
記住我
The retina is a structure of the eye where characteristics of the microvasculature can noninvasively be viewed. Microaneurysms, hemorrhages, arteriolar-venular nicking, and arteriolar narrowing are findings in the retinal microcirculation in individuals with hypertension and diabetes [1]. Multiple studies suggest that these abnormalities of the retinal vasculature reflect pathology of the systemic microvasculature. This pathology, in turn, predicts cardiovascular morbidity and mortality [2–4]. We recently discovered that cerebral small vessel disease (SVD), particularly cerebral microbleeds (CMBs), is more common in young people with type 1 diabetes without any signs of neurological disease than in healthy controls [5]. In contrast, the differences between patients with type 1 diabetes and healthy controls in ischemic changes such as white matter hyperintensities and lacunar infarcts were not significant [5]. In the same cohort, cerebral SVD was associated with the severity of diabetic retinal disease (DRD), assessed with a validated clinical grading [6,7]. Importantly, the association was true only in those with either moderate or the most severe, sight-threatening form of DRD, proliferative diabetic retinopathy.
These findings raised a hypothesis about whether cerebral SVD is associated with other retinal changes measured as retinal vessel parameters (RVP) by Integrative Vessel Analysis (IVAN) (University of Wisconsin-Madison, Wisconsin, USA). This software uses digital retinal imaging technology to semi-automatically assess RVP. Through this method, quantification of vascular caliber is available, which can reveal both arteriolar narrowing and venular widening [8,9]. The retinal arteriole-to-venule ratio (AVR) has been shown to correlate with the risk of stroke and coronary artery disease [10]. Furthermore, the software has good internal agreement and reliability [9,11].
Our first aim was to assess whether RVP changes correlated with CMBs, which are the most common form of SVD in patients with type 1 diabetes. Second, we studied whether diabetes-related covariates, including glycemic control, blood pressure, and the presence of other diabetic microvascular complications, were associated with RVP. Third, we compared RVP between individuals with type 1 diabetes and healthy controls.
METHODSThis study is a part of the prospective nationwide Finnish Diabetic Nephropathy (FinnDiane) Study. The design of the FinnDiane study has been described elsewhere in more detail [12]. For this substudy, 191 subjects with type 1 diabetes were examined between 2011 and 2017 [5]. A total of 30 heathy age-matched and sex-matched controls were also enrolled. The participants were adults less than 50 years of age. None of the participants had a history or clinical manifestations of any neurological disease. However, one individuals who turned out to have experienced previous neurosurgery and two participants showing findings consistent with multiple sclerosis were excluded from the analysis. Exclusion criteria were kidney failure with replacement therapy, coronary heart disease or peripheral arterial disease, and contraindications for MRI. The study was carried out in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Helsinki and Uusimaa Hospital District (ID: HUS/2184/2017). Each participant gave their written informed consent prior to participation.
All participants underwent a clinical evaluation and comprehensive laboratory work-up at the FinnDiane research unit at Biomedicum Helsinki, Finland. The visit included a review of previous medical history, office blood pressure measurement and structured questions on lifestyle and anthropometrics. Blood pressure was measured twice with 2 min intervals in the sitting position after a 10 min rest, mean value of these two measurements was used as a continuous variable. Blood samples were drawn to analyze concentrations of plasma creatinine, lipids and lipoproteins [total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL) and triglycerides], high-sensitivity C-reactive protein (hs-CRP), and blood glycated hemoglobin (HbA1c) using standardized methods. Diabetic kidney disease was defined as increased albumin excretion rate (≥200 μg/min or ≥300 mg/24 h) in two out of three urine collections. Glomerular filtration rate (eGFR) was estimated by the CKD-EPI-formula [13,14].
The Early Treatment of Diabetic Retinopathy (ETDRS) scale was used to classify diabetic retinopathy severity [15]. Acquisition, evaluation and grading of retinal images has been described elsewhere [7]. Tropicamide was used for pupil dilatation [7]. For analysis, participants were categorized based on diabetic retinopathy severity: ETDRS score 35 or less indicated no-to-mild nonproliferative diabetic retinopathy (NPDR), 43–57 moderate to severe NPDR, and ETDRS score at least 61 proliferative diabetic retinopathy (PDR). Presence of any diabetic retinopathy was defined as ETDRS score at least 20 [7].
