
Remember me






In 2021, the CDC estimated that 38.4 million people, or 11.6% of the American population, were living with diabetes.1 Located mainly in the central Appalachian region of the country, the “diabetes belt,” as identified by the CDC, is home to a disproportionate number of people living with diabetes as compared with outside the belt.2 In Virginia, 33 counties fall into the reported “diabetes belt,” with a considerable concentration of people living with diabetes located in the southwestern portion of the state.2 The increased rate of diabetes within this area is multifactorial, with contributing factors including lack of access to primary care providers, healthcare services, and healthy eating options as well as physical inactivity, among other concerns.3 These disparities present challenging situations for both healthcare providers and patients to overcome in order to achieve proper diabetes care in this rural region. Overcoming these challenges is important for individuals with a chronic illness such as diabetes. Self-efficacy is an important factor for promoting positive outcomes in patients with type 2 diabetes mellitus (T2DM).4
The term “self-efficacy” refers to an individual's perceived ability to perform specific behaviors and achieve goals.5 Elevated levels of self-efficacy have been shown to be the cornerstone of effective chronic disease self-management and are a key component of diabetes care.5,6 For a person living with diabetes, these behaviors include, but are not limited to, optimizing physical activity, making healthy dietary choices, and monitoring blood glucose levels with the purpose of adjusting insulin as needed to properly manage the many facets of their chronic condition.4,6 When high levels of efficacy are perceived by the individual, challenges diminish and goals become achievable.
According to Bandura's theory of self-efficacy, individuals must believe that they can perform a specific behavior.7 Mere possession of knowledge and skills is insufficient; confidence in the ability to perform the behavior is crucial, and goal attainment reflects efficacy beliefs for the individual. According to Bandura's theory, self-efficacy affects activities, effort, and persistence. For example, if an individual believes that they can walk 30 minutes per day to improve their blood glucose levels, then they will make this activity a personal goal and maintain a persistent effort to achieve the goal.7 Verbal persuasion is another aspect of Bandura's theory of self-efficacy.5,7 Providers can provide verbal persuasion through frequent, reliable follow-up via telephone and face-to-face communication.
To emphasize the importance of timely management of diabetes, studies have shown that short-term delays in delivery of routine diabetes care are associated with adverse reactions on risk factor control and worse microvascular, macrovascular, and mortality outcomes.8 Furthermore, multiple variables (for example, recurrent lockdowns) during the COVID-19 pandemic led to restricted access to routine diabetes care, which ultimately affected patient self-management, routine follow-up, and access to medications. Although the full impact of the pandemic on people currently living with diabetes has still not been completely recognized, according to a provider survey in the United Kingdom, more than 70% of respondents felt the COVID-19 pandemic had a moderate to significant impact on the ability of their practice to provide routine diabetes care, health checks, or regular screening.9 For these reasons, it is critical for healthcare providers to identify persons living with diabetes who report decreased perceived efficacy in their ability to self-manage their condition and to provide appropriate patient-centered education to correct any existing deficiencies, ultimately empowering patients to develop alternatives and discover solutions to challenges related to their diabetes care.
The program described in this study is based on evidence that has been reported over the years, specifically that (1) uncontrolled diabetes and delays in delivery of routine care have been associated with poorer diabetes-related outcomes; (2) continuous glucose monitoring (CGM) improves glycemic control in diabetes, with reported self-efficacy a strong marker for success; and (3) pharmacist participation, as one part of an interprofessional healthcare team, increases a variety of clinically and economically significant outcomes.6,8,10-14 Thus, with the objective to assess patient self-efficacy in diabetes management while utilizing a CGM system, a family NP, with the assistance of a clinical pharmacist, implemented a CGM program for patients with hemoglobin A1C (A1C) levels higher than 10%. The family NP and clinical pharmacist, located at two primary care clinics in Southwest Virginia, collaborated with another family NP and a medical student working in the same clinics to hypothesize that implementation of CGM combined with medication therapy management and education in this patient population would impact important goals in their diabetes care such as managing A1C values.
