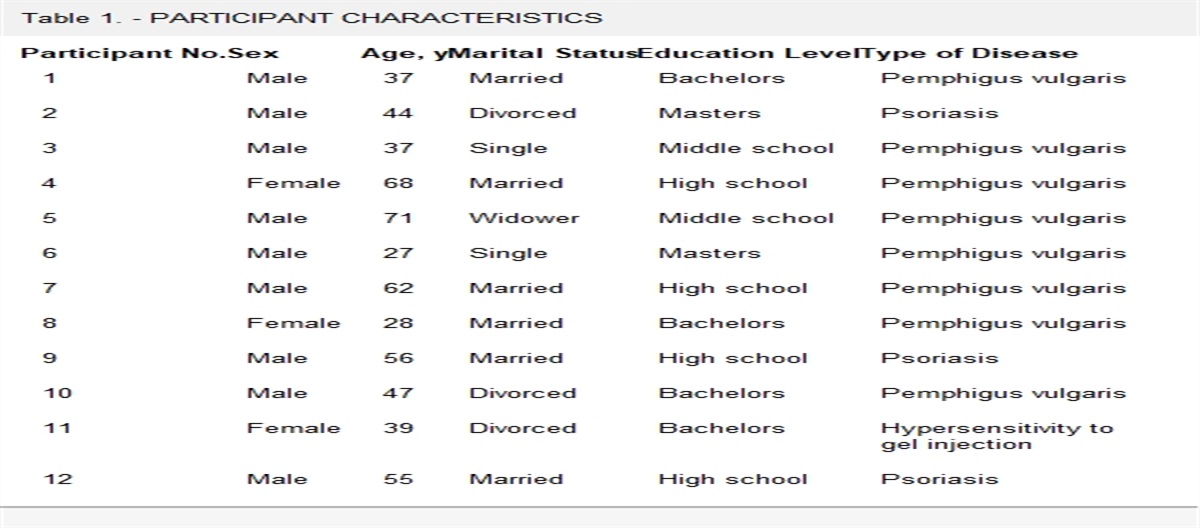
The principal comorbidities recorded among the participants were diabetes (n = 103, 34.1%), dyslipidemia (n = 179, 59.3%), smoking (n = 40, 13.2%), arterial hypertension (n = 225, 74.5%), and obesity (n = 61, 20.2%). Regarding CIED type, 185 participants (61.3%) had a PM, and 117 (38.7%) had an ICD. Whereas 201 participants (66.5%) underwent a first implantation, 101 (33.4%) underwent device replacements. The numbers of leads of each CIED included were as follows: 142, single-chamber (47%); 68, bichambers (22.5%); and 92, CRT (30.5%). The groups did not differ significantly in any of the demographic parameters or in the clinical characteristics except for the higher prevalence of ICDs (P = .037) and dyslipidemia (P = .007) among the intervention group (Table 1).
Table 1. - PARTICIPANT CHARACTERISTICS Characteristic Total (N = 302), n (%) CCB Group (n = 149), n (%) HCB Group (n = 153), n (%) P Age, mean ± SD, y 74 ± 11.00 74 ± 11.08 73 ± 10.2 .34 Men 226 (74.83) 106 (71.14) 120 (78.43) .14 Dyslipedemia 179 (59.27) 77 (51.67) 102 (66.66) .008 Diabetes 103 (34.10) 50 (33.55) 53 (34,64) .84 Smoker 40 (13.24) 16 (10.70) 23 (15.03) .26 AHT 225 (74.50) 111 (74.49) 114 (74.50) .99 Obesity 61 (20.20) 24 (16.10) 37 (24.18) .08 Duration of intervention, mean ± SD, min 75.11 ± 42 73.00 ± 39 77.00 ± 43 .40 Device type .04 PM 185 (61.25) 100 (67.11) 85 (55.55) ICD 117 (38.74) 49 (32.8) 68 (44.44) Intervention .13 Implantation 201 (66.55) 93 (62.45) 108 (70.58) Replacement 101 (33.44) 56 (37.58) 45 (29.41) No. of leads .75 Single chamber 142 (47.01) 73 (48.99) 69 (45.09) Bichamber 68 (22.51) 30 (20.13) 38 (24.83) CRT 92 (30.46) 46 (30.87) 46 (30.06) Antithrombotic treatment OAC/NOAC 140 (46,35) 73 (48,99) 67 ( 43,79) .29 AVK 117 (83,57) 58 (72,5) 59(75,6) .65 NAVK 41 (29.30) 22 (27.50) 19 (24.40) .45 OAA 144 (47.68) 69 (46.30) 75 (49.01) .47 OAC/NOAC + OAA 18 (5.96) 7 (4.69) 11 (7.18) .36Abbreviations: AHT, arterial hypertension; AVK, antagonists to vitamin K; CCB, conventional compression bandage; CRT, cardiac resynchronization therapy; HCB, hypothermic compression bandage; ICD, implantable cardioverter defibrillator; NAVK, nonantagonists to vitamin K; NOAC, new oral anticoagulants; OAA, oral antiplatelet agent; OAC, oral anticoagulation; PM, pacemaker.
