
Remember me


The study was approved by the Ethics Committee of the Medical University of Vienna (EK: 1899/2018) and by the Federal Office for Safety and Healthcare in Austria (EudraCT No: 2018-002972-42), trial registration number: NCT03557138.
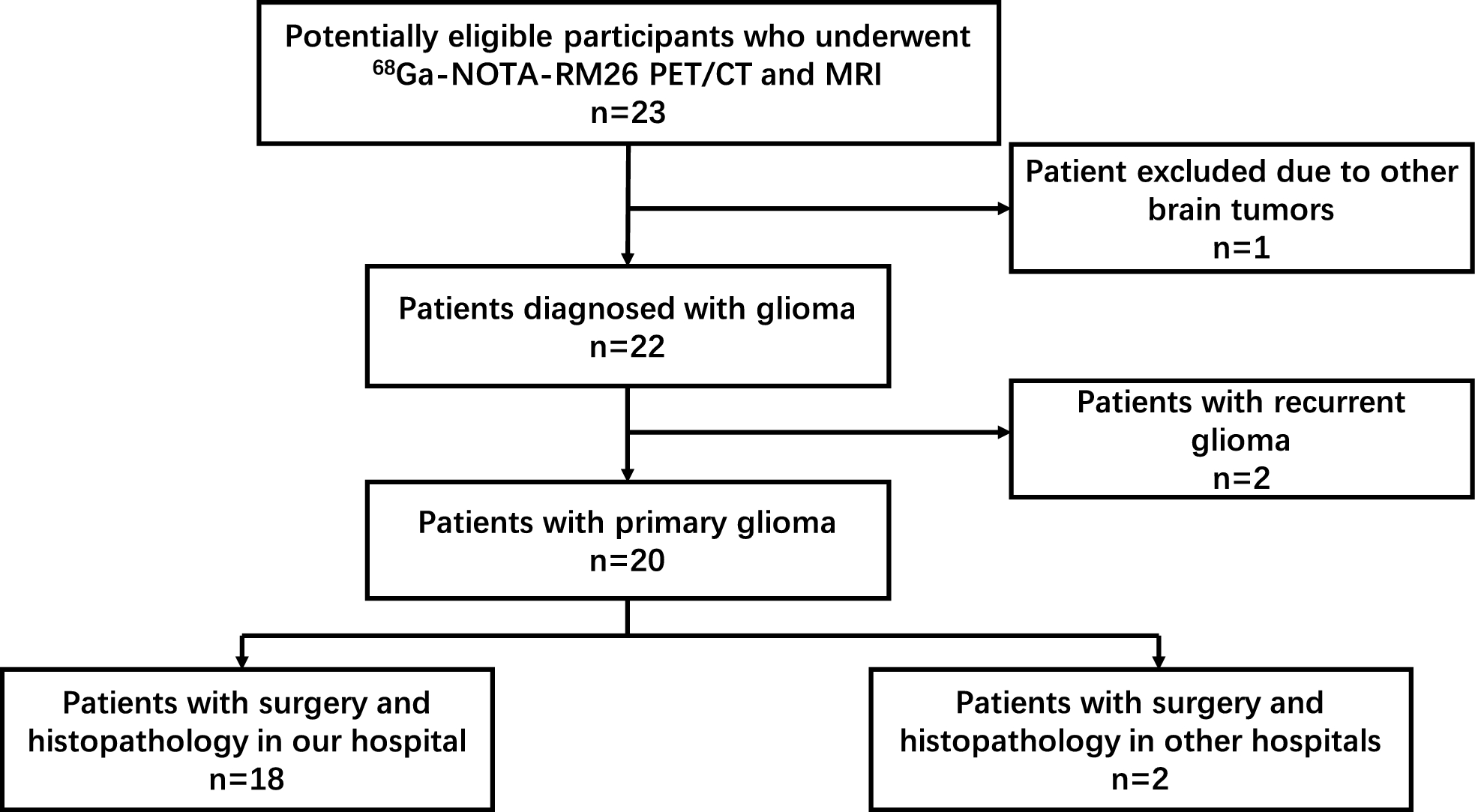
SubjectsAll subjects gave written informed consent and met the inclusion criteria, which were age > 18 and < 75 years, healthy, no previous history of oncological and endocrinological diseases, non-smoker, body mass index (BMI) below 30 kg/m², radiation exposure < 10 mSv within the last 10 years, and written informed consent. Exclusion criteria were any organ dysfunction, claustrophobia, pregnancy, and a positive Covid PCR test. Collectively, five healthy adult subjects (1 male and 4 female) were investigated and met the above-mentioned criteria. Subjects were asked to fast at least 6 h and to empty their bladder immediately before conducting the first PET/CT scan. No further bladder emptying was requested in the first hour of the scanning period.