Methods Design and sampleThis pilot study was completed to assess self-efficacy in managing diabetes when utilizing a CGM system among patients with diabetes seeking care at two different clinics serving uninsured and underinsured patients in rural Southwest Virginia. Adults 18 years of age and older with an A1C level higher than 10% were invited to participate in this study. This study was reviewed and approved by the University of Pikeville institutional review board (IRB) prior to data collection.
ProceduresParticipants recruited for this study completed the IRB consent form and a presurvey aimed at determining how well they could manage their blood glucose. After completing the consent form, participants were assigned a participant number, and to ensure confidentiality, a list of participant names and their corresponding participant numbers were kept in a locked file cabinet. The pre- and postsurveys were identified by the participants' numbers rather than their names. Participants' health information was secured in an electronic health record system that requires a password for access. After obtaining an initial A1C value, the primary investigator, the family NP, provided each participant with a prescription for a CGM system such as the FreeStyle Libre. The prescription included the reader for the sensor and directions for downloading and using the application for the sensor. After obtaining the sensor either by mail or from the pharmacy, the patient brought the sensor to the office to be inserted. The patient was instructed to wear the sensor for 14 days, and at the end of this period, the sensor was replaced by a new one if the patient chose to continue using the device. Instructions were provided for maintenance of the sensor. The patient was instructed to monitor their blood glucose levels prior to meals and at any moment during which they felt their blood glucose was too low or too high. A1C lab values were monitored prior to insertion of the sensor and again at the 3-, 6-, 9-, and 12-month marks following initiation of the CGM system. One month after the conclusion of the study, each patient was asked to complete the same survey regarding perceived ability to self-manage their diabetes.
As part of the protocol, the clinical pharmacist on the team conducted a complete medication review with every patient at enrollment and, throughout the study, contacted each patient regularly by telephone to provide patient-centered education and counseling. The goals of the telephone encounters were to ensure timely management of medication adjustments, including titration of insulin regimens; to answer any questions that arose about medications or diabetes care; and to prevent any delay in care. Pharmacist-patient encounters were conducted weekly each Friday and documented electronically, and the family NP was alerted to any issues that required attention. In addition to electronic documentation, when warranted, the pharmacist contacted the NP by telephone in order to promote prompt intervention. For example, during weekly telephone encounters with the pharmacist, patients might indicate that they needed a certain medication or medications refilled. In those cases, the pharmacist would then personally contact the NP about the required refill. In turn, the NP could promptly refill medications as needed. Face-to-face interaction between the family NP and clinical pharmacist was limited to once monthly, at which point every participant's progress was reviewed and changes to therapy were made accordingly.
MeasuresSelf-efficacy was measured using the Diabetes Management Self-Efficacy Scale (DMSES), a 20-item Likert-type scale.6 Response format was on a scale of 1 to 5 with 1 representing an answer of “Can't do at all” and 5 representing an answer of “Certain can do,” both in reference to the participant's perception that they could complete a task. Higher scores indicate greater self-efficacy. Internal reliability for this sample was .91. A1C was measured via venipuncture.
Statistical methodsStatistical analysis was based on participant response data using Microsoft Excel version 16.73 to perform measures of central tendency (mean [M]).
ResultsFourteen participants completed pretesting; of those individuals, 10 completed posttesting with the DMSES survey and 11 maintained CGM for 1 year. Among the 14 participants, 100% identified as White, with 71.4% being female, per the survey. The majority of participants were 40 years of age or older. A total of 64.3% reported some high school education; 42.9% reported that they were either employed or disabled; and 78.6% were insured.
