
記住我
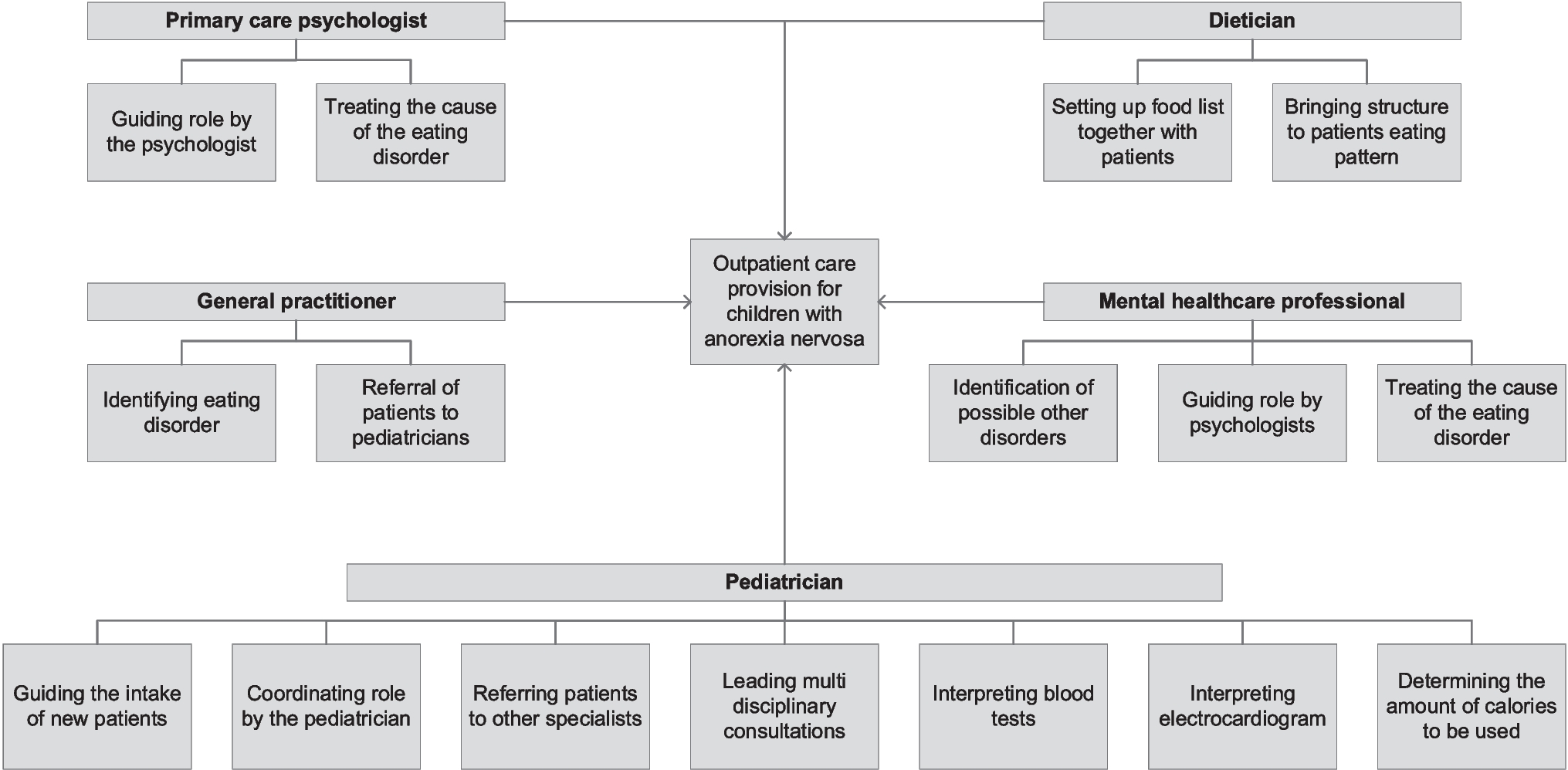
We were able to describe the healthcare practices in modular terms based on the interview data and collected documents. During outpatient care provision for children with AN, the child meets various healthcare professionals. From a modular perspective, the individual consultations with the various professionals comprise the modules. Examples of modules are ‘Consultation with the Pediatrician’ and ‘Consultation with the Dietician’. To illustrate: “We [pediatricians] do not provide the care alone, we also have the support of experienced dietitians who are involved in care provision for children with anorexia nervosa and have a great sense for these children” – Respondent A.