Carotid ultrasound was performed on the left and right carotid arteries. The distal 1 cm segment of the common carotid artery segment, immediately before the origin of the bulb was scanned using an ultrasound scanner equipped with a 10 MHz linear probe (MyLab 70, Esaote, Genova, Italy) and implemented with a radiofrequency-based tracking of arterial wall (QIMT) that allows an automatic and real-time determination of far-wall carotid intima–media thickness (CIMT). The mean of two measurements of the left and right CIMT was calculated for the subsequent analyses. To calculate central pulse wave velocity (cPWV), the path lengths from the sternal notch to the femoral pulse were measured.
Within 1 year of the clinical and laboratory work-up, all participants underwent a 3T brain MRI (Achieva, Philips, Best, The Netherlands) at the Medical Imaging Center at the Helsinki University Hospital. MR-sequences used were T1, T2, FLAIR, T1 MPRAGE, DWI, SWI, T2∗ and MRA TOF. Small-vessel disease (SVD) consisting of CMBs, white matter hyperintensities (Fazekas scale, with category ≥1 considered a significant burden), or lacunar infarcts were evaluated according to standardized criteria [16]. The number of CMBs were calculated and analyzed as a continuous variable. The MRI evaluation was performed by a senior neuro-radiologist (J.M.) with more than 10 years of experience, blinded to clinical and laboratory parameters.
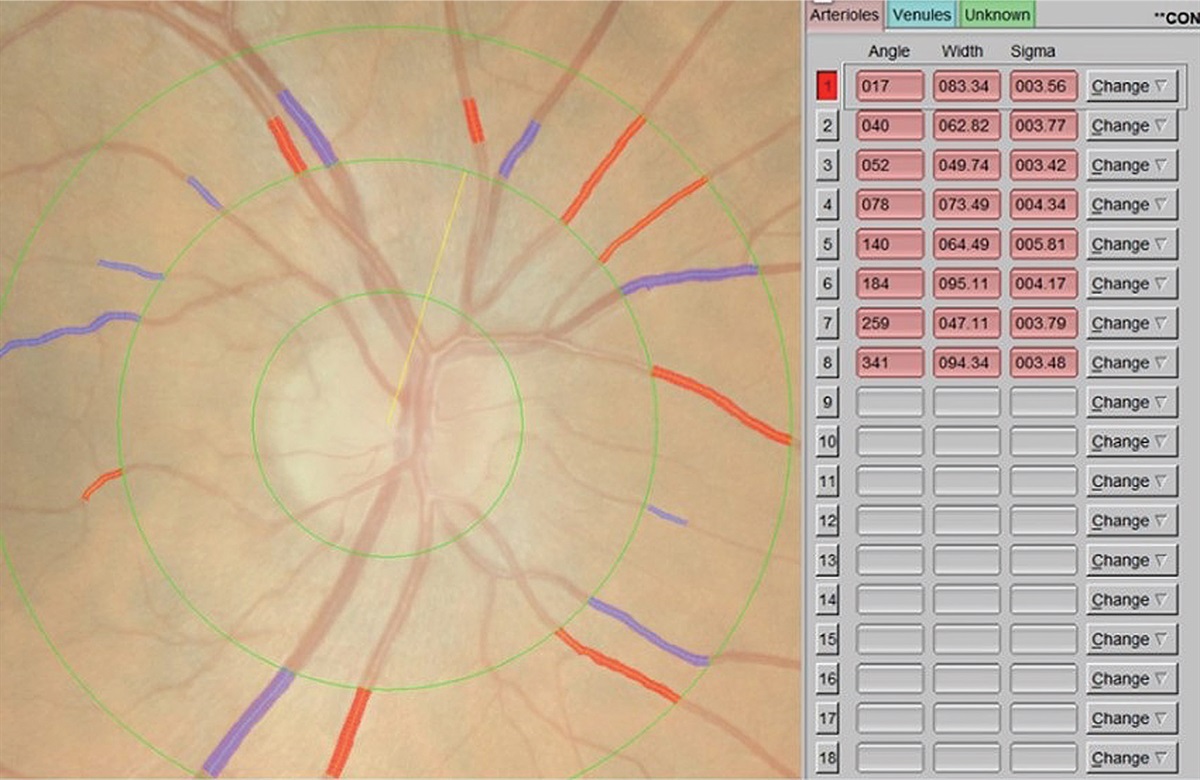
RVP indices were calculated using a computer-assisted semi-automated imaging software [Integrative Vessel Analysis (IVAN) software, version 3.2.6, University of Wisconsin, Madison, Wisconsin, USA] from digitized photographs. A standardized protocol at Centre for Eye Research Australia was followed [17]. The software identifies six largest arterioles and venules passing completely through a circumferential zone 0.5–1 disc diameter from the optic disc margin [18]. The software identifies the optic disc and measures the diameters of individual vessels. The grader confirms the correctness of vessel type selected by the program. Three indices are calculated by IVAN software, central retinal arteriole (CRAE) and central retinal vein (CRVE) equivalents and the ratio of the two variables (arteriovenous ratio, AVR), using the Knudtson's revision of the Parr–Hubbard formula [19]. CRAE was divided by CRVE to obtain the AVR. The grader (A.T.) was masked to subject identity and treatment. The right eye's image was primarily analyzed, unless unsuitable due to poor image quality leading to hazy or obscured views of the retinal vasculature (Fig. 1). In these cases of ungradable right eye images, the left eye's image was graded for RVP indices (Supplemental Data File, https://links.lww.com/HJH/C426).
