
Remember me



Attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) are both neurodevelopmental conditions that manifest at an early age. Individuals with ADHD exhibit symptoms such as inattention, hyperactivity, impulsivity, risk-taking behavior and poor judgment compared with healthy individuals, which can lead to an increased susceptibility to injury, stress or traumatic events (Adler et al., 2004). ASD, on the other hand, is a severe disorder that affects approximately one in 59 children. It is characterized by deficits in social interaction, verbal and nonverbal communication and restricted and repetitive patterns of behavior, interests or activities (Baio et al., 2018).
Individuals with ASD often struggle to cope with novel or environmental stressors (Anesiadou et al., 2021). The symptoms and functional deficits of both ADHD and ASD typically persist throughout an individual’s lifespan. These two disorders also have a high comorbidity rate and share some common symptoms, such as executive function deficits, lower social skills and attention deficits (Ghirardi et al., 2018). Additionally, ADHD and ASD share both overlapping and distinct genetic underpinnings (Baranova et al., 2022; Cao et al., 2022; Rao et al., 2022). A genetic correlation between ADHD and ASD has been identified (rg = 0.37) (Cao et al., 2022). As individuals with ADHD and ASD age, they are also more likely to develop other psychiatric comorbidities (Baranova et al., 2022; Rao et al., 2022). Furthermore, individuals with these developmental disorders may be three times more likely to experience traumatic events (Reiter et al., 2007).
Post-traumatic stress disorder (PTSD) is characterized by a cluster of symptoms (intrusion symptoms, avoidance, negative alterations in cognitive function and mood and hypervigilance) that impair the individual’s function after exposure to traumatic events of catastrophic intensity or an extraordinary threat (Al Jowf et al., 2022). Globally, approximately 2.9–10% of people suffer from PTSD, making it a significant public health concern (Qassem et al., 2021).
Extensive research suggests that the stress systems of ASD, ADHD and PTSD are abnormal, including dysregulation in the diurnal rhythm of the hypothalamic-pituitary-adrenal (HPA) axis and HPA axis sluggishness in response to stressors (Angeli et al., 2018; Anesiadou et al., 2021; Corbett et al., 2021). Observational studies have found a bidirectional association between ADHD and PTSD (Spencer et al., 2016). For instance, ADHD in combat soldiers increases the risk of developing PTSD (Adler et al., 2004; Biederman et al., 2014; Howlett et al., 2018), and individuals with PTSD often exhibit ADHD symptoms during childhood (Gurvits et al., 2000). Moreover, individuals with ASD are more likely to experience traumatic events, which subsequently serve as risk factors for developing PTSD (Haruvi-Lamdan et al., 2018). Research has shown that individuals with ASD are more susceptible to displaying symptoms of or being diagnosed with full-blown PTSD (Brenner et al., 2018; Rumball et al., 2020). One study found that 72% of autistic adults experienced interpersonal trauma, with 44% meeting the diagnostic criteria for PTSD (Reuben et al., 2021).
ADHD, ASD and PTSD are complex disorders influenced by multiple factors, including genetics and environmental factors (Maihofer et al., 2022; Genovese and Butler, 2023). Family, twin, adoption and genome-wide association studies (GWAS) have demonstrated that all three psychiatric disorders have high heritability rates, with higher concordance rates among siblings of probands, and involve a multitude of genes (Gilman et al., 2011; Risch et al., 2014; Faraone and Larsson, 2019). Studies have primarily focused on neurotransmitter pathways when examining the genetics of ADHD (Sudre et al., 2023). Several genes, such as KIAA0040, MYO1G, CRISPLD1 and ADAMTS9, have been found to be differentially expressed in the brains of individuals with ADHD and have also been implicated in other mental disorders (Sudre et al., 2023). In ASD, approximately 50% of cases involve chromosome deletions or duplications (Genovese and Butler, 2023). A large-scale sequencing study identified 102 risk genes relating to ASD, including KCNQ3, DEAF1, SCN1A and SLC6A1. (Satterstrom et al., 2020). Twin studies estimated that genetic factors contributed to 30–40% of the variance in PTSD (Banerjee et al., 2017), while a meta-analysis of a genome-wide association study found the heritability range to be between 5 and 20% (Nievergelt et al., 2019).