Components are elements of healthcare provision that have a distinct function but cannot function independently: they are offered as part of the module, in our case, the consultation. The components are based on guidelines, protocols, and screening forms used in outpatient care provision for children with AN; they are offered as part of a module. The components prescribe what kind of activities are being carried out during a consultation [module]. Examples of components are ‘Nutritional needs’, ‘Somatic state’, and ‘Physical examination’. To illustrate: “During the first visit, I always perform a blood test as standard element [component] of the consultation [module] to see, based on blood values, whether a child is suffering from not eating much. An electrocardiogram is also exemplary of an element [component] that I always perform” – Respondent B.
The six hospitals studied offered four to five different modules, wherein various components were distinguished (a comprehensive picture of the modular composition of outpatient care provision for children with AN as delivered by Hospital A is provided in Fig. 1; a comprehensive picture of the modular composition of the other five participating hospitals is shown in Appendix 4 (Figs. 2, 3, 4, 5 and 6).
Fig. 1
Modular composition of outpatient care provision for children with AN in Hospital A
We also found several communication mechanisms that connected the modules (i.e. the individual consultations). Using a modular perspective, these communication mechanisms are defined as interfaces. The majority of interfaces contributed to the flow of information in outpatient care provision as they helped to manage and guide interaction between the healthcare professionals involved. Multidisciplinary meetings, referral letters, electronic health record (EHR) reports, and direct communication lines (mail, phone call, instant messaging) are examples of interfaces that guide information-flow. For example, the referral letter ensures that information about a patient’s health status is being transferred from one professional to another, both within and outside of the hospital. We also identified interfaces like protocols, guidelines, and screening forms that guide professionals’ judgment in the selection of appropriate components for each child, ensuring that outpatient care provision meets the needs of each individual child. The identified interfaces highlight the interdependency of the involved healthcare professionals in outpatient care provision for children with AN. For example, when new information becomes available about a child (e.g. evidence of abuse), the pediatrician will inform the other professionals about the new information via the EHR or a referral letter.
Supporting continuity of care in outpatient care provision for children with anorexia nervosaBy explicitly decomposing outpatient care provision into modules, components, and interfaces, we were able to recognize how modularity can support the three essential parts of COC.
First, informational continuity is related to the availability of a child’s medical history, at all times, for each professional. Although the EHR ensures easy and quick access to a child’s medical history, not all professionals have direct access to the EHR. The professionals without access to the EHR need to actively request information from the healthcare professionals or patients and parents/caregivers, resulting in professionals sometimes lacking information. To illustrate: “I [pediatrician] cannot access the files of the psychologists and it does matter that I know what the psychologist is doing and vice versa” – Respondent B. The modular perspective explicitly highlighted this issue, since no (active) information exchange [interface] was present, for example, between the pediatrician and the psychiatrist, resulting in missed information during consultations. Actively exchanging information would ensure no information is lost, increasing efficiency of the consultation, and would result in supported informational continuity.
Second, relational continuity refers to the familiarity between professionals, children and their parents/caregivers. Respondents argued that they all try to realize relational continuity in care provision by ensuring that there is a dedicated professional for each child, resulting in lasting patient-professional relationships. For example, one pediatrician argued that seeing the same child multiple times makes consultations more effective and efficient and increases the level of trust: “By seeing the same child, consultations could become more efficient and would not have to take long, whereas if the child visits my colleague [pediatrician] and me interchangeably, there might be redundant information exchange possible” – Respondent A. This is especially relevant because it is quite an intense and emotional care trajectory for children and parents/caregivers, and it is important to establish levels of trust between all involved parties. However, relational continuity is at risk when healthcare professionals are temporarily absent, and the child needs to visit another healthcare professional. Respondents argued that there is no multidisciplinary workbook [interface] available that they can use to inform their fellow colleagues on the working methods in outpatient care provision for children with AN. The availability of such a workbook would improve the relational continuity of outpatient care provision.
Last, a lack of management continuity has been observed because for example, the pediatrician, general practitioner, and psychiatrist all have separate care plans, separate EHRs, and work in different organizations resulting in potentially missing or overlapping information and treatment. Management continuity refers to the extent to which the provided care is perceived as coherent, coordinated, and unduplicated. Respondents argued that it is not always clear for patient and parents/caregivers what element of care will be performed by whom: “Although most of us [pediatricians] focus on medical care and less so on psychological or psychiatric care, we have to incorporate those elements into our consultation to obtain an overall view of the patient in front of us. This might be confusing for patients because the information might also be obtained elsewhere” – Respondent A. Not only is this confusing for patients and parents/caregivers, but also for professionals themselves as the content of healthcare provision was not prescribed in detail for each professional, resulting in different professionals who ended up doing the same thing or not doing it at all according to a pediatrician: “I do not have a clear overview [modules and components] of what truly happens in mental care for example, which also limits me in that sense in my healthcare provision” – Respondent F. Having decomposed and allocated the different aspects of the professional’s work, it is possible to identify identical and missing components in care provision for children with AN, which would support management continuity.
留言 (0)