Ecchymosis (grade I) was present in the surgical wound zone in 36 patients (11.9%): 17 patients in the intervention group (11.1%) and 19 patients in the control group (12.8%; P = .6). A mild hematoma (grade II) was noted in 13 patients (4.3%): 4 patients in the intervention group (2.6%) and 9 patients in the control group (6.0%; P = .1). No patient had a severe hematoma (grade III; Table 2). Therefore, no significant difference was obtained between the two types of bandaging for each hematoma grade (Figure 3).
Table 2. - SKIN CONDITION AFTER 7 TO 15 DAYS Condition Total (N = 302), n (%) CCB Group (n = 149), n (%) HCB Group (n = 153), n (%) P Ecchymosis 36 (11.9) 19 (12.8) 17 (11.1) .6 Mild hematoma 13 (4.3) 9 (6.0) 4 (2.6) .1 Severe hematoma 0 0 0 1.0Abbreviations: CCB, conventional compression bandage; HCB, hypothermic compression bandage.
 Figure 3.:
Figure 3.: ASSESSED WOUND CONDITION BY GROUP, EXPRESSED AS THE PERCENTAGE OF OCCURRENCE
Among patients receiving OAC/NOAC treatment, 12.1% (n = 17) developed ecchymosis, and 4.3% (n = 6) developed a mild hematoma (P = .6). Among the patients taking an OAA, 11.1% (n = 16) developed ecchymosis, and 4.0% (n = 7) had a mild hematoma (P = .5). Of the patients receiving both treatments simultaneously, 16.7% (n = 3) developed ecchymosis, and none had mild hematoma (P = .5).
Total ecchymosis and mild hematoma occurrence did not vary by sex, type of surgery, or device type. Whereas 27 men (11.9%) developed ecchymosis and 9 (4%) developed a mild hematoma, 9 women (11.8%) developed ecchymosis and 4 (5.3%) had a hematoma (P = .9). For patients undergoing implantations, the incidence of ecchymosis was 26 (12.9%), and the incidence of mild hematoma was 10 (5%). Similarly, among patients undergoing replacements, the incidence of ecchymosis was 10 (9.9%), and the incidence of mild hematoma was 3 (3%; P = .5). When evaluating by device type, PM presented 21 cases of ecchymosis (12.9%) and 9 of mild hematomas (4.9%), ICDs presented 15 cases of ecchymosis (12.8%) and 4 of mild hematomas (3.4%), and CRTs presented 10 cases of ecchymosis (10.9%) and 4 of mild hematomas (4.3%; P = .8; Table 3).
Table 3. - RESULTS OF THE SECONDARY OBJECTIVES: HEMATOMA GRADE ACCORDING TO ANTITHROMBOTIC TREATMENT, SEX, INTERVENTION, AND DEVICE TYPE Variable Total (n = 49), n (%) P Ecchymosis (n = 36), n (%) P Mild Hematoma (n = 13), n (%) P Antithrombotic treatment OAC/NOAC 23 (46.9) .59 17 (12.1) .58 6 (4.3) .37 OAA 23 (46.9) .52 16 (11.1) .49 7 (4.9) .34 OAC + OAA 3 (6.12) .55 3 (16.7) .52 0 (0.0) .35 Sex .89 .98 .63 Men 36 (73.5) 27 (11.9) 9 (4.0) Women 13 (26.5) 9 (11.8) 4 (5.3) Intervention .51 .44 .42 CIED implantation 36 (73.5) 26 (12.9) 10 (5.0) CIED replacement 13 (26.5) 10 (9.9) 3 (3.0) Device type .78 .70 .55 PM 30 (61.2) 21 (11.4) 9 (4.9) ICD 19 (38.8) 15 (12.8) 4 (3.4) CRT 14 (28.6) 10 (10.9) 4 (4.3)Abbreviations: CEID, cardiac implantable electronic device; CRT, cardiac resynchronization therapy; ICD, implantable cardioverter defibrillator; NOAC, new oral anticoagulants; OAA, oral antiplatelet agents; OAC, oral anticoagulation; PM, pacemaker.
