
Remember me



Oropharyngeal squamous cell carcinoma (OPSCC) is often associated with the presence of human papillomavirus (HPV), and p16 is a commonly used surrogate marker for HPV.1–3 The prevalence of p16-positive OPSCC varies across different countries and regions and may change with time. The recent approval of the HPV vaccine by the United States Food and Drug Administration for oropharyngeal cancer prevention, as well as the implementation of universal HPV immunization programs, may lead to a decrease in the incidence of p16-positive OPSCC. Nevertheless, the treatment of p16-negative OPSCC should not be overlooked. Investigations into the treatment of this subtype of OPSCC remain crucial to improving oncologic outcomes.
The main distinction between p16-positive and p16-negative OPSCC lies in their response to chemoradiotherapy. Compared to p16-positive OPSCC, p16-negative OPSCC tends to be a poor responder to chemoradiotherapy, which can have a detrimental effect on oncologic outcomes.4 Intensified multimodality treatment can enable better management of p16-negative OPSCC.
Aside from p16, neck stage is another significant prognostic factor for OPSCC. Patients with advanced neck stage have been found to exhibit poorer response to radiotherapy, likely due to the relatively lower responsiveness of large and/or hypoxic lymph node metastases compared to the primary tumor. To address this issue, planned neck dissection (ND) has been included in treatment protocols either independently of treatment response or as a salvage procedure for residual or recurrent nodal disease following chemoradiotherapy for advanced head and neck squamous cell carcinoma. The potential benefits and role of upfront ND (UFND) in patients with clinically node-positive (cN+) p16-negative OPSCC have not been widely explored in the current literature. The available literature on this topic is limited and primarily focuses on head and neck cancer, with a particular emphasis on hypopharyngeal and OPSCC cases, regardless of p16 status.5–7 Therefore, the aim of the present study is to investigate the possible advantages of UFND in patients with cN+ p16-negative OPSCC.
2. METHODSThe retrospective study was approved by the institutional research ethics committee of Taipei Veterans General Hospital (TPEVGH IRB No.: 2020-04-013AC), and the requirement for informed consent from patients was waived. Between January 1, 2011, and September 30, 2019, the medical records of 213 newly diagnosed patients with p16-negative OPSCC who received curative treatment at Taipei Veterans General Hospital, a single tertiary referral hospital in Taipei, Taiwan were reviewed. Among these patients, 114 had clinical neck metastasis. We excluded patients who did not complete the entire treatment course or were not followed up for more than 3 months (n = 10), had simultaneous or prior head and neck malignancy (n = 17), or had distant metastasis (n = 11) at the time of diagnosis. Ultimately, data from 76 patients with cN+ p16-negative OPSCC were included in the analysis. The mean follow-up duration was 50.4 months (range: 5.6-140.6 months). Clinicopathological data and tumor characteristics were recorded from hospital registries.
All patients underwent standard pretreatment evaluations for staging, which were determined by a multidisciplinary team comprising radiologists, medical oncologists, radiation oncologists, and head and neck surgeons using the seventh edition of the American Joint Committee on Cancer/Union for International Cancer Control TNM staging classification. During the meeting, the largest diameters of lymph nodes were measured in the long axis and recorded as the maximal neck size in this review. Based on the image study, necrotic metastatic nodes are characterized by thicker walls and irregular, complex central low attenuation. In contrast, the definition of cystic nodes entails homogeneous fluid content without internal complex, irregular, or solid areas, and an enhancing capsule <2 mm in thickness.8
The curative treatment was determined using a shared decision-making approach involving the patients, their families, and attending physicians. The treatment plan for neck disease was concluded based on the patient’s preference, either definite concurrent chemoradiotherapy (CCRT group) or upfront surgery including ND followed by chemoradiotherapy (UFND group). The extent of ND was determined based on preoperative imaging studies and the conclusion of a multidisciplinary meeting.
Standard radiotherapy performed at our hospital includes intensity-modulated radiation therapy (IMRT) with standard fractionation according to the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology for Head and Neck Cancer. The planned total dose of radiotherapy was >60 Gy (2.0 Gy/d) to the primary tumor region and involved nodal stations. For the purposes of this review, the radiation dose for the primary tumor was defined as the total dose of radiotherapy to the primary tumor region (primary tumor site or postoperative tumor bed), and the dose for the neck metastasis was defined as the total dose to the involved nodal stations.
