
記住我
This retrospective study was conducted at a single center and involved 131 children who underwent FBN1 screening due to suspicion of Marfan syndrome between 2016 and 2021.
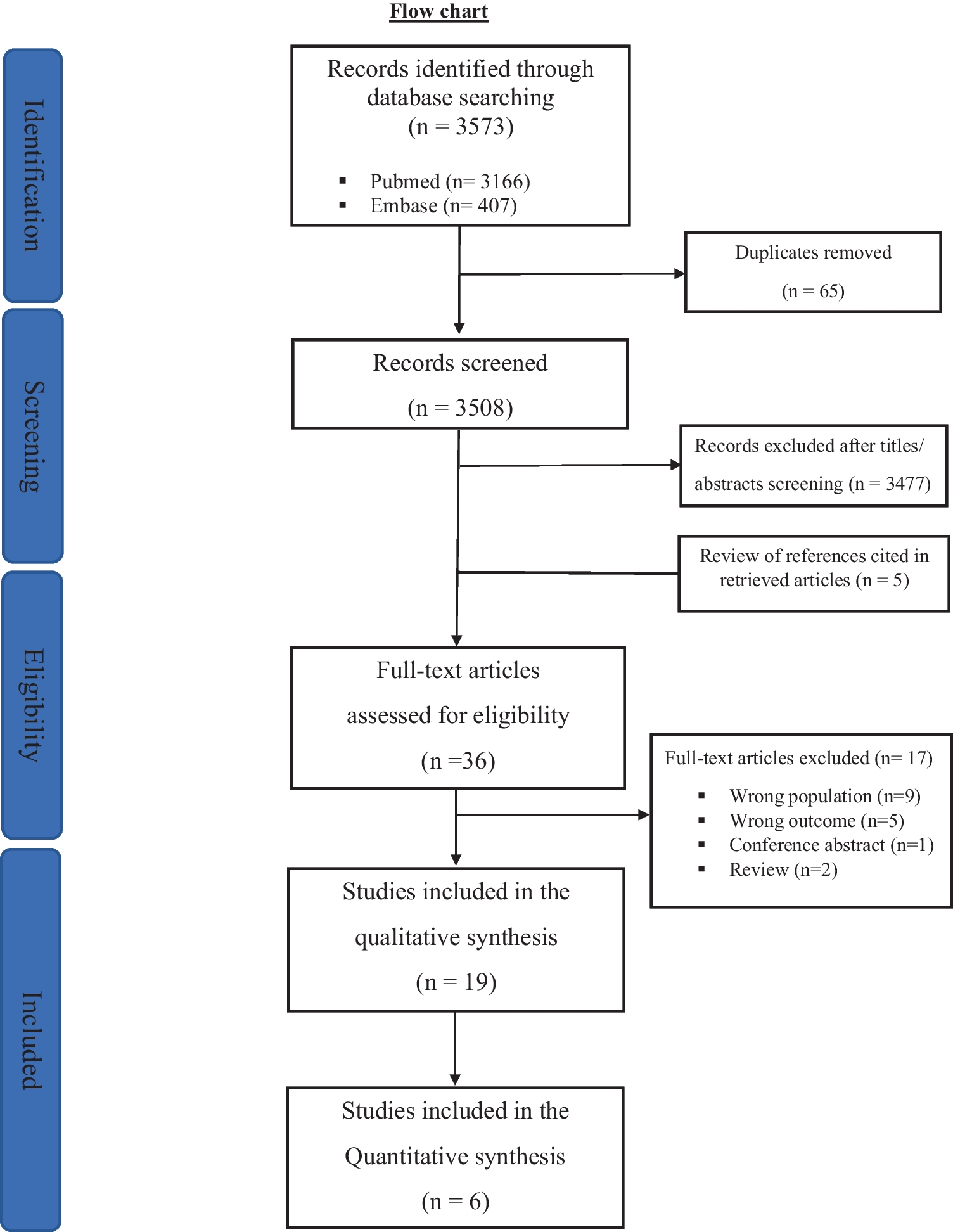
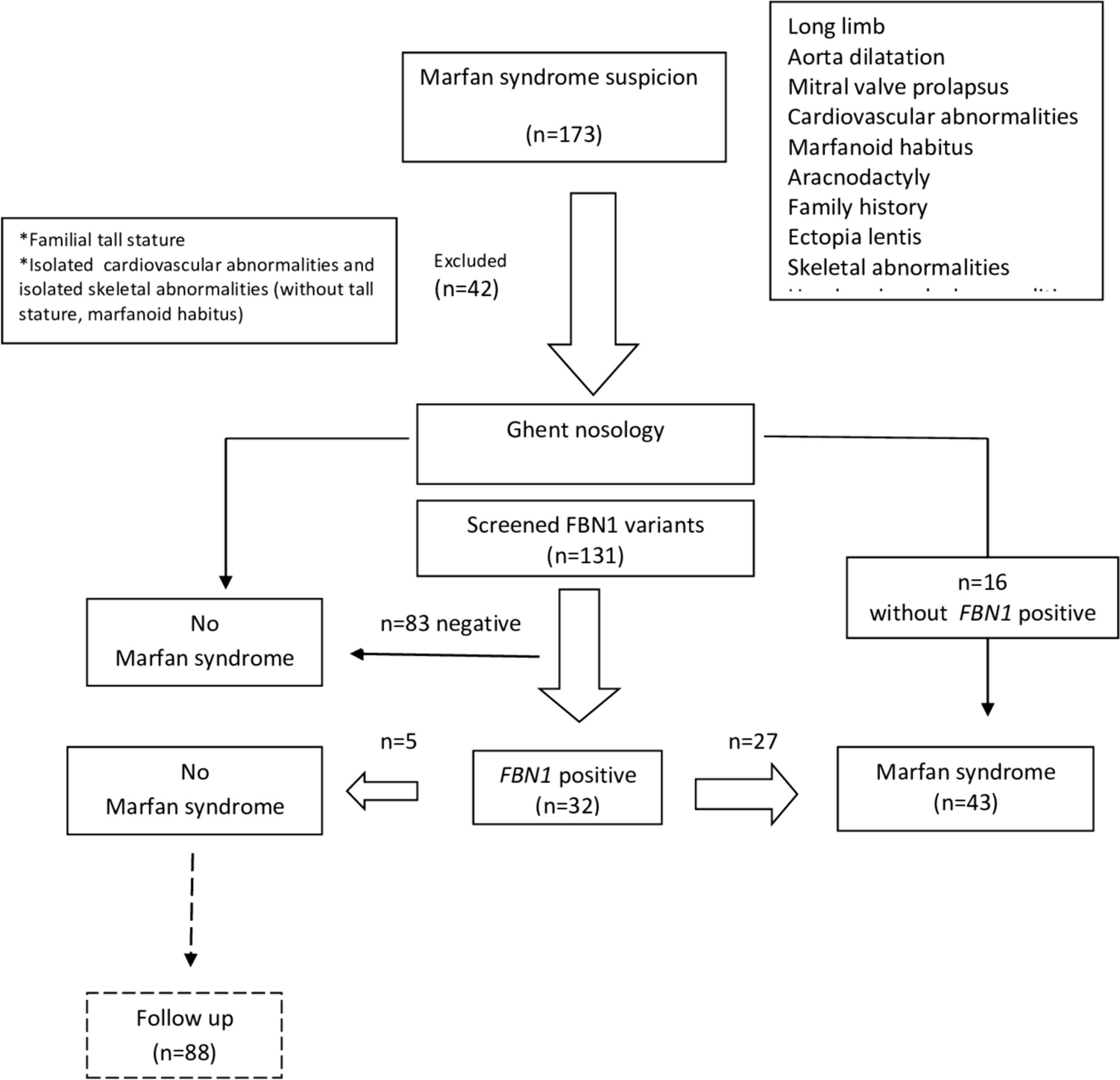
One hundred seventy-three patients were referred from orthopedics, ophthalmology, cardiology, and pediatrics outpatient clinics with suspicion of MFS (Fig. 1). Clinical findings suggestive of MFS included tall stature (height > +2.5 SDS), family history, arachnodactyly, lens subluxation, and anomalies of the chest, face, and extremities. FBN1 screening was not performed in 42 patients with another specific diagnosis: familial tall stature (n = 34), isolated cardiovascular findings (n = 4), and skeletal system findings (n = 4). FBN1 screening was performed to 131 patients who presented with at least one MFS-related finding [18]. These findings included a family history, clinical signs, and symptoms suggestive of Marfan syndrome, such as a Marfanoid appearance (long limbs, long face, thumb sign, wrist sign), aortic dilatation, other specific cardiovascular findings, skeletal system abnormalities, or ectopia lentis. In addition, a total of 131 patients underwent FBN1 molecular analysis. FBN1 screening was conducted on children who could not be diagnosed with MFS according to the revised Ghent criteria but were strongly suspected of having MFS. These children were mostly those for whom specific findings were expected to develop with age. Additionally, FBN1 screening was scheduled for children whose height exceeded their midparental height. Several cases were referred from various departments (ophthalmology, orthopedics, cardiology, etc.) with an FBN1 analysis report. The researchers collected clinical signs, symptoms, and genotype characteristics. Out of the 43 patients diagnosed with MFS according to the Ghent nosology criteria, 16 were found to have the FBN1 variant. The diagnosis of MFS was excluded in 88 cases, with the FBN1 variant detected in 5 participants.