In recent years, Mendelian randomization (MR) analysis has been frequently employed to explore causal relationships between various diseases (Baranova et al., 2023a,2023b,2023c; Cao et al., 2023). However, limited data exists regarding the genetic associations between ADHD/ASD and PTSD. Given the shared characteristics mentioned above, we sought to test the hypothesis that ADHD and ASD are associated with PTSD. Therefore, this study aimed to investigate the genetic relationships between these disorders using MR analysis.
Methods Data sources and study designThis study utilized publicly available GWAS summary results of ADHD, ASD and PTSD in individuals of European descent. The ADHD dataset included 38 691 cases and 275 986 controls (Demontis et al., 2023). The ASD dataset included 18 381 cases and 27 969 controls (Grove et al., 2019). The GWAS summary results for PTSD included 23 212 cases and 151 447 controls (Nievergelt et al., 2019). The study compared single-nucleotide polymorphisms (SNPs) alleles across the ADHD, ASD and PTSD datasets and implemented quality control measures, such as removing SNPs with a minor allele frequency >0.42 and harmonizing allele and effect directions across datasets.
Genetic correlation analysisGenetic correlations between ADHD/ASD and PTSD were calculated using linkage disequilibrium score regression. The linkage disequilibrium structure for European populations was estimated using the 1000 Genome Project phase 3 data.
Mendelian randomization analysisThe primary analyses utilized the inverse-variance weighted (IVW) method. Sensitivity analyses were also performed using the weighted median and MR-Egger methods, which were implemented in TwoSampleMR (Hemani et al., 2018). The weighted median and MR-Egger methods were used to evaluate the pleiotropy and heterogeneous instrumental variants. The MR-Egger regression intercept term was used to test for pleiotropy (Bowden et al., 2015). If the MR-Egger intercept of the linear regression model is close to 0 (P > 0.05), it suggests no pleiotropy in the instrumental variants, supporting the validity of the exclusion hypothesis; conversely, if it deviates significantly from 0, it suggests the presence of genetic pleiotropy and invalidates the exclusion hypothesis. The significance threshold for identifying associations between ADHD/ASD and PTSD was set at an false discovery rate < 0.05 using the IVW method. In each MR analysis, instrumental variants were selected as SNPs with genome-wide significance (P < 5 × 10−8) and were further pruned using a clumping r2 cutoff of 0.01. If fewer than 10 instrumental variants surpassed the threshold, a P value threshold of 1 × 10−5 was used.
Results Genetic correlation analysisThe genetic correlation analysis revealed highly positive correlations of PTSD with ADHD (rg = 0.70; P = 1.04 × 10−20), and ASD (rg = 0.34; P = 1.13 × 10−4).
Mendelian randomization analysisThe number of SNPs used as instrumental variants is listed in Table 1. The primary MR analysis using the IVW method indicated the causal effects of ADHD and ASD on PTSD.
