
記住我
Tuberculosis (TB) remains a major health problem, especially in developing countries. A total of 1.6 million deaths due to TB were reported worldwide in 2021 and it was the second leading infectious killer after COVID-19. The WHO South-East Asia (SEA) Region is home to 26% of the world’s population with a 43% burden of TB. Six out of the global high TB burden countries are in the SEA Region: Bangladesh, the Democratic People’s Republic of Korea, India, Indonesia, Myanmar, and Thailand. Among extrapulmonary TB, tubercular lymphadenitis is the most prevalent.[1]
Fine-needle aspiration cytology is the first line of investigation for tubercular lymphadenitis as it is easy to perform, less invasive, quick, and economical. The typical cytopathological features of TB include epithelioid cell granulomas with Langhans giant cells and caseous necrosis. However, acid-fast bacilli (AFB) may not be always demonstrated on Ziehl-Neelsen stain on aspirate material. Furthermore, it is a time-consuming procedure with low sensitivity. More sensitive methods such as Lowenstein-Jensen culture and GeneXpert Mycobacterium tuberculosis/rifampicin assay may be required for confirmation where AFB are not demonstrated.[2]
GeneXpert is a sophisticated molecular diagnostic platform developed by Cepheid, a leading player in the field of molecular diagnostics. Utilizing real-time polymerase chain reaction (PCR) technology, GeneXpert enables rapid and precise detection of a diverse range of infectious diseases and genetic disorders. One of the distinctive features of GeneXpert is its automated and on-demand testing capability, delivering results swiftly without compromising accuracy. GeneXpert has garnered significant recognition for its pivotal role in the diagnosis of TB. The platform offers a rapid and reliable method for detecting M. tuberculosis, the causative agent of TB. This proves particularly invaluable in regions with a high prevalence of TB, where timely and accurate diagnosis is paramount for effective disease management. Beyond TB, GeneXpert has demonstrated its versatility in diagnosing other infectious diseases, including HIV, hepatitis, and respiratory infections. Its capacity to deliver quick and precise results has positioned it as an indispensable tool in the realm of molecular diagnostics, contributing to more efficient and targeted healthcare interventions.[2]
The present study aimed to evaluate the cytomorphological features of newly diagnosed cases of tubercular lymphadenitis confirmed by GeneXpert.
MATERIAL AND METHODSThis was a retrospective study in which all fine-needle aspirates from newly diagnosed cases of tubercular lymphadenitis confirmed by GeneXpert over a 1-year period from July 2022 to July 2023 were included in the study. Any previously diagnosed cases already taking ATT or patients with any history of malignancy (primary or metastatic) were excluded.
The May–Grunwald–Giemsa stained smears from these aspirates were categorized into three patterns:
Epithelioid cell granulomas with necrosis
Epithelioid cell granulomas without necrosis
Necrosis only
The cytomorphological pattern of granulomas was, further, classified into:
Well-composed epithelioid cell granuloma
Poorly formed epithelioid cell granuloma
Splintered epithelioid cell granuloma
Well-composed epithelioid cell granuloma was defined as epithelioid cells along with caseous necrosis, lymphocytes, and giant cells. Poorly formed granuloma was defined as a group of epithelioid cells along with caseous necrosis or lymphocytic infiltrate. Splintered epithelioid cell granulomas consisted of dispersed epithelioid cells with or without lymphocytic infiltration. The background of the aspirate which included a reactive lymphoid background, lymphocytes, eosinophils, and neutrophils was tabulated for all the cases.