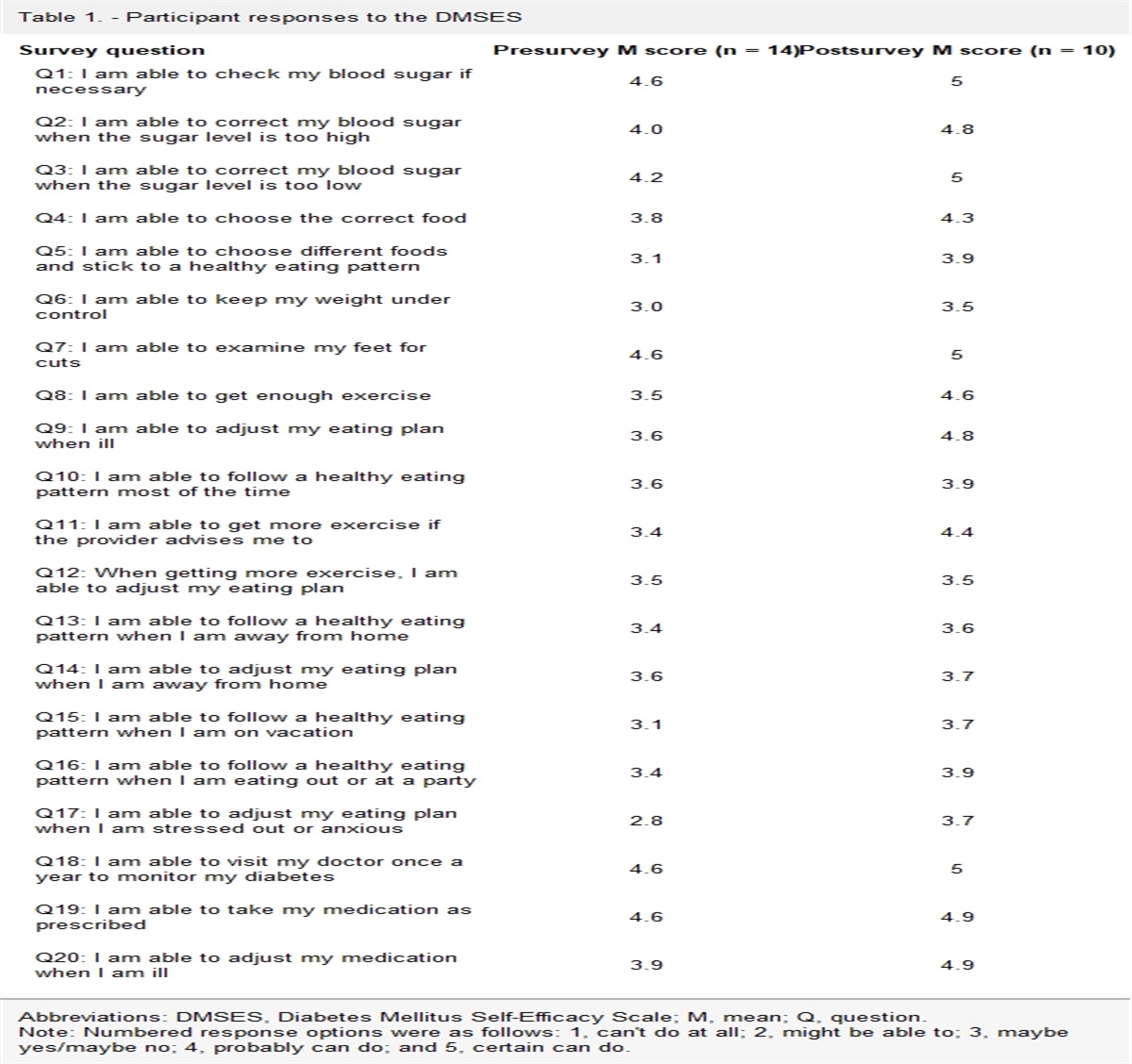
Self-efficacyTable 1 summarizes participant responses to pre- and posttest DMSES scores on individual items. Overall, in comparison with the presurvey results (M of total score = 74.2/100), patients reported an increase in efficacy in managing blood glucose levels while using CGM in the postsurvey (M of total score = 87.1/100). From pre- to postsurvey, the M score increased for every question except one (question [Q] 12: “When getting more exercise, I am able to adjust my eating plan”), for which the M remained the same. The lowest M score on the presurvey (M = 2.8) was for Q17 (“I am able to adjust my eating plan when I am stressed or anxious”); the score for this question increased to M = 3.7 on the postsurvey. Q13 (“I am able to follow a healthy eating pattern when I am away from home”) had the smallest score increase from pre- (M = 3.4) to postsurvey (M = 3.6). Of note, participants reported high efficacy (M > 4.5) in the areas of taking medications as prescribed (Q19), visiting the doctor once per year (Q18), examining feet for cuts (Q7), and checking blood glucose (Q1) before CGM was initiated.
