This is the first survey to assess and compare current practice in managing ankle OA amongst physiotherapists and podiatrists in the UK. There is little guidance currently available to help allied healthcare professionals plan an evidence-based management plan of usual care for managing this condition; most guidance is for knee OA and hip OA.
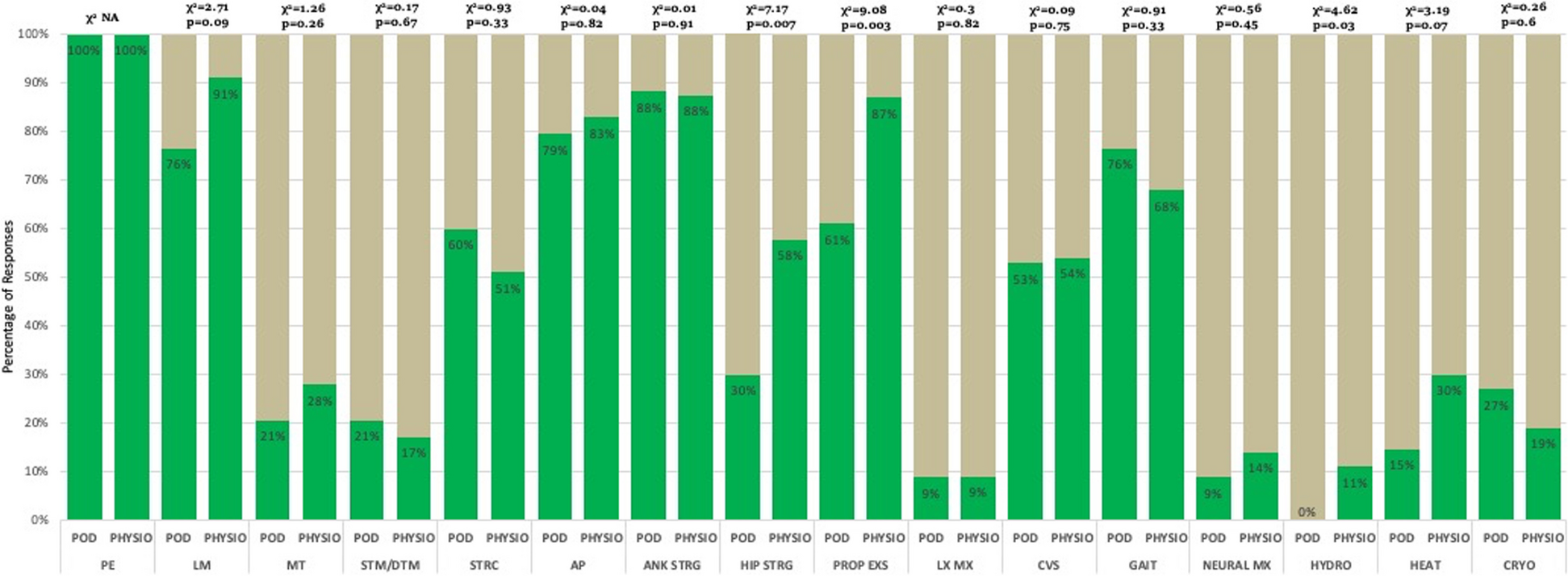
Both professions always or usually used patient education, lifestyle modification, and ankle strengthening exercises, with physiotherapists additionally using self-management and proprioception exercises, whereas podiatrists additionally used activity pacing and gait training. Outside of these five, other commonly used ways to manage ankle OA by physiotherapists were hip strengthening (58%) and by podiatrists were orthotics (73%) and self-management (64%) (Table 2). These treatment choices align with the top three treatment aims in both professions to reduce pain, improve quality of life, and teach self-management. This consensus concurs with many general OA guidelines, such as National Institute for Health and care Excellence (NICE [6], and Osteoarthritis Research Society International (OARSI) which includes patient education, exercise and self-management [7] as core treatment options, although these guidelines are not specific to ankle OA. Additionally, our survey results align with the treatment research agenda from an international foot and ankle OA consortium which recommended understanding usual care of foot and ankle OA to inform the design of control interventions in clinical trials [8]. It is also in line with the modern rehabilitation model for chronic pain which suggests using education to improve the effectiveness of other treatment options, and adding active/self-management techniques as a part of usual care [9].
