
Remember me


A global budget impact model (BIM) was developed in Microsoft Excel 2010 by AstraZeneca following the principles of good practice in budget impact modelling [16]. The global BIM model was adapted and evaluated to the Argentinian settings to estimate two scenarios over a 5-year time horizon: one where the current first-line maintenance treatment landscape continues without the addition of olaparib (current scenario) and the other where olaparib was added to bevacizumab in the first-line maintenance treatment landscape (projected scenario). The 5-year time horizon was defined on the basis of both the relevance for the budget holder and in line with the principles of good practices for reporting BIAs [16]. All the epidemiological parameters and the market shares input of the model were estimated and validated on the basis of the local clinical oncologist expert member of the research team. The BIM estimates the budget impact in terms of absolute terms, relative terms (the ratio of the projected scenario and the current scenario) and per-member per-month (PMPM) terms under the perspective of the third-party health system payer. In this paper, when referring to PMPM, we are considering one million women covered. In other words, we refer to per-women per-month. Therefore, we adjusted the PMPM estimates by sex applying the following formula:
$$} = \frac }}}/12}} \right)}}$$
(1)
In Eq. (1), \(\beta_\) represent the net budget impact for the healthcare sector ‘i’.
In addition, the results were presented disaggregated by healthcare sectors. In Argentina, the healthcare system is decentralised and fragmented into three sectors: public, social security and private. The social security sector is the largest and provides healthcare coverage to approximately 46% of the Argentine population. The social security sector provides coverage to public and private workers, and there is one nationwide social health insurance fund for retired workers [Programa de Asistencia Médica Integral (PAMI)], which is broadly comparable to Medicare in the USA. On the other hand, 16% of individuals are covered by the private sector. This sector provides coverage to people from social security coverage contracting private supplementary plans but also people enrolled on an individual basis through direct and voluntary payments. Lastly, approximately 38% of the population is covered by the public sector [17]. All Argentinian citizens and residents, including foreign workers or tourists, can get healthcare from public facilities.
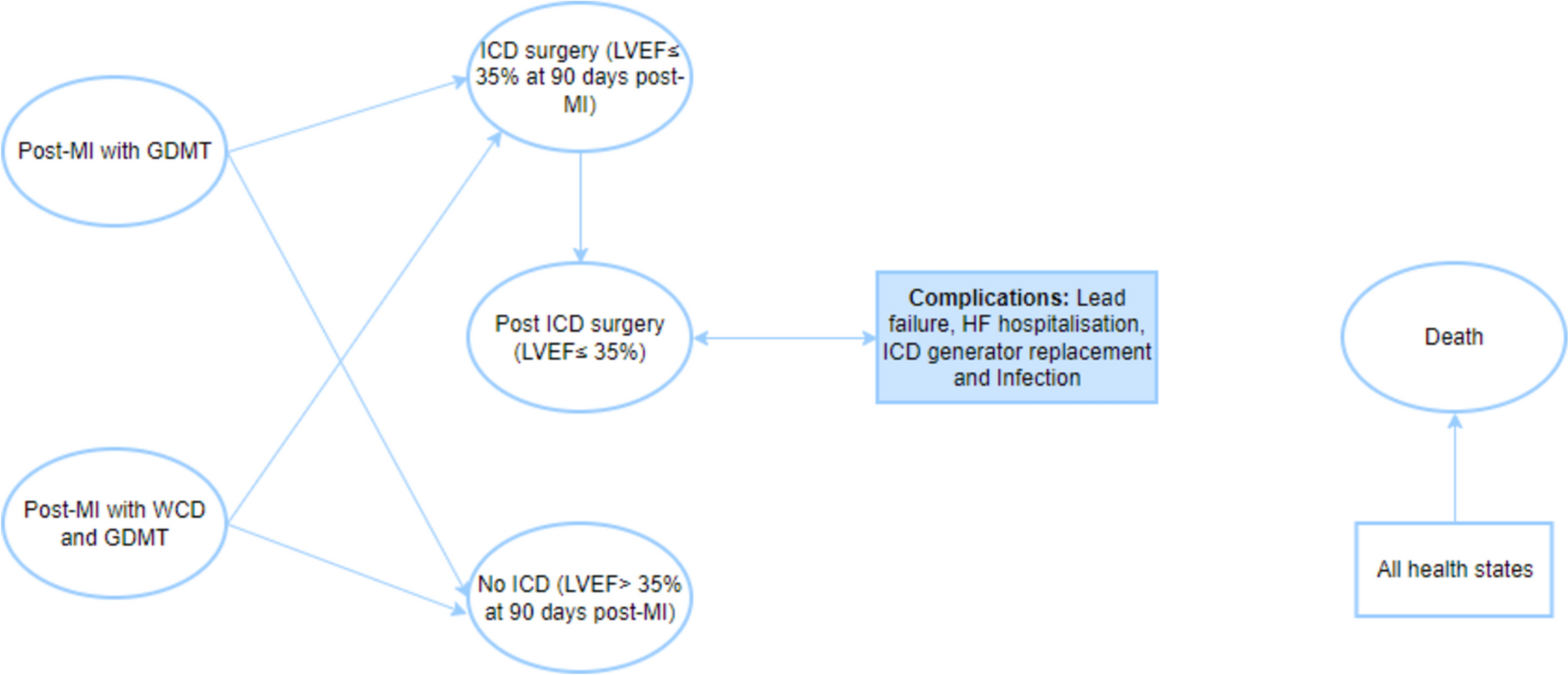
The model followed the Professional Society for Health Economics and Outcomes Research (ISPOR) Task Force for reporting budget impact analysis in health [16]. No discount rates nor adjustment for inflation were considered. The analytical structure of the BIM is reported in Fig. 1.