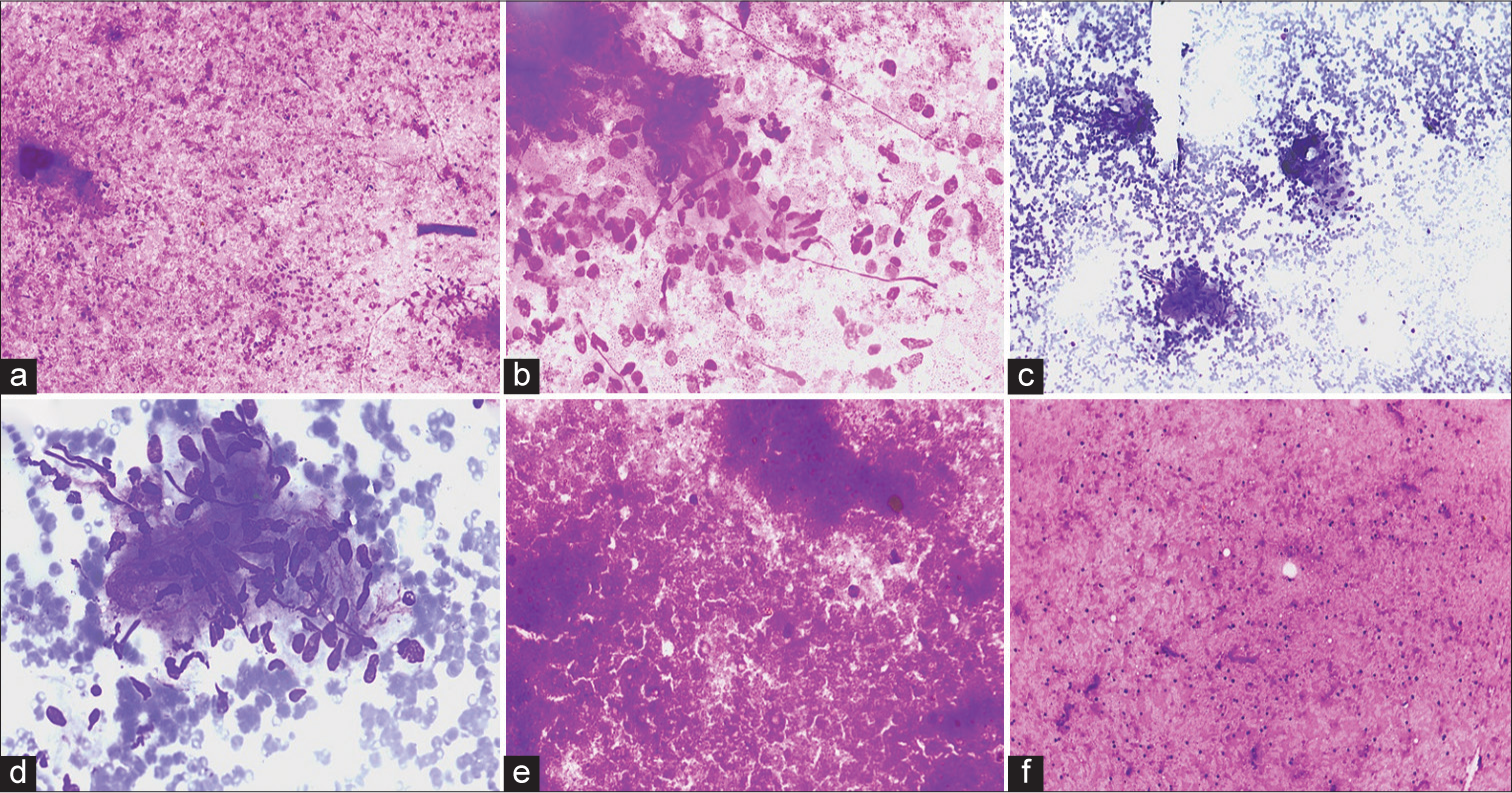
RESULTSA total of 120 lymph node aspirates from confirmed cases of tubercular lymphadenitis by GeneXpert were included in the study. The majority of the lymph node aspirates were from the cervical region (84, 70%), followed by axillary (18, 15%), inguinal (12, 10%), and supraclavicular (6, 5%). The age group of cases ranged from 6 years to 74 years with a male-to-female ratio of 1.2:1. Out of the three cytomorphological patterns, epithelioid granulomas with necrosis were the most predominant (67.5%), followed by necrosis only (20.8%) and granulomas without necrosis (11.6%) [Table 1, Figures 1 and 2].
Export to PPT

Export to PPT
Table 1: Categorization into different cytomorphological patterns along with AFB positivity.