 FIGURE 1:
FIGURE 1: Screenshot of Integrative Vessel Analysis software interface. Red vessels manually identified as arterioles and blue vessels as veins.
Statistical analysisThe normality of distribution of CRAE, CRVE, and AVR was evaluated using the Shapiro–Wilks test. Two-sided Student's t test was used to compare normally distributed variables between groups, whereas nonnormally distributed variables were analyzed with the Mann–Whitney U test. Data are presented as mean ± SD for normally distributed variables and median with interquartile range (IQR) for nonnormally distributed variables.
In individuals with diabetes, we analyzed the correlation between RVPs and clinical and laboratory variables using the Spearman's correlation test and linear regression analysis. Standardized coefficients were calculated to evaluate how many standard deviations RVPs would change per standard deviation increase in a specific clinical variable.
We also used binary logistic regression models to identify covariates that were independently associated with CMBs. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Along with RVP, HbA1c and SBP were included in the logistic regression analysis because of their associations with RVP. We conducted a sensitivity analysis by excluding individuals with at least moderate retinopathy (ETDRS >35) to assess the associations in a population of individuals with none-to-mild retinopathy.
Finally, we divided the subjects based on the median AVR into two groups: those with AVR more or less than the median value. We compared the clinical parameters of these groups using the Mann–Whitney U test and the prevalence of CMBs, WMHs, and lacunes using the chi-squared test.
Statistical analyses were performed using R (version 4.0.2). A two-sided P less than 0.05 was set as the threshold for statistical significance.
RESULTSRVP measurements were of sufficient quality in 77.7% (146/188) of individuals with type 1 diabetes and 80% (24/30) of the healthy control subjects. No significant differences in clinical characteristics were observed between individuals with type 1 diabetes who were included or excluded from the final analysis (P > 0.05 in all). There was no substantial difference in clinical characteristics between healthy controls who were included or excluded from the final analysis.
Of a total of 170 individuals included in whom RVPs were measured, 39% (57/146) of individuals with type 1 diabetes and 8.3% (2/24) of controls had cerebral SVD. Seventy percent of individuals with type 1 diabetes had no or mild diabetic retinopathy, 16% had moderate or severe retinopathy, and 14% had PDR. None of the controls showed signs of DRD.