Table 1 - Causal relationship of ADHD and ASD with PTSD Exposure Outcome Method b (se) OR (95%CI) N_IV P_IV Q_P I 2 Egger_intercept P_pleiotropy P FDR ADHD PTSD IVW 0.135 (0.040) 1.14 (1.06–1.24) 26 5.00E-08 0.058 0.324 NA NA 7.88E-04 3.15E-03 ADHD PTSD WM 0.079 (0.055) 1.08 (0.97–1.20) 26 5.00E-08 NA NA NA NA 0.151 NA ADHD PTSD MR-Egger −0.049 (0.123) 0.95 (0.75–1.21) 26 5.00E-08 0.094 0.254 0.004 0.128 0.695 NA ASD PTSD IVW 0.043 (0.017) 1.04 (1.01–1.08) 60 1.00E-05 0.016 0.302 NA NA 0.014 0.028 ASD PTSD WM 0.046 (0.022) 1.05 (1.00–1.09) 60 1.00E-05 NA NA NA NA 0.038 NA ASD PTSD MR-Egger 0.048 (0.049) 1.05 (0.95–1.16) 60 1.00E-05 0.013 0.301 0 0.914 0.337 NA PTSD ADHD IVW 0.077 (0.048) 1.08 (0.98–1.19) 29 1.00E-05 3.88E-03 0.461 NA NA 0.11 0.147 PTSD ADHD WM 0.012 (0.054) 1.01 (0.91–1.13) 29 1.00E-05 NA NA NA NA 0.832 NA PTSD ADHD MR-Egger 0.035 (0.112) 1.04 (0.83–1.29) 29 1.00E-05 2.93E-03 0.458 0.001 0.686 0.755 NA PTSD ASD IVW 0.009 (0.064) 1.01 (0.89–1.15) 36 1.00E-05 0.492 −0.015 NA NA 0.884 0.884 PTSD ASD WM −0.005 (0.093) 1.00 (0.83–1.20) 36 1.00E-05 NA NA NA NA 0.961 NA PTSD ASD MR-Egger −0.037 (0.155) 0.96 (0.71–1.31) 36 1.00E-05 0.449 −0.018 0.001 0.746 0.815 NAADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; CI, confidence interval; IVW, inverse variance weighted; FDR, false discovery rate; N_IV: number of instrumental variables; OR, odds ratio; PTSD, posttraumatic stress disorder; Q_P: Cochran’s P value of heterogeneity analysis; WM, weighted median.
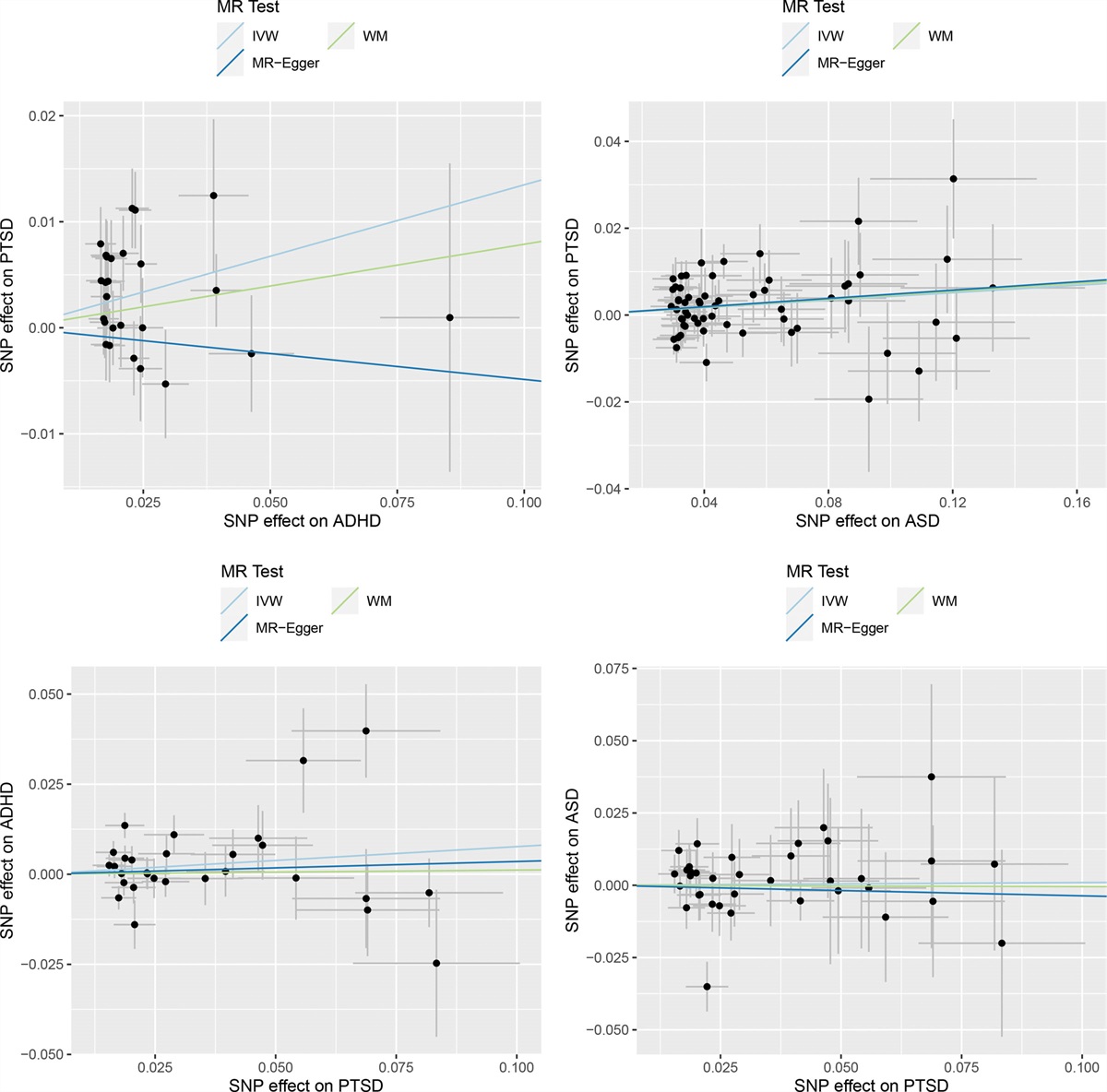
Analysis showed that ADHD was associated with an increased risk of PTSD [odds ratio (OR) = 1.14; 95% confidence interval (CI), 1.06–1.24; P = 7.88 × 10−4) (Table 1). Sensitivity analyses using the weighted median showed similar estimates (OR = 1.08; CI, 0.97–1.20; P = 0.151). However, the MR-Egger model yielded