Some of the treatment options reported by physiotherapists suggest they extrapolated evidence from other joint sites and applied to ankle OA. Hip strengthening was commonly used by physiotherapists (58%) but not podiatrists (27%), which does not align with a systematic review recommending hip strengthening for the conservative management of knee OA but not ankle OA [10]. There were several treatment options which were used sometimes, rarely or never by physiotherapists or podiatrists including hydrotherapy, electrotherapy, dry needling/acupuncture, taping, and intra-articular injections of visco-supplementation or platelet-rich plasma (PRP). Possible reasons include lack of access to hydrotherapy, contradictory OA guidelines by NICE [5] and OARSI [7] about acupuncture for OA, a lack of injection skills, and either the limited availability of visco-supplementation products or PRP in the NHS or a lack of supporting evidence. The observation that few physiotherapists (4%) and podiatrists (15%) used electrotherapy to treat ankle OA contrasts with NICE [5] and OARSI [7] guidelines recommending transcutaneous electrical nerve stimulation (TENS) to alleviate pain. Less than a third of respondents in either professions opted for ankle bracing or taping as usual care. This is surprising, particularly with physiotherapists, since taping is commonly used to reduce ankle range of motion and improve joint stability [11]. The aim of ankle braces is similar [12] but the low uptake of bracing might be due to the survey not specifying the stage of ankle OA clinicians should consider when responding to these questions. It might be that some clinicians only consider ankle bracing in end-stage ankle OA. Orthotics were used significantly more by podiatrists (73%) than physiotherapists (37%), consistent with the finding of a survey of physiotherapists’ and podiatrists’ treatment of plantar fasciitis that foot orthotics were considered the specialist role of podiatrists [13]. It is possible that physiotherapists refer to other services for orthotics but our survey did not distinguish those fitting orthotics themselves and those referring to podiatric or orthotic services. The use of footwear, as opposed to orthotics, was not available as a treatment option in the survey and it is possible that respondents may have opted for this if it had been available. Interestingly, despite podiatrists being asked to contribute at the survey’s development stage, a ‘footwear’ option was not suggested and so was not included in the final version. Although this survey provides data from physiotherapists and podiatrists as to what is current practice for ‘usual care’ in ankle OA, this has not yet been robustly assessed for its efficacy and should be the target for future funding applications.
A survey on the management of foot and ankle OA by GPs in Australia found that pharmacological management was favoured over active and self-management techniques [14]. Our survey found medications were used by nearly half of both physiotherapists and podiatrists. There are approximately 1400 physiotherapists and 450 podiatrists registered as independent or supplementary prescribers in the UK. [15], but we did not ask whether medications were prescribed directly by the physiotherapist or podiatrist, or whether the patient was required to see another healthcare professional to obtain a prescription.
This study had some limitations. Only UK-based practitioners were included, limiting the generalizability of our findings. Our response of 98 is smaller than the 191–293 physiotherapists or podiatrists who responded to electronic surveys of the management of other musculoskeletal conditions [15,16,17,18]. It is not possible to establish the exact response to the study owing to its online nature and the denominator who saw the survey invitation being unknown. This study did not identify the length of participants’ clinical experience which might have influenced responses if some treatments such as prescribed medications or intra-articular injections would be more likely be administered by more experienced practitioners. However, just over a third of physiotherapists and half of podiatrists had a master’s degree as their highest qualification which suggests a level of seniority and experience amongst many respondents and the possibility of bias towards these more advanced treatments. We did not make a distinction between foot orthoses, ankle orthoses and ankle foot orthoses (AFOs). Some clinicians might interpret these terms differently from our intended interpretation of an insole type of support. Lastly, due to the small sample sizes in each group, no comparison was made between private and NHS practice, nor in the practice between different countries of the UK.










Comments (0)