Table 1. - Participant responses to the DMSES Survey question Presurvey M score (n = 14) Postsurvey M score (n = 10) Q1: I am able to check my blood sugar if necessary 4.6 5 Q2: I am able to correct my blood sugar when the sugar level is too high 4.0 4.8 Q3: I am able to correct my blood sugar when the sugar level is too low 4.2 5 Q4: I am able to choose the correct food 3.8 4.3 Q5: I am able to choose different foods and stick to a healthy eating pattern 3.1 3.9 Q6: I am able to keep my weight under control 3.0 3.5 Q7: I am able to examine my feet for cuts 4.6 5 Q8: I am able to get enough exercise 3.5 4.6 Q9: I am able to adjust my eating plan when ill 3.6 4.8 Q10: I am able to follow a healthy eating pattern most of the time 3.6 3.9 Q11: I am able to get more exercise if the provider advises me to 3.4 4.4 Q12: When getting more exercise, I am able to adjust my eating plan 3.5 3.5 Q13: I am able to follow a healthy eating pattern when I am away from home 3.4 3.6 Q14: I am able to adjust my eating plan when I am away from home 3.6 3.7 Q15: I am able to follow a healthy eating pattern when I am on vacation 3.1 3.7 Q16: I am able to follow a healthy eating pattern when I am eating out or at a party 3.4 3.9 Q17: I am able to adjust my eating plan when I am stressed out or anxious 2.8 3.7 Q18: I am able to visit my doctor once a year to monitor my diabetes 4.6 5 Q19: I am able to take my medication as prescribed 4.6 4.9 Q20: I am able to adjust my medication when I am ill 3.9 4.9Abbreviations: DMSES, Diabetes Mellitus Self-Efficacy Scale; M, mean; Q, question.
Note: Numbered response options were as follows: 1, can't do at all; 2, might be able to; 3, maybe yes/maybe no; 4, probably can do; and 5, certain can do.
Scheduled A1C measurements at 3, 6, and 9 months were unattainable for all 11 patients due to a lack of reliable transportation; therefore, many values were missing at the time of analysis. Thus, analysis shifted to compare prestudy (initial) and 12-month values. As noted in Table 2, 9 of 11 patients who used a CGM device achieved a decrease in A1C from the prestudy to the 12-month measurement. One participant could not be reached at 12 months, and therefore, a 12-month A1C measurement is not available for that individual.
Table 2. - Participants' A1C results Participant Initial A1C (%) A1C at 12 months (%) 1 11.7 8.9 2 14.8 7.1 3 10.4 10 4 10.3 9.0 5 10.4 7.6 6 10.6 12.7 7 10.5 10.2 8 10.0 7.6 9 >15.5 10 10.1 7.3 11 >15.5 10.2Abbreviation: A1C, hemoglobin A1C.
Note: The 12-month A1C data point is missing for participant 9 because the individual was lost to follow-up.
In central Appalachia, many obstacles tend to hinder an individual's ability to manage their own health conditions appropriately; thus, any approach that helps to achieve nationally recognized glycemic goals is an approach that is worth the effort, especially when navigating a postpandemic landscape. Overall, results from this pilot study indicate that utilization of CGM devices, in combination with both pharmacotherapy management and education delivered by a family NP and clinical pharmacist, improves patients' perceived self-efficacy in managing blood glucose levels in rural Appalachia. Of note, DMSES questions related to nutrition showed the least improvement in the postsurvey. These findings provide insight into healthy nutrition choices or accessibility as a barrier to adequate blood glucose control, even with CGM and medication management, in this patient population. Future research should address these lifestyle measures and the socioeconomic factors that impact adjustment of eating plans in the “diabetes belt.”