an opposite direction (OR = 0.95; CI, 0.75–1.21; P = 0.695). Due to the higher power of the IVW method, the results from IVW were considered final. Scatter plots depicting the association between ADHD and PTSD for the instrumental variants were presented in Fig. 1, with colored lines representing different regression analyses. Cochran’s Q statistic indicated no evidence of pleiotropy (Q = 37; P = 0.058) across instrument effects.
 Fig. 1:
Fig. 1: Scatter plots of MR analyses using three models to investigate causal relationships between ADHD, ASD and PTSD. The trait on the x-axis denotes exposure, the trait on the y-axis denotes outcomes, and each cross point represents an instrumental variant. ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; MR, Mendelian randomization; PTSD, posttraumatic stress disorder.
Analysis showed that ASD was associated with an increased risk of PTSD (OR = 1.04; CI, 1.01–1.08; P = 0.014) (Table 1 and Fig. 1). Sensitivity analyses using the weighted median showed similar estimates (OR = 1.05; CI, 1.00–1.09; P = 0.038), as did the MR-Egger models (OR = 1.05; CI, 0.95–1.16; P = 0.337). Cochran’s Q statistic suggested the presence of pleiotropy (Q = 84.47; P = 0.016) across instrument effects.
In the reverse MR analysis, genetic liability to PTSD did not have a causal effect on ADHD (OR = 1.08; CI, 0.98–1.19) or ASD (OR = 1.01; CI, 0.89–1.15) (Table 1 and Fig. 1).
DiscussionAn MR study revealed genetic correlations between ADHD and PTSD phenotypes (rg = 0.43–0.52), with ADHD being causally linked with an increased risk of PTSD (β = 0.367; CI, 0.186–0.552) (Wendt et al., 2023). Our analysis, using the latest and largest GWAS data on ADHD, showed a high correlation between ADHD and PTSD (rg = 0.70) at the genetic level. ADHD conferred a causal effect on the development of PTSD (OR = 1.14).
