Design
The present study is a post hoc analysis of secondary outcome parameters of a prospective observational study performed at the Division of Neonatology, Department of Pediatrics and Adolescent Medicine, at the Medical University of Graz, Austria (EC number: 30–450 ex 17/18).
Written parental consent was obtained before birth for all neonates included in the prospective observational study. Demographics and antepartum medical history of neonates were collected from patient charts.
Inclusion and exclusion criteria
Preterm and term neonates delivered by caesarean section due to feasibility to get informed consent before birth were included in the prospective observational study and were eligible for the present post hoc analysis. Neonates with ECG monitoring, arterial blood pressure measurements, and electrical bioimpedance-based CO measurements at 10 and 15 min after birth were included for analyses.
Exclusion criteria were major congenital malformations and umbilical cord artery pH < 7.0.
Monitoring
All neonates were transferred to the resuscitation table immediately after birth and routine monitoring with pulse oximetry and ECG (Intelli Vue MP 30 Monitor, Philips, Amsterdam, The Netherlands) was initiated.
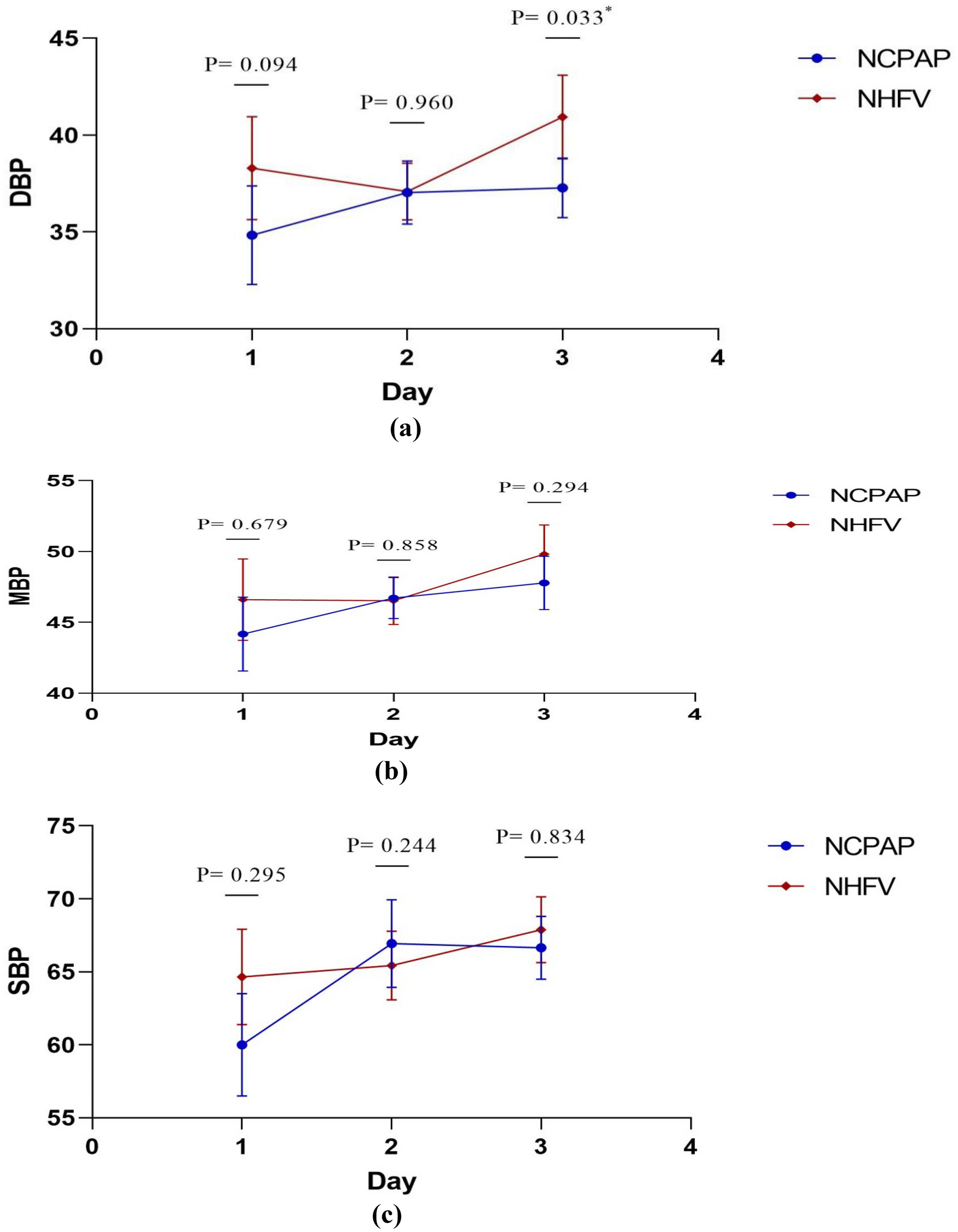
HR was continuously obtained by ECG during the first 15 min after birth. Arterial blood pressure was measured non-invasively at minutes 10 and 15 after birth using an oscillometric blood pressure cuff (Intelli Vue MP 30 Monitor, Philips, Amsterdam, The Netherlands) of appropriate size (#1, #2, or #3) on the right calf. The cuff size diameter was chosen according to the circumference of the infant’s right calf. The right calf was chosen to avoid interference with the pulse oximetry measurements at the infant’s right hand or wrist.
CO-bioimpedance measurement
For measurements of CO-bioimpedance, the Aesculon monitor (Osypka, Berlin, Germany) was used. Before starting the measurement, the skin was cleaned and four electrodes were placed on the left forehead, left side of the neck, left hemithorax, and left thigh. The CO measurements at minutes 10 and 15 after birth were only accepted if the Signal Quality Index (SQI) was ≥ 80%.
All data were continuously stored in a polygraphic system (alpha trace digital MM, BEST Medical Systems, Vienna, Austria) for further analyses.
COest/adj LaZ calculation
Estimated CO (COest) was calculated using the LaZ formula:
$$\mathrm=\mathrm/ (\mathrm+\mathrm) *\mathrm(\mathrm)$$
(PP: pulse pressure, SABP: systolic arterial blood pressure, DABP: diastolic arterial blood pressure, HR: heart rate).
CO was then adapted with the calibration factor (k) to gain the adjusted estimated CO (COest/adj LaZ).
$$}/\mathrm= k* (\mathrm/ (\mathrm+\mathrm) *}) (}:\mathrm/})$$
Statistical analysis
Demographic and clinical data are presented as mean ± standard deviation (SD) for normally distributed data or as median and interquartile range (IQR) for skewed distributions.
Correlation analysis of CO-bioimpedance and COest/adj LaZ was performed using Pearson’s correlation, due to this data being normally distributed. The Kolmogorov–Smirnov test was performed prior to establishing normality. In addition, the Bland–Altman analysis was performed.
A p-value < 0.05 was considered statistically significant. These values were considered in an explorative sense so that no multiple testing corrections were performed. All statistical analyses were performed using IBM SPSS Statistics 28 (IBM Corporation, Armonk, NY, USA).

留言 (0)