A well-known relationship exists among stress, inability to control food intake, and mental and physical health.15 Patients in this study reported the most difficulty with stress-related dietary intake, as shown by the lowest M score in the presurvey attributed to the question, “I am able to adjust my eating plan when I am stressed out or anxious.” In addition, during telephone encounters with the clinical pharmacist, many patients expressed an inability to afford fresh produce or to manage their diet; therefore, integrating dietary education and behavioral strategies related to stress management during routine encounters theoretically should improve diabetes-related outcomes.
Of interest, this study illustrates a unique interprofessional collaboration between a family NP and clinical pharmacist in a rural, medically underserved area in which regular access to care is limited. To overcome lack of access to care and the many other obstacles that prevent adequate diabetes management, the investigators in this study decided to focus on empowering participants to control their diabetes through self-management and education via the utilization of technology and teamwork. Although this does not represent a novel approach to diabetes care, as multiple studies have shown that CGM use and the addition of a clinical pharmacist to a healthcare team lead to improved diabetes outcomes, the importance of this pilot lies in its emphasis on communication with participants by telephone, not necessarily via in-person communication, to achieve improved results, even if modest.10,12,13 Corresponding with this study's findings, other research has suggested that telephone intervention delivered by various healthcare professionals can be a clinically effective tool to improve diabetes outcomes in diverse populations, indicating that this approach to diabetes care may be one of the many strategies that can be used to improve outcomes.16,17 In addition, the regular, intentional communication between the NP and pharmacist translated to timely targeted interventions, which in any healthcare setting is a prescription for patient success.
As discussed, the findings of this study suggest that future research is needed in this specific healthcare setting in rural Appalachia. Efforts should focus on expanding the number of participants in order to have a larger impact; furthering collaborations between family NPs and clinical pharmacists; incorporating other self-management approaches such as healthy coping strategies; exploring ways to overcome socioeconomic barriers; and possibly engaging other types of healthcare professionals in the care of patients with diabetes, including mental health providers and nutrition specialists.
LimitationsRecruitment for this study occurred in two clinics in rural Southwest Virginia. Population size was a limiting factor for recruitment of patients with uncontrolled T2DM in this study. Because the majority of study participants were female and White residing in rural areas, results cannot be generalized to more diverse populations, including those living in urban settings or areas of greater socioeconomic status. In addition, unique healthcare challenges or social determinants of health for rural communities, such as lack of cell phone signal and transportation difficulties, imposed obstacles on participants that included timely follow-up for A1C measures and postsurvey completion. One participant could not be reached for A1C measurement at the end of the study, and four participants could not be reached for postsurvey completion. Patients' ability to receive CGM devices was also limited due to cost and lack of health insurance, resulting in the recruitment of three participants for the study who ultimately did not utilize CGM systems and were therefore not included in postsurvey or A1C data.
The Hawthorne effect may have contributed to bias in this study, as patients may have behaved in a way that was intended to increase efficacy in managing their diabetes throughout it.18 This social desirability bias in connection with participation in the study could have been a confounding factor, as patients self-reported efficacy through the DMSES. Patients may have increased exercise, checked blood glucose levels more frequently, and/or improved dietary intake during this time, as they were aware that survey results and A1C measurements would be analyzed. To limit this bias, patients were given the opportunity to answer surveys in a private setting and were instructed that results from the surveys would in no way affect their care or healthcare providers' perceptions. In addition, the clinical pharmacist contacted the participants routinely to provide education and to ensure that their monitors were functioning properly. These encounters were encouraging and could have been perceived as coaching or reminders to engage in physical activity and make healthy dietary choices. To minimize this confounding factor and ensure that results would reflect patients' true efficacy in self-managing this chronic disease as much as possible, the study period lasted 1 year between pre- and postsurveys.