Individuals with ADHD are more susceptible to experiencing trauma, such as physical injuries and abuse (Koenen et al., 2007). Cross-sectional studies have also found a high prevalence of ADHD among individuals with PTSD (Spencer et al., 2016). Longitudinal studies have indicated that children with ADHD have a higher risk of developing PTSD in the next 10 years (Biederman et al., 2014). In addition, US Army soldiers with preexisting ADHD deployed to Afghanistan were associated with a doubled risk of postdeployment PTSD (Howlett et al., 2018). Both ADHD and PTSD exhibit structural and functional abnormalities in brain regions and endocrine factors (Martínez et al., 2016). Preliminary studies suggested that both disorders shared common polymorphisms in the dopamine transporter gene and cannabinoid gene (Lu et al., 2008; Onaivi, 2009; Spencer et al., 2013). The genetic overlap of the two disorders aligns with their shared symptoms, including attention and concentration difficulties, attention shift, impulsive behavior, irritability and executive function impairments (Biederman et al., 2013; Martínez et al., 2016). Dysfunctions in the HPA axis and inflammatory biomarkers have been observed in both ADHD and PTSD, characterized by lower cortisol levels and disrupted cortisol rhythms (Al Jowf et al., 2021; Chang et al., 2021). Lower cortisol levels have been correlated with hyperactivity in ADHD and hyperarousal/flashback in PTSD (Kaneko et al., 1993). Another MR study found low morning plasma cortisol levels associated with ADHD (Jue et al., 2023). Psychostimulants used for ADHD treatment may also be effective for PTSD (Barreto et al., 2022). The mechanism of psychostimulants’ effectiveness could involve decreased dopamine activity and increased catecholamine release in certain brain regions (Houlihan, 2011).
In our study, we also found a correlation between ASD and PTSD (rg = 0.34) at the genetic level, with ASD conferring a causal effect on PTSD (OR = 1.04).
Individuals with ASD are more vulnerable to maltreatment, abuse, bullying, serious physical injuries and extended psychiatric hospitalization, increasing their risk of developing post-traumatic symptoms (Sterzing et al., 2012; Lobregt-van Buuren et al., 2021). Studies have demonstrated that disease-related disasters and quarantine for ASD can increase the risk of PTSD (Sprang and Silman, 2013; Cénat et al., 2021). During the COVID-19 pandemic, individuals with ASD exhibited increased sleep difficulties, aberrant behaviors, irritability, tantrums, anxiety and lethargy (Arazi et al., 2022; Hall et al., 2023). Childhood sexual abuse has been found to impact brain function in adults with ASD, as evidenced by altered event-related potential components and P300 amplitudes (Okazaki et al., 2020). Research on gene expression in cord blood has shown that maternal psychological distress and adverse childhood experiences increase the risk of neurodevelopmental disorders (Breen et al., 2018). In ASD, a compromised HPA axis leads to insufficient stress response, resulting in delayed cortisol secretion and low cortisol levels, similar to the dysregulation observed in PTSD (Makris et al., 2021). These findings suggest impaired stress systems in ASD and provide a potential explanation for the increased risk of PTSD.
LimitationsThere are several limitations to this study. First, the data used are primarily from individuals of European descent, limiting the generalizability of the results to other populations. International collaborations are needed to validate these findings across diverse populations. Second, although we identified causal relationships between ADHD/ASD and PTSD, the exact mechanisms by which genes influence the pathology of these disorders remain unclear. Further research is needed to elucidate these mechanisms. Finally, ADHD, ASD and PTSD are influenced by a complex interplay of genetic and environmental factors. Understanding how other factors contribute to the development of these disorders is crucial.
ConclusionOur study contributes to understanding the genetic relationships between ADHD/ASD and PTSD. We found that ADHD and ASD may increase the risk of developing PTSD, but not vice versa.
AcknowledgementsWe thank all investigators and participants for contributing their genetics. We also thank members of the consortia, who generously shared the GWAS data.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
F.Z. conceived the project, supervised the study and analyzed the data. F.Z., W.Y., H.C., Y.S. and A.B. wrote the manuscript. All authors read and approved the final manuscript.
Conflicts of interestThere are no conflicts of interest.