IMRT was combined with cisplatin-based triweekly chemotherapy or weekly targeted therapy with cetuximab in this review. Targeted therapy with cetuximab is covered by National Health Insurance for patients aged 70 years and older and those with serum creatinine clearance <50 mL/min, hearing impairment, or intolerance to cisplatin-based chemotherapy.
After treatment completion, regular follow-up was performed once a month in the first year, once every 2 months in the second year, and once every 3 months after the third year. The first imaging follow-up was conducted 2 to 3 months after the completion of CCRT. After that, follow-up imaging was scheduled every 6 to 12 months until 5 years after completion of CCRT. Functional results were determined based on the patient’s dependence on feeding and tracheostomy tubes at their last follow-up.
The causes of death are ultimately documented and categorized into locoregional disease, distant metastasis, second primary malignancy, and pneumonia. As local and regional diseases can sometimes be difficult to distinguish, they are grouped together under the same cause of death. Furthermore, if a patient passes away due to carotid blowout syndrome, this too will be attributed to a locoregional disease-related cause of death.
2.1. Statistical analysisCategorical variables across groups were compared using the Pearson Chi-squared test or Fisher exact test when the number was <5. Parametrically distributed continuous data were compared using the unpaired Student’s t test. Cumulative regional recurrence-free survival (RRFS), disease-specific survival (DSS), and overall survival (OS) were determined using the Kaplan-Meier method, and these three survivals were measured from the start of treatment. The Log-Rank test was used to statistically compare the survival curves between the UFND and CCRT groups.
Variables that achieved statistical significance (p < 0.05) or those that were close to significance (p < 0.1) by univariate Cox proportional hazard model were subsequently included in the multivariate analysis using a forward stepwise Cox regression model.
To address potential confounding factors, a propensity analysis was performed using logistic regression to generate a propensity score for patients who received UFND or CCRT. The propensity model included variables that were associated with treatment decisions. The model was then used to match UFND and CCRT groups on a one-to-one basis using the nearest-neighbor matching method. Survival analysis was repeated for each matched subgroup to evaluate the effect of UFND on oncologic outcomes while adjusting for confounding factors. Statistical significance was set at a two-tailed p < 0.05. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 20 for Windows, SPSS Inc., Chicago, IL).
3. RESULTS 3.1. Patient demographics and tumor-related characteristicsOf the 76 patients reviewed, 96.1% (73/76) were male, with a mean age of 56.3 years (range 38-89 years). The majority of patients had a history of cigarette smoking (90.8%) and alcohol consumption (73.7%). Approximately half had the habit of betel-quid chewing (52.6%). The most common location of the primary tumor was the palatine tonsil (67.1%, 51/76), followed by the tongue base (18.4%, 14/76), soft palate (9.2%, 7/76), posterior pharyngeal wall (3.9%, 3/76), and vallecula (1.3%, 1/76).
Based on the treatment modality, the CCRT group consisted of 49 patients, while the UFND group had 27 patients. Within the UFND group, 92.6% (25/27) of cases underwent ipsilateral NDs, while only 7.4% (2/27) underwent bilateral NDs. After undergoing ND, 40.7% (11/27) of patients were diagnosed with a higher pathologic N stage than their original clinical N stage. Pathological reports of 11 out of 27 patients (40.7%) showed extranodal extension (ENE). Among these 11 cases, only 45.5% (5/11) were initially diagnosed with ENE through staging imaging.
Among the cohort of 73 patients who underwent systemic treatment, the majority (78.1%, 57/73) received cisplatin-based chemotherapy, while a subset of 12 patients (16.4%) were treated with cetuximab-targeted therapy. Two patients (2.7%) received a combination of targeted therapy and cisplatin-based chemotherapy, and the remaining two patients (2.7%) were administered cisplatin in conjunction with immunotherapy.
The baseline characteristics of the patients in the two treatment groups are presented in the left column of Table 1. The UFND group had a statistically significant higher proportion of male patients (88.9% vs 100%) and significantly earlier clinical T stage (T1-2, 100% vs 46.9%). Additionally, the UFND group received significantly lower radiation doses over the primary tumor and neck field (both p = 0.000). However, other factors, including age, personal habits, clinical N stage, overall staging, maximal size of neck metastasis, ENE, necrotic or cystic nodal change of lymph nodes shown on the image, and functional outcomes (long-term tube feeding and tracheostomy tube), did not reach statistical significance.
Table 1 - Patient demographics and tumor-related characteristics in the UFND and CCRT groups before and after matching by propensity analysis Before propensity score matching After propensity score matching UFNDCCRT = concurrent chemoradiotherapy; cGy = centigray; ENE = extranodal extension; RT = radiotherapy; UFND = upfront neck dissection.