[18F]Me4FDG radiosynthesis[18F]Me4FDG was prepared in-house following a standardized protocol, using a GE FASTlab synthesizer (GE Healthcare, Boston, MA, USA) with dedicated disposable cassettes on the day of PET imaging. A regular cassette for [18F]FDG was used and prepared as follows: The FDG-precursor-vial was removed and exchanged to a 11 mL crimp-vial, filled with a solution of 10 mg GMP compliant precursor for Me4FDG (β-D-Galactopyranoside, methyl, 2,3,6-triacetate 4-trifluoromethanesulfonate, obtained from ABX advanced biochemical compounds GmbH, Radeberg, Germany) in 2 mL acetonitrile. Full radiopharmaceutical quality control according to the monographs of the European Pharmacopoeia (Ph. Eur.) was thoroughly performed prior the release of the tracer and application to the patient. The prepared cassette lost its GMP compliant due to the manipulation but since a radiosynthesis for a subsequent in-house application at the Vienna General Hospital is exempt from any GMP regulation, this route could be taken.
Examination and safety assessmentA venous cannula was placed in the arm of each subject. Before activity administration, vital parameters were determined by measuring blood pressure, pulse, body temperature. Additionally, one blood sample was drawn for the determination of a full blood count, including kidney, liver and inflammation markers, and one urine sample was collected for the determination of glucose and protein. [18F]Me4FDG was administered as an intravenous bolus injection, followed by a flush with 5 mL of saline solution. Before the injection, subjects were placed in a whole-body PET/CT (Biograph Vision Quadra, Siemens Healthineers) with a 106 cm axial PET field of view. The first acquisition started with injected to obtain a 30 min dynamic scan (rebinned into 15 two-minute frames), followed by 4 static images within four hours starting at 60 min, 150 min, 210 min and 270 min pi. The scan time was adjusted for each time point to account for the decay of [18F] and was 120 s, 210 s, 312 s and 450 s, respectively. A scheme of the imaging procedure is shown in Fig. 1. All PET images were accompanied by an ultra-low-dose CT scan for attenuation correction purposes (Settings: CAREDose4D with ref tube current 10 mAs and ref. tube potential 100 keV, pitch = 1.5, iterative reconstruction using ADMIRE with strength 3). The PET images were reconstructed using an OP-OSEM algorithm with PSF correction and TOF information with 4 iterations and 5 subsets. Matrix size was 440 × 440 resulting in a 1.65 mm²-pixel size. A 3 mm FWHM Gaussian blurring was applied to the reconstructed images. To evaluate toxicity of [18F]Me4FDG, all vital parameters mentioned above were determined after one hour, i.e., a second blood and a second urine sample were obtained, accompanied by a measurement of body temperature and blood pressure. A standard physical examination was performed during the screening visit, any conspicuousness was documented.