In individuals with type 1 diabetes, diabetes duration was 21.7 (18.2–30.8) years and HbA1c 66 ± 13 mmol/mol. SBP was 129 ± 15 mmHg, total cholesterol 4.4 (4.0–5.0) mmol/l, LDL 2.37 (2.00–2.92) mmol/l, HDL 1.51 (1.25–1.80) mmol/l and hs-CRP 1.11 (0.50–2.31) mg/l. A total of 85 (58%) of subjects had either SBP over 130 mmHg or DBP over 80. Twenty-four-hour urinary albumin excretion rate was 13.7 (10.3–18.0) mg. Increased urinary albumin rate was present in 20 of 146 (13.7%) of subjects. In the T1D group, 34 (23%) were on statins, 55 (38%) on antihypertensive medication and 12 (8.2%) on low-dose aspirin. We lack granular details about the exact antihypertensive drugs; 30 subjects were on one type, 16 were on two types, 7 were on three, and 1 individual was on four different antihypertensive medications. The most frequently prescribed classes were angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, followed by calcium channel blockers, and then beta-receptor blockers. None of the age-matched and sex-matched controls had any of these medications. A total of 85 (58%) in the T1D group had either SBP greater than 130 mmHg or DBP greater than 80 mmHg (Table 1).
TABLE 1 - Participant characteristics People with type 1 diabetes (n = 146) Control subjects (n = 24) P Female sex [n (%)] 74 (51) 14 (58) 0.626 Age (years) 40.6 (33.7–45.6) 37.7 (31.1–41.1) 0.433 Diabetes duration (years) 21.7 (18.2–30.8) – – BMI (kg/m2) 26.9 ± 4.2 24.7 ± 3.3 0.002 SBP (mmHg) 131 ± 14 122 ± 11 0.002 DBP (mmHg) 77 (72–82) 76 (74–85) 0.384 HbA1c (%) (mmol/mol) 8.2 ± 1.2 (66 ± 13) 5.3 ± 0.2 (32 ± 2) <0.001 Creatinine (μmol/l) 68 (61–80) 74 (66–80) 0.305 Total cholesterol (mmol/l) 4.4 (4.0–5.0) 4.6 (4.2–5.4) 0.184 LDL cholesterol (mmol/l) 2.4 (2.0–2.9) 2.6 (2.4–3.3) 0.029 HDL cholesterol (mmol/l) 1.51 (1.25–1.80) 1.46 (1.28–1.62) 0.442 Triglycerides (mmol/l) 0.90 (0.71–1.43) 0.84 (0.71–1.25) 0.540 Statin therapy [n (%)] 34 (23) 0 (0) 0.002 Antihypertensive medication [n (%)] 55 (38) 0 (0) <0.001 Aspirin therapy [n (%)] 12 (8.2) 0 (0) 0.232 Albuminuria [n (%)] 20 (14) 0 (0) 0.055 Retinal photocoagulation [n (%)] 32 (22) 0 (0) 0.002 Coronary heart disease [n (%)] 1 (0.5) 0 (0) 1.000 Current smoking [n (%)] 11 (7.5) 4 (17) 0.118Clinical characteristics and MRI findings in participants with type 1 diabetes and control subjects matched for age and sex.HDL, high-density lipoprotein; LDL, low-density lipoprotein.
CRAE were normally distributed (P = 0.303 in Shapiro–Wilks's test), whereas CRVE and AVR were not (P < 0.001 and P = 0.036). There were no significant differences in CRAE between people with type 1 diabetes and healthy controls (Table 1).
Retinal vessel parameters in individuals with type 1 diabetesCRAE were not different between male and female individuals, but CRVE were larger among female individuals [277 (256–303) μm vs. 300 (272–325) μm, P < 0.001]. There was no difference in AVR between male and female individuals. None of the RVP were different in individuals with no-to-mild NPDR vs. those with more severe, similarly the RVP metrics were not different in individuals with moderate-to-severe DRD vs. PDR. CRAE were smaller in individuals with PDR vs. without PDR (P = 0.029), whereas CRVE or AVR were not different between eyes with vs. without PDR. CIMT was negatively associated with AVR (P = 0.034). None of the RVP indices were associated with diabetic kidney disease (P > 0.05). Similarly, no associations between lipids, cPWV, hs-CRP, antihypertensive or lipid-lowering medications and RVP were observed (P > 0.05 in all) (Table 2).