ConclusionIt is important to understand the beliefs of patients with T2DM regarding their ability to self-manage blood glucose levels, as their perceptions of self-efficacy may provide insight into barriers affecting proper care. CGM, in conjunction with pharmacotherapy management and education delivered by a family NP and clinical pharmacist, promoted self-efficacy among patients with diabetes in this study. Findings from this study can assist healthcare providers in determining areas in which patients need assistance to manage their diabetes properly. Areas of support include monitoring blood glucose levels, timely management of medications and complications, and patient adherence to recommended therapeutic lifestyle care strategies (for example, dietary choices and physical activity). Future consideration should be given to replication of this study with a larger sample size as well as integration of behavioral health strategies and nutrition education in the care of patients with diabetes.
REFERENCES 1. Centers for Disease Control and Prevention. National Diabetes Statistics Report. www.cdc.gov/diabetes/data/statistics-report/index.html. Accessed March 11, 2024. 2. Barker LE, Kirtland KA, Gregg EW, Geiss LS, Thompson TJ. Geographic distribution of diagnosed diabetes in the U.S.: a diabetes belt. Am J Prev Med. 2011;40(4):434–439. 3. Marshall JF, Thomas L, Lane NM, et al. Health Disparities in Appalachia [Internet]. Appalachian Regional Commission. 2017. www.arc.gov/report/health-disparities-in-appalachia/. 4. Jiang X, Jiang H, Li M, Lu Y, Liu K, Sun X. The mediating role of self-efficacy in shaping self-management behaviors among adults with type 2 diabetes. Worldviews Evid Based Nurs. 2019;16(2):151–160. 5. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. 6. Sturt J, Hearnshaw H, Wakelin M. Validity and reliability of the DMSES UK: a measure of self-efficacy for type 2 diabetes self-management. Prim Health Care Res Dev. 2010;11(4):374–381. 7. Artino AR Jr. Academic self-efficacy: from educational theory to instructional practice. Perspect Med Educ. 2012;1(2):76–85. 8. Khunti K, Aroda VR, Aschner P, et al. The impact of the COVID-19 pandemic on diabetes services: planning for a global recovery. Lancet Diabetes Endocrinol. 2022;10(12):890–900. 9. Seidu S, Hambling C, Holmes P, et al. The impact of the COVID pandemic on primary care diabetes services in the UK: a cross-sectional national survey of views of health professionals delivering diabetes care. Prim Care Diabetes. 2022;16(2):257–263. 10. Maiorino MI, Signoriello S, Maio A, et al. Effects of continuous glucose monitoring on metrics of glycemic control in diabetes: a systematic review with meta-analysis of randomized controlled trials. Diabetes Care. 2020;43(5):1146–1156. 11. Giberson S, Yoder S, Lee MP. Improving Patient and Health System Outcomes through Advanced Pharmacy Practice. A Report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S. Public Health Service. 2011. 12. Henry TM, Smith S, Hicho M. Treat to goal: impact of clinical pharmacist referral service primarily in diabetes management. Hosp Pharm. 2013;48(8):656–661. 13. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-physician collaboration for diabetes care: cardiovascular outcomes. Ann Pharmacother. 2013;47(11):1471–1477. 14. Bluml BM, Watson LL, Skelton JB, Manolakis PG, Brock KA. Improving outcomes for diverse populations disproportionately affected by diabetes: final results of Project IMPACT: Diabetes. J Am Pharm Assoc (2003). 2014;54(5):477–485. 15. Bremner JD, Moazzami K, Wittbrodt M, et al. Diet, stress and mental health. Nutrients. 2020;12(8):2428. 16. Walker EA, Shmukler C, Ullman R, Blanco E, Scollan-Koliopoulus M, Cohen HW. Results of a successful telephonic intervention to improve diabetes control in urban adults: a randomized trial. Diabetes Care. 2011;34(1):2–7. 17. Abughosh SM, Wang X, Serna O, et al. A pharmacist telephone intervention to identify adherence barriers and improve adherence among nonadherent patients with comorbid hypertension and diabetes in a Medicare advantage plan. J Manag Care Spec Pharm. 2016;22(1):63–73. 18. McCarney R, Warner J, Iliffe S, van Haselen R, Griffin M, Fisher P. The Hawthorne Effect: a randomised, controlled trial. BMC Med Res Methodol. 2007;7(1):30.
Comments (0)