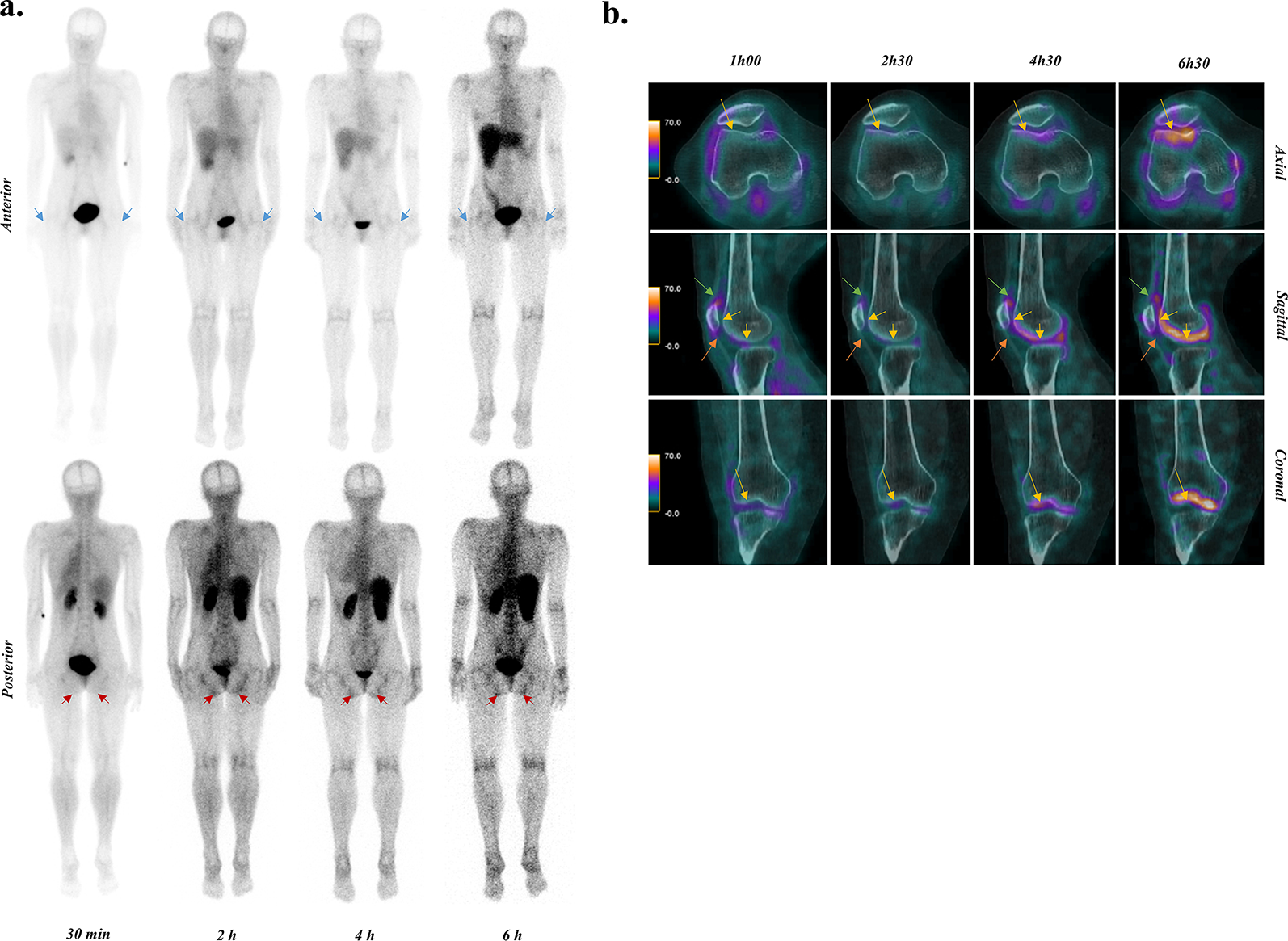
Biodistribution and radiation dosimetryFrom the imaging protocol, static whole-body images were reconstructed from 5 time points (Fig. 1). The PET images were used to evaluate the biodistribution of renal cortices, heart and bladder by measuring the tracer concentration as standardized uptake value (SUV).
Radiation dosimetry was performed with Voxel Dosimetry program (HERMES Medical Solutions, Stockholm, Sweden). Briefly, the 5 time points were first registered to a common reference (the first time point) using a 6-parameter rigid registration algorithm followed by a Demons-type [12] non-rigid registration. Registration was performed using CT images and the transformation parameters and deformation fields were later applied also to PET images. After registration voxel level time-activity curves were generated and integrated to obtain voxel level cumulated activities. Since the first scan data were acquired dynamically starting from time zero, a linear activity grow from zero to the activity at the first time point was chosen. From last time point to infinity, a voxel level mono-exponential fit to the last two time points were made, the half-life from the fit was taken and used that after the last time point, whereas the physical half-life was taken if it was shorter. Voxel level photon tracking and absorbed dose map were performed using a fast Monte Carlo algorithm [13]. From the dose map images, volumes of interest (VOIs) were manually delineated from all organs or areas of the body that could be visually distinguished from the background. These were, brain, subcutaneous tissue of abdomen, breasts, colon ileocecal, gluteus maximus, tongue, lungs (average of left and right lung is presented), vertebral bodies L1-L5, spleen, heart, optical nerves (average of left and right optic nerve is presented), pancreas, liver, bladder as well left and right kidneys. In addition, only an ROI (region of interest) was drawn for the abdominal aorta and inferior vena cava, both at the level of the first lumbar vertebra, because it was not possible to follow the entire course of these vessels. The percentage of radiotracer excreted after one hour was assessed from the scan 60 min post injection by calculating the ratio between total bladder uptake and total body uptake.
Fig. 1
[18F]Me4FDG PET scan schedule
After intravenous injection of [18F]Me4FDG, 5 PET/CT acquisitions were performed, with increasing scanning time from 2 to 7.5 min. The subjects were asked to rest and to void their urinary bladder after one hour.
StatisticsStatistics in this study were limited to descriptive statistics, calculated with Microsoft Excel 2016. Values are presented as mean value plus/minus one standard deviation (SD). Differences between vital parameter were determined using a student’s T-Test.
Comments (0)