References Adler LA, Kunz M, Chua HC, Rotrosen J, Resnick SG (2004). Attention-deficit/hyperactivity disorder in adult patients with posttraumatic stress disorder (PTSD): is ADHD a vulnerability factor? J Atten Disord 8:11–16. Al Jowf GI, Snijders C, Rutten BPF, de Nijs L, Eijssen LMT (2021). The molecular biology of susceptibility to post-traumatic stress disorder: highlights of epigenetics and epigenomics. Int J Mol Sci 22:10743. Al Jowf GI, Ahmed ZT, An N, Reijnders RA, Ambrosino E, Rutten BPF, et al. (2022). A public health perspective of post-traumatic stress disorder. Int J Environ Res Public Health 19:6474. Anesiadou S, Makris G, Michou M, Bali P, Papassotiriou I, Apostolakou F, et al. (2021). Salivary cortisol and alpha-amylase daily profiles and stress responses to an academic performance test and a moral cognition task in children with neurodevelopmental disorders. Stress Health 37:45–59. Angeli E, Korpa T, Johnson EO, Apostolakou F, Papassotiriou I, Chrousos GP, et al. (2018). Salivary cortisol and alpha-amylase diurnal profiles and stress reactivity in children with attention deficit hyperactivity disorder. Psychoneuroendocrinology 90:174–181. Arazi A, Koller J, Zachor DA, Golan O, Sadaka Y, Eytan D, et al. (2022). Home-quarantine during the initial Covid-19 outbreak in Israel: parent perceived impact on children with ASD. Heliyon 8:e09681. Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z, et al. (2018). Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill Summ 67:1–23. Banerjee SB, Morrison FG, Ressler KJ (2017). Genetic approaches for the study of PTSD: advances and challenges. Neurosci Lett 649:139–146. Baranova A, Wang J, Cao H, Chen J-H, Chen J, Chen M, et al. (2022). Shared genetics between autism spectrum disorder and attention-deficit/hyperactivity disorder and their association with extraversion. Psychiatry Res 314:114679. Baranova A, Cao H, Teng S, Su KP, Zhang F (2023a). Shared genetics and causal associations between COVID-19 and multiple sclerosis. J Med Virol 95:e28431. Baranova A, Chandhoke V, Cao H, Zhang F (2023b). Shared genetics and bidirectional causal relationships between type 2 diabetes and attention-deficit/hyperactivity disorder. Gen Psychiatr 36:e100996. Baranova A, Zhao Y, Cao H, Zhang F (2023c). Causal associations between major depressive disorder and COVID-19. Gen Psychiatr 36:e101006. Barreto C, Vila Irigoyen A, Lopez O, Gralnik L (2022). Psychostimulants for the treatment of comorbid post-traumatic stress disorder (PTSD) in a patient with attention-deficit/hyperactivity disorder (ADHD): a case report and literature summary. Cureus 14:e28199. Biederman J, Petty CR, Spencer TJ, Woodworth KY, Bhide P, Zhu J, et al. (2013). Examining the nature of the comorbidity between pediatric attention deficit/hyperactivity disorder and post-traumatic stress disorder. Acta Psychiatr Scand 128:78–87. Biederman J, Petty C, Spencer TJ, Woodworth KY, Bhide P, Zhu J, et al. (2014). Is ADHD a risk for posttraumatic stress disorder (PTSD)? Results from a large longitudinal study of referred children with and without ADHD. World J Biol Psychiatry 15:49–55. Bowden J, Davey Smith G, Burgess S (2015). Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol 44:512–525. Breen MS, Wingo AP, Koen N, Donald KA, Nicol M, Zar HJ, et al. (2018). Gene expression in cord blood links genetic risk for neurodevelopmental disorders with maternal psychological distress and adverse childhood outcomes. Brain Behav Immun 73:320–330. Brenner J, Pan Z, Mazefsky C, Smith KA, Gabriels R; Autism and Developmental Disorders Inpatient Research Collaborative (ADDIRC) (2018). Behavioral symptoms of reported abuse in children and adolescents with autism spectrum disorder in inpatient settings. J Autism Dev Disord 48:3727–3735. Cao H, Wang J, Baranova A, Zhang F (2022). Classifying major mental disorders genetically. Prog Neuropsychopharmacol Biol Psychiatry 112:110410. Cao H, Baranova A, Song Y, Chen JH, Zhang F (2023). Causal associations and genetic overlap between COVID-19 and intelligence. QJM 116:766–773. Cénat JM, Blais-Rochette C, Kokou-Kpolou CK, Noorishad P-G, Mukunzi JN, McIntee S-E, et al. (2021). Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res 295:113599. Chang JP, Su KP, Mondelli V, Pariante CM (2021). Cortisol and inflammatory biomarker levels in youths with attention deficit hyperactivity disorder (ADHD): evidence from a systematic review with meta-analysis. Transl Psychiatry 11:430. Corbett BA, Muscatello RA, Kim A, Patel K, Vandekar S (2021). Developmental effects in physiological stress in early adolescents with and without autism spectrum disorder. Psychoneuroendocrinology 125:105115. Demontis D, Walters GB, Athanasiadis G, Walters R, Therrien K, Nielsen TT, et al.; ADHD Working Group of the Psychiatric Genomics Consortium (2023). Genome-wide analyses of ADHD identify 27 risk loci, refine the genetic architecture and implicate several cognitive domains. Nat Genet 55:198–208. Faraone SV, Larsson H (2019). Genetics of attention deficit hyperactivity disorder. Mol Psychiatry 24:562–575. Genovese A, Butler MG (2023). The autism spectrum: behavioral, psychiatric and genetic associations. Genes (Basel) 14:677. Ghirardi L, Brikell I, Kuja-Halkola R, Freitag CM, Franke B, Asherson P, et al. (2018). The familial co-aggregation of ASD and ADHD: a register-based cohort study. Mol Psychiatry 23:257–262. Gilman SR, Iossifov I, Levy D, Ronemus M, Wigler M, Vitkup D (2011). Rare de novo variants associated with autism implicate a large functional network of genes involved in formation and function of synapses. Neuron 70:898–907. Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al.; Autism Spectrum Disorder Working Group of the Psychiatric Genomics Consortium (2019). Identification of common genetic risk variants for autism spectrum disorder. Nat Genet 51:431–444. Gurvits TV, Gilbertson MW, Lasko NB, Tarhan AS, Simeon D, Macklin ML, et al. (2000). Neurologic soft signs in chronic posttraumatic stress disorder. Arch Gen Psychiatry 57:181–186. Hall CL, Partlett C, Valentine AZ, Pearcey S, Sayal K (2023). Understanding the impact of home confinement on children and young people with ADHD and ASD during the COVID-19 pandemic. Child Psychiatry Hum Dev 12:1–15. Haruvi-Lamdan N, Horesh D, Golan O (2018). PTSD and autism spectrum disorder: co-morbidity, gaps in research, and potential shared mechanisms. Psychol Trauma 10:290–299. Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D, et al. (2018). The MR-Base platform supports systematic causal inference across the human phenome. Elife. 7:e34408. Houlihan DJ (2011). Psychostimulant treatment of combat-related posttraumatic stress disorder. J Psychopharmacol 25:1568–1572. Howlett JR, Campbell-Sills L, Jain S, Heeringa SG, Nock MK, Sun X, et al. (2018). Attention deficit hyperactivity disorder and risk of posttraumatic stress and related disorders: a prospective longitudinal evaluation in US Army Soldiers. J Trauma Stress 31:909–918. Jue H, Fang-Fang L, Dan-Fei C, Nuo C, Chun-Lu Y, Ke-Pin Y, et al. (2023). A bidirectional Mendelian randomization study about the role of morning plasma cortisol in attention deficit hyperactivity disorder. Front Psychiatry 14:1148759. Kaneko M, Hoshino Y, Hashimoto S, Okano T, Kumashiro H (1993). Hypothalamic-pituitary-adrenal axis function in children with attention-deficit hyperactivity disorder. J Autism Dev Disord 23:59–65. Koenen KC, Moffitt TE, Poulton R, Martin J, Caspi A (2007). Early childhood factors associated with the development of post-traumatic stress disorder: results from a longitudinal birth cohort. Psychol Med 37:181–192. Lobregt-van Buuren E, Hoekert M, Sizoo B (2021). Autism, adverse events, and trauma. In: Grabrucker AM, editor. Autism spectrum disorders. Exon Publications Copyright: The Authors. Lu AT, Ogdie MN, Järvelin MR, Moilanen IK, Loo SK, McCracken JT, et al. (2008). Association of the cannabinoid receptor gene (CNR1) with ADHD and post-traumatic stress disorder. Am J Med Genet B Neuropsychiatr Genet 