Due to significant differences in clinical T stage between the UFND and CCRT groups, propensity analysis using a one-to-one nearest-neighbor matched method was conducted to minimize selection bias. The variables entered in the propensity model were age, sex, clinical T stage, and N stage. The propensity analysis matched 23 patients in each group, and the aforementioned confounding factors were well-matched between the two groups (Table 1, right column).
3.2. Causes of deathTable 2 displays the causes of death for each group following propensity score-matched analysis. In the UFND group, 17.4% (4/23) of patients died due to distant metastasis, while 4.3% of patients died of locoregional disease. Out of the four cases that died of distant metastasis, 50% (2/4) had ENE upon pathological analysis. In the CCRT group, 21.7% of patients died due to aspiration pneumonia, 8.7% of patients died of locoregional disease, and 4.3% died of distant metastasis. No patients in either group died as a result of a second primary malignancy. It is noteworthy that patients in the CCRT group had a significantly higher risk of dying from aspiration pneumonia (p = 0.049), while there was no significant difference in other factors between the two groups.
Table 2 - Causes of death in the UFND and CCRT groups after propensity score-matched analysis Cause of death, No. (%) UFND groupCCRT = concurrent chemoradiotherapy; UFND = upfront neck dissection.
The median follow-up duration for all cases was 53.3 months (range, 5.6-140.6) in the UFND group and 45.6 months (range, 6.7-130.7) in the CCRT group. In the UFND group, 25.9% (7/27) of cases experienced relapse, including seven cases of local recurrence (25.9%), one case of regional recurrence (3.7%), and five cases of distant recurrence (18.5%). In contrast, 38.8% (19/49) of cases in the CCRT group experienced relapse, including eight cases of local recurrence (16.3%), 13 cases of regional recurrence (26.3%), and six cases of distant recurrence (12.2%).
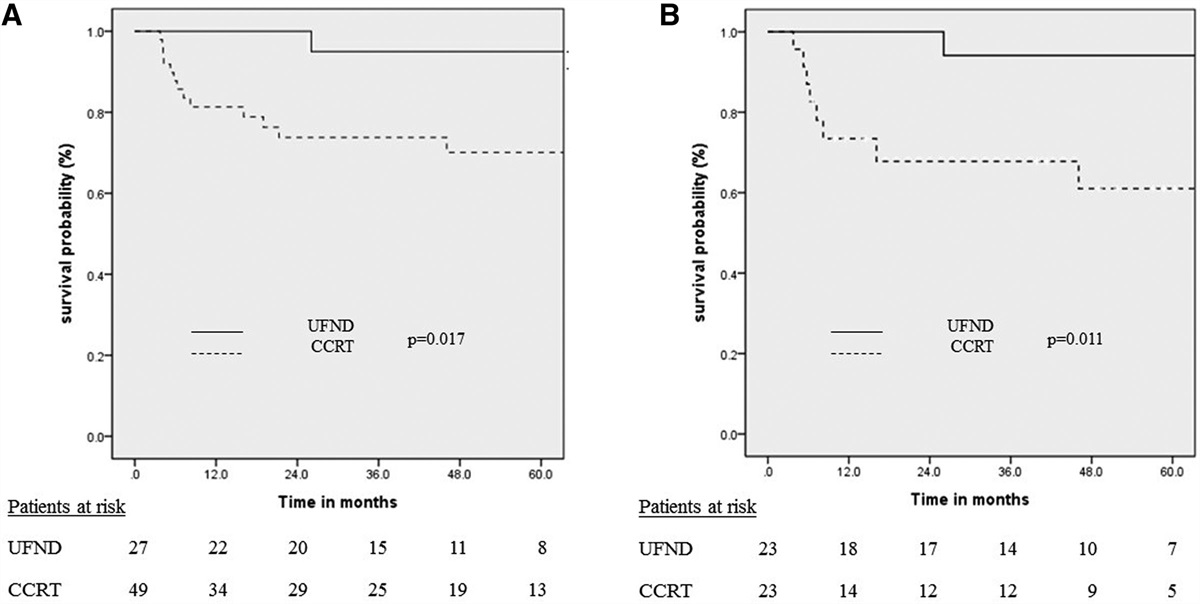
The comparative analysis revealed a statistically significant difference in the 5-year RRFS rate between the UFND and CCRT groups (95.0% vs 70.1%, p = 0.017) (Fig. 1A). However, there were no statistically significant differences in the 5-year DSS and OS rates between the two groups (5-year DSS: 80.8% vs 74.8%, p = 0.656; 5-year OS: 70.4% vs 60.1%, p = 0.549) (Figs. 2A and 3A).