The study results indicate that applying either HCB or CCB after a CIED implant is equally effective for the prevention of hematomas. Both techniques are cost-effective, but given these results, it may not be advisable to apply hypothermic compression on the pocket zone because it is likely to create more work for the nurse and be more uncomfortable for the patient. Only a few studies have evaluated the grade of the hematoma according to the bandage type. Molinero et al13 evaluated two groups of patients, both retrospectively, and prospectively and concluded that a bandage with an ice dressing for cold therapy was more effective in preventing hematomas. However, those authors did not consider the antithrombotic treatment of each patient.13
To prevent hematoma, providers should adjust the patient’s antithrombotic treatment prior to surgical intervention. Although clinical guidelines recommend compressive therapy for the surgical wound, they do not detail proper procedure,1,14 leaving compressive therapy decisions to the implant care team. There are several devices on the market that generate compression on a surgical wound, such as the Pocket Pal II (Pressure Products) or the Premofix PM/ICD set (Andanza). However, they are single use, impersonal, and opaque, which inhibits visual control of the surgical zone. These devices also are not funded by public healthcare in the authors’ country. In addition, randomized studies evaluating these devices do not show significant differences in preventing grade II and III hematomas in comparison with a CCB.15
In the present study, the researchers excluded patients who had a vacuum drain implanted in the wound at the end of the surgical procedure because this was considered a bias factor. Mukherjee et al16 used this technique on patients undergoing antithrombotic treatment who had high bleeding risk and found that it reduced the risk of infection and hematoma. Other intraoperative techniques to reduce the risk of hematoma include the use of fibrin sealing dressings; hemostatic powder; topical tranexamic acid; hemostatic sponges; hemostatic absorbable gauzes; and physical techniques, such as the anti-Trendelenburg posture at 30° or electrocautery. All of these techniques have randomized studies showing their effectiveness.17
The STOP-HEMATOMA I study by Turagam et al18 found that applying compression in the device’s pocket reduces the risk of ecchymosis in patients with an OAC or OAA treatment, in comparison with no compression. They evaluated the wounds 7 days postsurgery. No significant differences were observed in the onset of more severe hematomas.18
Awada et al19 compared three techniques of hemostasis in patients with OAC and/or OAA: Stypro (hemostatic sponge; Curasan), compression system (Premofix), and vacuum draining, all of which had a control group. They observed that the compression technique combined with the hemostatic sponge reduced the incidence of mild hematoma.19
The use of OAA and OAC/NOAC therapy can prolong the bleeding time up to beyond 24 hours after the surgical procedure. Sudden or exaggerated movements of the affected upper extremity can reactivate bleeding during the first days postprocedure. Thus, immobilization of the shoulder articulation is recommended for patients on anticoagulation therapy, and these patients are also instructed not to handle weight/carry anything with the affected extremity for the first 2 weeks. The nurse in charge of wound management should provide patient education on wound care to prevent complications and provide recommendations should a complication develop.
The presurgical management of the antithrombotic treatment was effective in preventing hematoma, given that this study obtained percentages similar to those described in the literature.20 Likewise, no statistically significant difference was found between treatments of OAC/NOAC and/or OAA among the patients. The onset of hematomas also did not vary by sex, although women were underrepresented in this study (25%, n = 76). The group of patients undergoing a first device implantation experienced more ecchymosis and hematomas than those undergoing a replacement, but the differences were not statistically significant. Axillary vein puncture may be the cause of bleeding in these patients.
LimitationsThe intervention was performed in one center, which limits the external validity of the results. The exact pressure of each bandage was not calculated and thus could vary according to the operator. Further, the researchers did not monitor when the ice began to melt in the HCB; thus, the effect of the HCB on tissue vasoconstriction could not be measured.
CONCLUSIONSTo the authors’ knowledge, this is the first study in which CIED wounds using HCB were randomized. The results indicate that bandaging with or without hypothermic therapy is effective in the prevention of hematomas. The authors propose a randomized study that compares the incidence of bleeding using both types of bandaging in the general population, not just patients with a high risk of bleeding. Further research is needed to determine the optimal bandaging for the wound of the CIED pocket.