147B:1488–1494. Maihofer AX, Choi KW, Coleman JRI, Daskalakis NP, Denckla CA, Ketema E, et al. (2022). Enhancing discovery of genetic variants for posttraumatic stress disorder through integration of quantitative phenotypes and trauma exposure information. Biol Psychiatry 91:626–636. Makris G, Agorastos A, Chrousos GP, Pervanidou P (2021). Stress system activation in children and adolescents with autism spectrum disorder. Front Neurosci 15:756628. Martínez L, Prada E, Satler C, Tavares MC, Tomaz C (2016). Executive dysfunctions: the role in attention deficit hyperactivity and post-traumatic stress neuropsychiatric disorders. Front Psychol 7:1230. Nievergelt CM, Maihofer AX, Klengel T, Atkinson EG, Chen C-Y, Choi KW, et al. (2019). International meta-analysis of PTSD genome-wide association studies identifies sex- and ancestry-specific genetic risk loci. Nat Commun 10:4558. Okazaki K, Ota T, Makinodan M, Kishimoto N, Yamamuro K, Ishida R, et al. (2020). Associations of childhood experiences with event-related potentials in adults with autism spectrum disorder. Sci Rep 10:13447. Onaivi ES (2009). Cannabinoid receptors in brain: pharmacogenetics, neuropharmacology, neurotoxicology, and potential therapeutic applications. Int Rev Neurobiol 88:335–369. Qassem T, Aly-ElGabry D, Alzarouni A, Abdel-Aziz K, Arnone D (2021). Psychiatric co-morbidities in post-traumatic stress disorder: detailed findings from the adult psychiatric morbidity survey in the English Population. Psychiatr Q 92:321–330. Rao S, Baranova A, Yao Y, Wang J, Zhang F (2022). Genetic relationships between attention-deficit/hyperactivity disorder, autism spectrum disorder, and intelligence. Neuropsychobiology 81:484–496. Reiter S, Bryen DN, Shachar I (2007). Adolescents with intellectual disabilities as victims of abuse. J Intellect Disabil 11:371–387. Reuben KE, Stanzione CM, Singleton JL (2021). Interpersonal trauma and posttraumatic stress in autistic adults. Autism Adulthood. 3:247–256. Risch N, Hoffmann TJ, Anderson M, Croen LA, Grether JK, Windham GC (2014). Familial recurrence of autism spectrum disorder: evaluating genetic and environmental contributions. Am J Psychiatry 171:1206–1213. Rumball F, Happé F, Grey N (2020). Experience of Trauma and PTSD symptoms in autistic adults: risk of PTSD development following DSM-5 and Non-DSM-5 traumatic life events. Autism Res 13:2122–2132. Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An J-Y, et al.; Autism Sequencing Consortium (2020). Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell 180:568–584.e23. Spencer TJ, Biederman J, Faraone SV, Madras BK, Bonab AA, Dougherty DD, et al. (2013). Functional genomics of attention-deficit/hyperactivity disorder (ADHD) risk alleles on dopamine transporter binding in ADHD and healthy control subjects. Biol Psychiatry 74:84–89. Spencer AE, Faraone SV, Bogucki OE, Pope AL, Uchida M, Milad MR, et al. (2016). Examining the association between posttraumatic stress disorder and attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. J Clin Psychiatry 77:72–83. Sprang G, Silman M (2013). Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med Public Health Prep 7:105–110. Sterzing PR, Shattuck PT, Narendorf SC, Wagner M, Cooper BP (2012). Bullying involvement and autism spectrum disorders: prevalence and correlates of bullying involvement among adolescents with an autism spectrum disorder. Arch Pediatr Adolesc Med 166:1058–1064. Sudre G, Gildea DE, Shastri GG, Sharp W, Jung B, Xu Q, et al. (2023). Mapping the cortico-striatal transcriptome in attention deficit hyperactivity disorder. Mol Psychiatry 28:792–800. Wendt FR, Garcia-Argibay M, Cabrera-Mendoza B, Valdimarsdóttir UA, Gelernter J, Stein MB, et al.; Post-Traumatic Stress Disorder Working Group of the Psychiatric Genomics Consortium (2023). The relationship of attention-deficit/hyperactivity disorder with posttraumatic stress disorder: a two-sample Mendelian randomization and population-based sibling comparison study. Biol Psychiatry 93:362–369.
Comments (0)