Fig. 1
Analytical structure of the budget impact model. FIGO International Federation of Gynaecology and Obstetrics, OC ovarian cancer
2.2 Target PopulationThe target population for analysis was adult women with advanced [International Federation of Gynaecology and Obstetrics (FIGO) stage III and IV] high-grade epithelial ovarian, fallopian tube or primary peritoneal cancer who are in complete or partial response to first-line platinum-based chemotherapy and whose cancer is associated with a positive tumour homologous recombination deficiency (HRD) status. However, due the limited access of the HRD test in Argentina at the time of analysis, in the base-case analysis the population was estimated on the basis of a positive BRCA gene test.
In a scenario analysis, we assessed the HDR-positive advanced OC population.
2.3 Epidemiological ParametersThe starting point was a hypothetical cohort of 1,000,000 women. Of these, the incidence of OC was estimated at 97 per 1,000,000 women [18], with 75% being advanced stages (n = 73) [3]. Of these, 67.5% [4] were considered as high-grade serious disease (n = 49). The BRCA test was estimated to be performed for the initial year in 40% of the women. For the following years, we assume an increasing testing rate. Thus, for year 2, year 3, year 4 and year 5, the testing rate is 60%, 80%, 100% and 100%, respectively. The assumption was based on the local clinical oncologist expert opinion. The assumption was relaxed in the sensitivity analysis to estimate the impact of the assumption in the outcomes of the model. It was estimated that 24.1% [19] of these patients are BCRA1 and BCRA2 receptor positive. For both cases, 68% [20] were estimated to have received first-line chemotherapy with bevacizumab and 69% [21] showed a positive response to this treatment.
2.4 Intervention and ComparatorsThe intervention was olaparib in combination with bevacizumab. The dose, frequency and treatment duration were based on the PAOLA-1 trial [7]. The mean duration of treatment with olaparib was equal to 18.14 months, according to the analysis of PAOLA-1 trial [7]. Comparators were chosen on the basis of the current treatment landscape for patients with advanced high-grade epithelial ovarian, fallopian tube or primary peritoneal cancer. In Argentina, bevacizumab is the therapy currently indicated for patients with advanced high-grade epithelial ovarian, fallopian tube or primary peritoneal cancer. The dosing, frequency and treatment duration were based on the trial publication [22].
2.5 Market SharePatients were distributed to the different treatment regimens according to specified current and projected market shares that were estimated by the local clinical oncologist expert opinion. Annual budget impact for olaparib was determined for a current market share analysis (current scenario), in which olaparib had zero market shares versus comparator, and a projected market share analysis (projected scenario), in which olaparib and the comparator treatment had market shares. Market shares are reported according to each healthcare sector of the Argentine health system (third-party public payer, third-party social security payer and third-party private payer). The market share data are reported in Supporting Information Table S1.
2.6 Cost ParametersThe direct medical costs considered in the model were classified into the following categories: testing cost, drug acquisition costs, drug administration costs, monitoring costs and adverse events costs. All costs were estimated in Argentine pesos (ARS) as for October 2022 and were expressed in USD ($1 = 152.59 ARS) [23].
For the base-case analysis, testing costs considered the cost of the BRCA test. Based on the Institute for Clinical Effectiveness and Health Policy (IECS) Unit Cost database [24], the cost of the BRCA test was $351, $640 and $681 for the third-party public payer, third-party social security payer and third-party private payer, respectively.
Drug acquisition costs were obtained from public databases that report the retail price of drugs marketed in Argentina [25]. We used the most recent retail price at the moment to perform the analysis (October 2022), and we converted the retail prices to ex-factory prices by applying the conversion factor suggested by the Argentinian Ministry of Economy [26]. For each drug, the total drug acquisition cost was estimated from the ex-factory prices, the dosage of the therapy administered and the mean duration of treatment. For all drugs, we assumed there was no wastage. The drug acquisition costs are the same for the three healthcare sectors. For drugs administered according to weight, a mean patient weight of 72.62 kg was used. The mean age of patients with OC [7, 8] and the weight information of the women were retrieved using the National Survey for Risk Factors in Argentina [27]. The cost per-pack and monthly treatment costs per-patient for the interventions and comparators are presented in Table 1.