Fig. 1
Flow chart of the selection and diagnosis process for cases screened with suspicion of Marfan syndrome
To describe clinical signs and symptoms of Marfan syndrome, annotations were sourced from the Human Phenotype Ontology, a standardized dictionary of phenotypic abnormalities in human diseases. These annotations covered a range of phenotypic abnormalities including growth (disproportionate tall stature, slender build), head and neck (long and narrow face, dental crowding, high narrow palate, downslanted palpebral fissures, open bite), eye (ectopia lentis, lens subluxation, lens luxation, glaucoma, retinal detachment, hypoplasia of the iris, increased axial length of the globe, flat cornea visual impairment, myopia), cardiovascular (ascending tubular aorta aneurysm, ascending aortic dissection, arterial dissection, mitral valve prolapse, tricuspid regurgitation, mitral regurgitation, bicuspid aorta, congestive heart failure), skeletal system (pectus carinatum, pectus excavatum, arachnodactyly, joint hypermobility, scoliosis, protrusio acetabuli, abnormal zygomatic bone morphology, dolichocephaly, retrognathia, micrognathia, kyphosis, limited elbow movement, osteoporosis, mitral valve calcification), and nervous system (dural ectasia). Marfanoid habitus was defined as a set of clinical signs and symptoms, with the most common features being disproportionate tall stature, long arms and legs, arachnodactyly, and joint hypermobility.
The researchers gathered data on family history, cardiac and ocular findings, and skeletal findings. They also documented measurements of height, weight, and body mass index. Aortic diameter Z-scores were extracted from echocardiography records. Aortic diameters were calculated using an automated software created by Cantinotti et al. [19]. The program captured measurements such as aortic valve annulus (mm), sinus of Valsalva (mm), sino-tubular junction (mm), and ascending aorta (mm) from the echocardiography results. The revised Ghent nosology was utilized to categorize phenotypes [18]. Systemic findings were employed as diagnostic criteria for cases with a score of ≥ 7. Marfan syndrome (MFS) was diagnosed based on the outlined criteria in the Ghent nosology.
Molecular analysisThe NGS (next-generation sequencing) analysis method was utilized to analyze the FBN1 gene. Primers covering the specified exons of the gene were employed. DNA was extracted from blood samples collected in EDTA tubes. The DNA concentration was measured using a Qubit 3.0 device (ThermoScientific, USA) and adjusted to a final concentration of 2 nanograms per microliter. Initial PCR steps (library preparation) were conducted with the obtained DNA samples and primer pairs specifically designed for sequencing the FBN1 gene, not for complete panel sequencing. The library fragments acted as templates for synthesizing new DNA fragments. Following the library preparation phase, the manufacturer’s kit was utilized for the emulsion PCR steps, which were carried out on the Illumina MiSeq device (USA) according to their protocols. The digital recording of the introduction of nucleotides into the growing DNA helix took place. The sample mixtures were processed using the relevant kits on the Illumina MiSeq device and loaded onto the appropriate chips to initiate the sequencing stage.
Variant classificationFBN1 variants were identified as exon regions that exhibited a strong genotype-phenotype correlation based on previous data. Consequently, the exon regions were categorized into three groups: N-terminus (exon 1–21), middle region (exon 22–42), and C-terminus (exon 43–65). The relationship between genotypes in these regions and the manifestations in the patients was assessed.
The pathogenicity classification of variants was determined in accordance with the 2015 American College of Medical Genetics (ACMG) standards and guidelines [20]: Class 1 (benign), Class 2 (likely benign), Class 3 VUS (variant of unknown significance), Class 4 (likely pathogenic), and Class 5 (pathogenic). Specific guidelines for FBN1 were utilized to determine variant pathogenicity based on ACMG [21]. The pathogenicity of the variants was compared to the phenotypic abnormalities.
Bioinformatics analyses were conducted using various databases (Encode, ClinVar, OMIM, COSMIC, PubMed, HGMD, PGMD, Ensemble, Mutation Taster, Varsome). The variants’ domains were identified using Prosit (http://www.expasy.org/prosite/) and Smart (https://www.smartgene.com/). The MutationTaster analysis program was employed for in silico analysis.
The cases were clinically divided into two groups based on FBN1 positivity and cardiac findings: FBN1 positive and negative groups, and cardiac findings positive and negative groups.
StatisticsQuantitative variables were defined as mean ± standard deviation, while qualitative variables were expressed as percentages. Group comparisons were conducted using the chi-square (χ2) test, with the Fisher test used if the chi-square test was unsuccessful. The distribution was tested using the Kolmogorov-Smirnov test. The Student t test was used for normally distributed variables, and the Mann–Whitney U test was used for non-normally distributed variables. Statistical analyses were conducted using SPSS v21 (IBM Corporation, New York, USA).
留言 (0)