Implications for Practice - Compression bandages with or without hypothermic therapy are effective for the prevention of hematomas in implant wounds of cardiac pacing devices. - Patients undergoing anticoagulation or antiplatelet therapy may benefit from a compression bandage with hypothermic therapy. - The HCB presents fewer minor bruises compared with CCBs. REFERENCES 1. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427–520. 2. Fernandez I, Osca J, Alzueta J. Registro Español de Desfibrilador Automático Implantable. XVII Informe Oficial de la Asociación del Ritmo Cardiaco de la Sociedad Española de Cardiología (2020). Rev Esp Cardiol 2021;74:971–82. 3. Pombo M, Chimeno J, Bertomeu-Gonzalez V, et al. Registro Español de Marcapasos. XVIII Informe Oficial de la Sección de Estimulación Cardíac de la sociedad Española de Cardiología (2020). Rev Esp Cardiol 2021;74(12)1085–95. 4. Essebag V, Healey JS, Joza J, et al. Effect of direct oral anticoagulants, warfarin, and antiplatelet agents on risk of device pocket hematoma: combined analysis of BRUISE CONTROL 1 and 2. Circ Arrhythmia Electrophysiol 2019;12:1–8. 5. Song J, Tark A, Larson EL. The relationship between pocket hematoma and risk of wound infection among patients with a cardiovascular implantable electronic device: an integrative review. Heart Lung 2020;49:92–8. 6. Essebag V, Verma A, Healey JS, et al. Clinically significant pocket hematoma increases long-term risk of device infection: Bruise Control Infection study. J Am Coll Cardiol 2016;67:1300–8. 7. Hu J, Zheng J, Liu X, et al. Effect of a pocket compression device on hematomas, skin reactions, and comfort in patients receiving a cardiovascular implantable electronic device: a randomized controlled trial. J Interv Card Electrophysiol 2022;63:275–81. 8. Fei Y-P, Wang L, Zhu C-Y, et al. Effect of a novel pocket compression device on hematomas following cardiac electronic device implantation in patients receiving direct oral anticoagulants. Front Cardiovasc Med 2022;9:1–10. 9. Yang X, Wang Z, Zhang Y, et al. The safety and efficacy of antithrombotic therapy in patients undergoing cardiac rhythm device implantation: a meta-analysis. Europace 2015;17:1076–84. 10. Montoya A, Heredia C. Seguimiento heridas quirúrgicas de dispositivos de estimulación cardiaca. Enferm Cardiol Año XIX 2012:21–5. 11. De Sensi F, Miracapillo G, Cresti A, et al. Pocket hematoma: a call for definition. PACE Pacing Clin Electrophysiol 2015;38:909–13. 12. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:698–702. 13. Molinero Ochoa A, Puertas Calvero M, Gallardo Barrancos O, et al. Uso de la crioterapia tras la implantación de marcapasos. Enferm en Cardiol 2006;38:44–6. 14. Stevenson WG, Tracy CM, Epstein AE, et al. 2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration. J Thorac Cardiovasc Surg 2012;144:e127–45. 15. Mehta NK, Doerr K, Skipper A, et al. Current strategies to minimize postoperative hematoma formation in patients undergoing cardiac implantable electronic device implantation: a review. Heart Rhythm 2021;18:641–50. 16. Mukherjee SS, Saggu D, Chennapragada S, et al. Device implantation for patients on antiplatelets and anticoagulants: use of suction drain. Indian Heart J 2018;70:S389–93. 17. Barbar T, Patel R, Thomas G, et al. Strategies to prevent cardiac implantable electronic device infection. J Innov Card Rhythm Manag 2020;11:3949–56. 18. Turagam MK, Nagarajan DV, Bartus K, et al. Use of a pocket compression device for the prevention and treatment of pocket hematoma after pacemaker and defibrillator implantation (STOP-HEMATOMA-I). J Interv Card Electrophysiol 2017;49:197–204. 19. Awada H, Geller JC, Brunelli M, et al. Pocket related complications following cardiac electronic device implantation in patients receiving anticoagulation and/or dual antiplatelet therapy: prospective evaluation of different preventive strategies. J Interv Card Electrophysiol 2019;54:247–55. 20. Nichols CI, Vose JG. Incidence of bleeding-related complications during primary implantation and replacement of cardiac implantable electronic devices. J Am Heart Assoc 2017;6(1):e004263.
Comments (0)