In our experience, LNVA behaves similarly to LVA. Both are physiological procedures aimed at enhancing lymphatic drainage, as opposed to debulking techniques. Their effectiveness primarily lies in addressing the fluid component of lymphedema, with limited impact on lymphedema-induced lipodystrophy or fibrosis. Hence, it is crucial during treatment planning to ascertain that patients are still in the fluid-predominant phase of lymphedema and have not progressed to lipodystrophy or fibrosis. In cases where lipodystrophy or fibrosis has already developed, debulking liposuction, with or without skin excision, becomes the preferred treatment approach [16].
Like LVA, LNVA not only provides regional relief but also imparts systemic therapeutic benefits. This means that when performed on a specific part of the body, it can alleviate symptoms in areas beyond the actual site of the procedure. The systemic effects of LNVA are partially elucidated by recent findings on LVA’s immunomodulatory properties, including its ability to reduce exhaustion markers and increase antioxidative capacity [17, 18]. This unique attribute allows for strategic use of both LVA and LNVA. They can be employed either to directly address a readily accessible anatomic region or to remotely treat an area that is too invasive for direct surgical intervention. This approach underpins the success of treating post-traumatic chylothorax [19] and protein-losing enteropathy [20] with groin LNVA, demonstrating the procedure’s versatility and far-reaching impact.
In our practice, LNVA is recommended for patients experiencing fluid edema in the lower abdomen, genitalia, buttocks, and proximal thigh. While LVA directly targeting the affected areas remains a viable option, we have observed more brisk improvements in patients treated with LNVA compared to those undergoing LVA. Our standard approach often involves combining LVA and LNVA, with LVA addressing the leg and LNVA targeting the groin. This combination offers comprehensive coverage of the affected lower extremity and leverages their synergistic effects.
Additionally, LNVA can be effectively paired with debulking liposuction in cases where lymphedema-induced lipodystrophy is primarily localized in the distal segment of the lower extremity. This combined approach is viable when debulking liposuction does not interfere with the groin lymphatics essential for LNVA.
Early in our experience, we adopted Hong et al.’s methodology, employing preoperative MRI for lymph node assessment and lymphoscintigraphy for localization. Although effective, we found this protocol to be burdensome, costly, and time intensive for patients. Intraoperatively, using the gamma probe often led to a ‘field of signal’ from multiple lymph nodes, complicating the identification of a singular, optimal node. This often resulted in inefficient, overly extensive dissection, risking damage to the surrounding delicate lymphatics. Moreover, the radiation safety of this technique remains unverified. Current assumptions about its safety are merely extrapolations from studies on oncologic lymph node extirpations, which typically involve shorter procedures and lymph nodes embedded in adipose tissue. This context differs significantly from our applications, raising concerns about the direct applicability of these safety assumptions.
In response to safety concerns, our first technical modification was to eliminate lymphoscintigraphy. Instead, we started using isosulfan blue and ICG, injected just before surgery, as lymph node markers. However, as expected, these markers proved inconsistent in pinpointing lymph nodes. Their efficacy hinges on the lymphatic system’s ability to transport lymph effectively, a function often compromised in lymphedema patients. As a result, these markers may fail to reach the lymph nodes due to weakened lymphatic transport. Additionally, they tend to highlight all functioning lymph nodes, not just the optimal one for treatment.