TABLE 2 - Relationship of various characteristics to central retinal arteriolar equivalent; central retinal venular equivalent, and arteriolar-to-venous ratio CRAE (μm) P CRVE (μm) P AVR P Male 165.15 (155.02–183.11) 0.100 285.00 (258.97–313.67) <0.001 0.61 (0.56–0.65) 0.789 Female 175.95 (155.85–196.39) NA 300.00 (272.51–325.54) NA 0.61 (0.54–0.66) NA Age <40 years 176.00 (156.64–195.74) 0.106 295.00 (266.49–317.64) 0.422 0.61 (0.55–0.66) 0.304 Age ≥40 years 164.87 (155.27–183.90) NA 290.42 (258.60–317.94) NA 0.60 (0.54–0.64) NA HbA1c <65 mmol/mol 171.87 (155.44–193.44) 0.673 287.28 (258.92–309.90) 0.105 0.64 (0.56–0.67) 0.035 HbA1c ≥65 mmol/mol 165.84 (271.26–320.00) NA 293.55 (155.75–191.70) NA 0.59 (0.54–0.63) NA BMI <25 kg/m2 171.97 (155.11–195.67) 0.721 292.81 (269.64–318.02) 0.264 0.61 (0.54–0.65) 0.596 BMI ≥25 kg/m2 167.40 (155.85–187.58) NA 287.10 (259.23–317.86) NA 0.60 (0.55–0.66) NA SBP <130 mmHg 172.96 (157.10–195.52) 0.180 295.74 (269.32–318.44) 0.099 0.61 (0.54–0.65) 0.977 SBP ≥130 mmHg 164.94 (154.50–184.94) NA 281.66 (258.57–316.76) NA 0.60 (0.55–0.65) NA DBP <85 mmHg 171.50 (155.67–194.56) 0.121 292.75 (261.04–318.45) 0.393 0.61 (0.54–0.66) 0.818 DBP ≥85 mmHg 161.01 (155.37–176.46) NA 278.80 (263.10–301.71) NA 0.59 (0.56–0.66) NA Heart rate <70/min 166.13 (155.11–193.29) 0.607 288.20 (260.76–319.59) 0.963 0.61 (0.53–0.67) 0.857 Heart rate ≥70/min 170.58 (156.87–187.61) NA 292.75 (263.37–316.80) NA 0.60 (0.55–0.65) NA Nonsmokera 169.24 (155.44–189.38 0.611 288.20 (260.78–318.14 0.082 0.61 (0.54–0.66) 0.226 Smokera 176.31 (156.80–198.00) NA 310.12 (292.70–315.74) NA 0.57 (0.54–0.61) NA None-to-mild NPDR 171.61 (159.82–191.11) 0.241 291.45 (261.30–314.67) 0.624 0.60 (0.55–0.66) 0.458 Moderate-severe NPDR 167.53 (157.47–201.69) NA 293.14 (273.95–332.87) NA 0.62 (0.567–0.656) NA PDR 157.54(149.43–173.26) 0.029 271.93(247.40–314.71) 0.331 0.58 (0.52–0.64) 0.226 No CMBs 171.10 (155.75–194.23) NA 290.95 (262.72–316.30) NA 0.61 (0.56–0.66) NA ≥1 CMB 163.68 (152.86–180.35) 0.159 292.98 (261.82–318.46) 0.577 0.58 (0.52–0.64) 0.023 Fazekas 0/3 171.50 (155.51–191.11) NA 291.98 (262.26–318.43) NA 0.61 (0.54–0.65) NA Fazekas ≥1/3 165.17 (155.85–189.28) 0.940 290.42 (269.62–301.39) 0.552 0.60 (0.58–0.66) 0.829 Lacunes absent 170.08 (155.44–192.20) NA 291.45 (262.99–318.22) NA 0.61 (0.54–0.66) NA Lacunes present 158.72 (157.28–160.88) 0.301 259.02 (253.15–276.85) 0.220 0.63 (0.58–0.64) 0.978 WMHs absent 171.97 (155.51–189.48) NA 293.14 (262.26–318.47) NA 0.61 (0.53–0.65) NA ≥1 WMH 164.33 (155.85–197.75) 0.946 288.20 (269.62–302.23) 0.545 0.61 (0.58–0.66) 0.426 Microalbuminuria 164.75 (155.76–176.79) NA 286.59 (258.24–327.30) NA 0.58 (0.54–0.63) NA No microalbuminuria 170.33 (155.51–192.74) 0.614 291.45 (262.94–316.54) 0.853 0.61 (0.55–0.66) 0.189 Antihypertensive drugs 164.87 (154.70–179.22) 0.128 280.04 (254.61–315.95) 0.273 0.59 (0.54–0.65) 0.278 No antihypertensive drugs 175.39 (156.35–195.35) 293.96 (266.33–317.94) 0.61(0.56–0.66) Lipid-lowering medication 164.00 0.250 293.91 0.915 0.58 0.097 No lipid-lowering medicationAVR, arteriolar-to-venous ratio; CMB, cerebral microbleed; CRAE, central retinal arteriolar equivalent; CRVE, central retinal venular equivalent; DR, diabetic retinopathy; PDR, proliferative diabetic retinopathy; WMH, white-matter hyperintensity.