 Fig. 1:
Fig. 1: A comparative analysis of the 5-y regional recurrence-free survival of cN+ p16-negative OPSCC revealed a statistically significant difference in the UFND or CCRT groups before (95.0% vs 70.1%, p = 0.017) (A) and after propensity score matching (94.1% vs 61.0%, p = 0.011) (B). CCRT = concurrent chemoradiotherapy; cN+ = clinically node-positive; OPSCC = oropharyngeal squamous cell carcinoma; UFND = upfront neck dissection.
 Fig. 2:
Fig. 2: The comparative analysis of the 5-y disease-specific survival rates between the UFND and CCRT groups, respectively, revealing no statistically significant differences (80.8% vs 74.8%, p = 0.656) (A). The results of propensity score-matched analysis still demonstrated no statistically significant differences between the two groups (77.3% vs 64.8%, p = 0.482) (B). CCRT = concurrent chemoradiotherapy; UFND = upfront neck dissection.
 Fig. 3:
Fig. 3: In the comparative analysis of the 5-y overall survival rates between the UFND and CCRT groups, no statistically significant differences were observed (70.4% vs 60.1%, p = 0.549) (A). The results of propensity score-matched analysis also demonstrated no statistically significant differences between the two groups (73.9% vs 61.7%, p = 0.515) (B). CCRT = concurrent chemoradiotherapy; UFND = upfront neck dissection.
After propensity score-matched analysis, 5-year RRFS was still better in the UFND group (94.1% vs 61.0%, p = 0.011) (Fig. 1B). There were still no statistically significant differences in the 5-year DSS and OS rates between the two groups (5-year DSS: 77.3% vs 64.8%, p = 0.482; 5-year OS: 73.9% vs 61.7%, p = 0.515) (Figs. 2B and 3B).
3.4. Factors associated with survival by univariate and multivariate analysesAmong all of the 76 p16-negative OPSCC patients, univariate analysis revealed that UFND was the sole factor associated with regional control, as shown in Table 3. Clinical T stage, N stage, primary tumor excision, ENE, and necrotic or cystic lymph nodes shown on image were not found to be significantly associated with RRFS. Given that all other factors had a p > 0.1, multivariate analysis was not performed. After propensity score matching analysis of the 46 patients, univariate analysis also revealed that UFND was the only factor related to regional control. Furthermore, none of the specific factors were associated with DSS in the univariate Cox proportional hazard model (Table 4). Similarly, no factors were found to be linked to OS in all p16-negative OPSCC patients. After propensity score matching analysis, only clinical T stage was found to have an impact on OS (Table 5). Similarly, because none or only one factor had a p < 0.1 in the univariate Cox proportional hazard model, multivariate analysis was not conducted.
Table 3 - Factors associated with regional recurrence-free survival by univariate Cox proportional hazard model before and after matching by propensity analysis Variables Before propensity score matching After propensity score matching Univariate Univariate HR (95% CI) p HR (95% CI) p Clinical T stage T1-T2 Reference Reference T3-T4 1.092 (0.366-3.261) 0.875 1.000 (0.000-686946.909) 1.000 Clinical N stage N1-N2a Reference Reference N2b-N3 4.390 (0.574-33.598) 0.154 28.933 (0.029-29301.862) 0.341 Overall staging 3 Reference Reference 4 2.362 (0.309-18.065) 0.408 23.701 (0.002-303289.761) 0.512 Treatment group CCRT Reference Reference UFND 0.126 (0.016-0.960) 0.046 0.110 (0.014-0.879) 0.037 Primary tumor excision No Reference Reference Yes 0.432 (0.120-1.550) 0.198 0.274 (0.057-1.322) 0.107 ENE upon image No Reference Reference Yes 2.047 (0.709-5.911) 0.186 1.402 (0.350-5.611) 0.633 Necrotic lymph node No Reference Reference Yes 1.609 (0.539-4.804) 0.394 1.181 (0.317-4.401) 0.805 Cystic lymph node No Reference Reference Yes 0.438 (0.098-1.960) 0.280 0.699 (0.145-3.371) 0.656CCRT = concurrent chemoradiotherapy; ENE = extranodal extension; HR = hazard ratio; UFND = upfront neck dissection.
CCRT = concurrent chemoradiotherapy; ENE = extranodal extension; HR = hazard ratio; LN = lymph node; UFND = upfront neck dissection.
Comments (0)