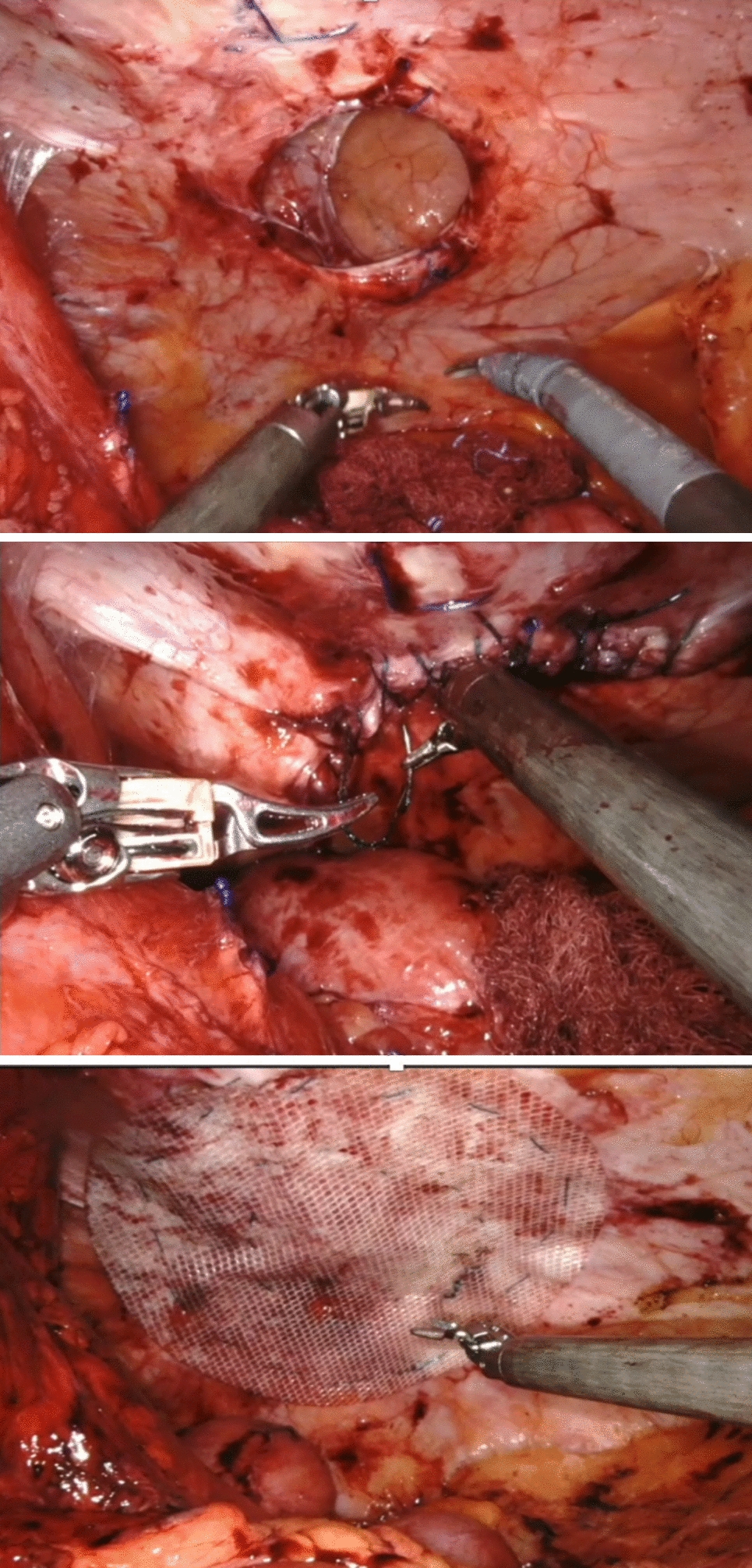
This challenge was resolved by adopting SAVI SCOUT® technology, already prevalent in breast surgery for the extirpation of breast tumors and lymph nodes [15, 21]. Utilizing a small, nonradioactive radar reflector, SAVI SCOUT® allows us to mark a specific lymph node for quick and precise intraoperative identification and dissection, streamlining the process considerably.
Our next challenge was refining the method for identifying the most suitable lymph node for LNVA. Leveraging our proficiency in ultra-high-frequency duplex ultrasound (UHF-DU) for perforator flap and LVA planning, we, in conjunction with our radiologists, explored the effectiveness of UHF-DU at 22 MHz in assessing lymph node morphology and architecture. These characteristics are key indicators of a lymph node’s functional status. For example, the shape of a lymph node—whether oval, round, lobulated, or speculated—can denote a healthy node, one affected by metastasis, a reactive node, or one infiltrated by cancer, respectively [22•]. The visibility of a node’s structural features, such as its capsule, cortex, medulla, and hilar vascularity on UHF-DU, indicates its health and suitability for LNVA. Moreover, this sonographic examination also maps the venous anatomy, enabling preoperative selection of an appropriate vein for LNVA.
Our refined technical approach, which integrates comprehensive preoperative ultra-high-frequency duplex ultrasound (UHF-DU) assessment of both lymph nodes and veins, coupled with precise SAVI SCOUT® marking of the optimal lymph node, has enabled us to consistently perform LNVA with heightened success and efficiency. We anticipate that our techniques will continue to evolve, leading to the development of even more efficient and less invasive methods that may surpass the effectiveness of our current practices. Furthermore, we foresee the application of the LNVA procedure expanding to include lymph nodes in various other regions of the body. This progression marks a promising future in the field of lymphedema treatment, bringing hope for more comprehensive and less burdensome therapeutic options for patients.







Comments (0)