Table 1 Dosage, ex-factory cost per-pack, and monthly treatment cost per-patient for the intervention and comparators. Costs are reported in USD ($)The cost of each intravenous drug administration is estimated for the third-party public payer, the third-party social security payer and the third-party private payer at $73, $116 and $132, respectively. This cost included the use of the oncologic room to administer the drugs. We assume that oral administration has not cost. The costs were estimated on the basis of the IECS Unit Cost database [24].
The monitoring costs and the costs of adverse events were estimated using the micro-costing approach. The identification, rate of use and measurement of health resources used for the disease management were estimated by the opinion of a local expert, and the unit costs by health sector were obtained from the Institute for Clinical Effectiveness and Health Policy (IECS) unit cost database [24]. The health resources include medical consultations (oncologist), laboratory tests (blood count) and images (chest CT scan with contrast). The cost of disease management is presented in Table 2. The unit cost per health resource and the quantities used in the estimation of disease management are available in Supporting Information Table S2.
Table 2 Monthly monitoring costs per-patient for olaparib and the comparator and adverse events management costs, according to the healthcare sector. Costs are reported in USD, 2022The adverse events (AEs) included in the model were hypertension, anaemia, febrile neutropenia and diarrhoea. The included adverse events are grade 3/4 AEs with incidences of greater than 2% and are in line with those reported in the clinical trials for each treatment [7]. The AEs excluded are lymphopenia as it is not considered a treatment-relevant toxicity, and fatigue as it is an adverse event whose management does not require associated clinical practices. The cost per AE is presented in Table 2, and the prevalence rates per AEs are reported in Supporting Information Table S3.
2.7 Model ValidationThe model structure and calculations were reviewed and validated by the research team composed of health economists, a decision-analytic modeller, public health researchers, epidemiologists and a clinical oncologist. All input parameters were initially reviewed and validated by the local clinical oncologist expert. Suggestions for revision and/or adaptation were addressed prior to conducting the analysis.
2.8 Sensitivity AnalysisTo evaluate the effect of uncertainty associated with the parameters of the model on the budget impact results, deterministic (one-way) sensitivity analyses (DSAs) were performed. The parameters were varied according to its confidence interval or, when this information was missing, by ± 20%. For the market shares values, we varied the first-year base-case value by ± 20%. To vary the base-case value for year 2 onward, we used the same variation between year 1 and the rest of the years reported in the base-case values. When necessary for year 2 onward, we capped the market share upper value at 100%.
2.9 Scenario AnalysesTo be eligible to receive olaparib, it is required to test the HRD. However, as the accessibility to the test is limited in Argentina, in our base-case analyses we included patients with BRCA test. Despite that the assumption is not far distant from the Argentinian current clinical practice, we evaluated a scenario where the HRD test is fully available for the population. We assume that 58.3% of the patients who performed the HRD test were positive [7], and we included the cost of the HDR test. All the remaining parameters remained fixed.
To obtain an estimate of the cost for the HRD test in Argentina, an indirect estimation was performed in which the ratio between BRCA test cost and HRD test cost in Uruguay was applied to the cost of the BRCA test in Argentina. The cost estimates were estimated on the basis of the database of the sponsor of the study. Thereby, HRD testing costs for the public sector, social security and the private sector correspond to $1609, $2945 and $3122, respectively.
2.10 Decision Rule—Budgetary Impact ThresholdThis study used the methodology for estimating a threshold of high budgetary impact proposed by Pichón-Riviere and colleagues for countries without their own estimates [28]. According to this report, the reference value of the high budgetary impact threshold is estimated at 0.00016 health spending units (0.00008–0.00024). The estimation of the threshold of high budget impact in Argentina for 2022 was made using the reference value and the estimation of total health expenditure. This latter is estimated using data from the gross domestic product (GDP) and total population of Argentina, and the average of the last 10 available years of healthcare expenditure as a percentage of GDP [29, 30]. The threshold estimation was carried out for each health perspective, using the per capita healthcare expenditures estimated and reported in the study by Espinola and colleagues [31]. Accordingly, it was estimated that the PMPM threshold of high budget impact is $ 0.0153 for the health system. In addition, the per capita healthcare expenditure values were used to quantify conversion factors and thus estimate the threshold of high budget impact for each healthcare sector perspective. So, the PMPM threshold was estimated as $0.0110 for the public sector, $0.0146 for social security and $0.0261 for the private sector.
Comments (0)