aCurrent smoker/nonsmoker values given as median (interquartile range).
CRAE was associated with SBP but not with DBP. Neither CRVE nor AVR were associated with SBP or DBP. CRAE did not correlate with HbA1c. However, CRVE correlated positively with HbA1c and AVR negatively. None of the three variables correlated with the duration of diabetes (P > 0.05 for all) (Table 3).
TABLE 3 - Standardized coefficient values of linear regression for different characteristics CRAE, r P CRVE, r P AVR, r P Age (years) −0.154 0.063 0.024 0.776 −0.138 0.096 Duration (years) −0.050 0.554 0.075 0.377 −0.143 0.089 HbA1c (mmol/mol) −0.008 0.921 0.210 0.008 −0.213 0.007 BMI (kg/m2) −0.012 0.885 −0.015 0.856 0.026 0.752 SBP (mmHg) −0.185 0.025 −0.057 0.498 −0.094 0.261 DBP (mmHg) −0.107 0.215 0.017 0.840 −0.078 0.368 CMBs (n) −0.091 0.220 0.140 0.056 −0.063 0.035 WMHs (n) −0.015 0.846 −0.034 0.660 0.002 0.984 Lacunes (n) −0.076 0.368 −0.088 0.326 0.005 0.958 hs-CRP (mg/l) 0.148 0.087 0.031 0.720 0.090 0.298 Total cholesterol (mmol/l) −0.031 0.704 0.005 0.954 −0.030 0.710 LDL cholesterol (mmol/l) −0.022 0.781 −0.044 0.577 0.020 0.803 HDL cholesterol (mmol/l) 0.008 0.928 0.089 0.290 −0.064 0.451 Triglycerides (mmol/l) −0.059 0.464 −0.054 0.501 −0.018 0.822 eGFR (ml/min/1.73m2) 0.096 0.242 −0.094 0.252 0.187 0.022Linear regression coefficients values of univariate analysis and P for correlation between RVP and various characteristics. AVR, arteriolar-to-venous ratio; CMB, cerebral microbleed; CRAE, central retinal arteriolar equivalent; CRVE, central retinal venular equivalent; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; hs-CRP, high sensitivity C-reactive protein; LDL, low-density lipoprotein; RVP, retinal vessel Parameter; WMH, white matter hyperintensity.
There was no difference in CRAE or CRVE between subjects with or without CMBs. AVR were, however, lower among those with CMBs. There was no correlation between CRAE or CRVE and the number of CMBs, but AVR were associated with the number of CMBs. RVP indices were not associated with WMHs, Fazekas classification or lacunes (P > 0.05 for all) (Tables 2 and 3).
Finally, we divided individuals with T1D into different subsets between those with AVR below median value or above median value. Here we observed a difference in HbA1c and in CMB prevalence between these two groups, both values being higher in AVR below median group (Table 4 and Fig. 2). After further dividing DRD groups by median values of AVR, we observed a segregation in CMB prevalence (Fig. 3), and this difference was significant among both those with no-to-mild retinopathy and among those with ETDRS greater than 35.
TABLE 4 - Descriptive statistics AVR above median AVR below median P value Age (years) 40.06 (33.33–44.82) 40.75 (34.88–46.31) 0.136 Duration (years) 21.74 (18.34–27.27) 21.63 (17.96–32.15) 0.321 HbA1c (mmol/mol) 59.50 (56–70) 67.00 (60.0–75.5) 0.001
留言 (0)