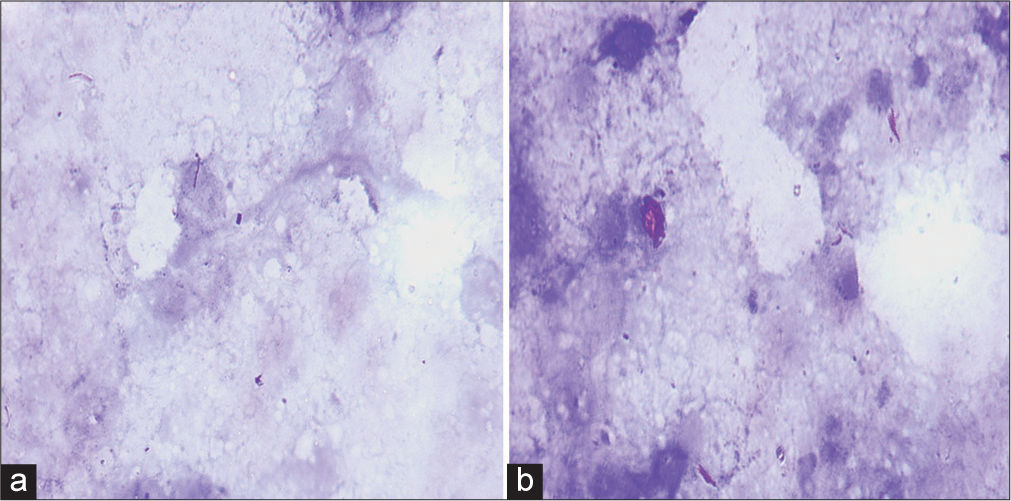
S. No. Cytomorphological pattern Total casesAn AFB positivity of 53.3% (64 cases) was seen on the Ziehl-Neelsen stain. Amongst these, the proportion of cases with AFB detected on the Ziehl-Neelsen stain was highest for necrosis only (60%) followed by the granulomas with necrosis pattern (54.3%) [Figure 3]. The location of AFB was predominantly extracellular (92%). The remaining cases (8%) exhibited AFB located intracellularly within the macrophages. The AFB were seen predominantly scattered singly (90%) except for very occasional cases (10%) where clumps of bacilli were observed.
Export to PPT
Well-composed, poorly formed, and splintered granulomas were seen in 55 (57.9%), 42 (44.2%), and 21 (22.1%) cases, respectively. [Table 2] Neutrophils were the most common background population (42, 35%) followed by lymphocytes (36, 30%). Reactive lymphoid cells and eosinophils were seen in 12 (10) and 3 (2.5%) cases, respectively [Table 3].
Table 2: Categorization of the different types of granulomas.
S. No. Type of granuloma (n=95) AbsentTable 3: Categorization of the background population.
S. No. Background (n=120) AbsentThe study illustrated that cases of tubercular lymphadenitis exhibit various patterns on cytopathological examination-granulomas with necrosis, granulomas without necrosis, and necrosis only. The most common pattern observed in the present study included epithelioid cell granulomas with caseous necrosis followed by necrosis only. This was concordant with the findings of most of the previous studies.[2-14] However, few authors found necrosis to be the most prevalent pattern.[15-18] The majority of the lymph node aspirates were from the cervical region (84, 70%), followed by axillary (18, 15%), inguinal (12, 10%), and supraclavicular (6, 5%). These findings were similar to those of previous studies.[2,4,6,10,11]
[Table 4] summarizes the different cytomorphological patterns in previously done studies. This difference could be attributed to the varying immune status of the cases.
Table 4: Percentage of each of the cytomorphological patterns in tubercular lymphadenitis reported by previous studies.
Author Number of cases Granuloma with necrosis (%) Granuloma without necrosis (%) Necrosis only (%) Helle et al.[2] (2023) 158 59 6 21 Shetty and Vyas[3] (2022) 100 59 22 14 Pooja et al.[4] (2020) 461 74.4 9.2 16.4 Rammeh et al.[5] (2018) 171 83.04 8.77 7.01 Hasija et al.[6] (2018) 271 45.75 39.11 15.12 Bhatta et al.[7] (2018) 126 53.17 38.09 8.73 Umar et al.[17] (2018) 612 30.4 16.7 78.3 Mitra et al.[14] (2017) 180 41 29 30 Gupta and Bhake[13] (2017) 69 49 26 25 Venkatraman[12] (2017) 132 55 17 28 Dasgupta et al.[18] (2017) 257 25 24 51 Masilamani et al.[9] (2015) 212 48 19 33 Hemalatha et al.[10] (2014) 150 56 19 23 Chand et al.[16] (2014) 550 22 28 50 Thakur et al.[11] (2013) 90 57.8 11.1 31.1 Mittal et al.[8] (2010) 36 47 17 36 Nayak et al.[15] (2004) 42 33 17 50An AFB positivity of 53.3% (64 cases) was seen on the ZiehlNeelsen stain which was highest for necrosis only (60%) followed by the granulomas with necrosis pattern (54.3%). The AFB were predominantly found extracellularly in the areas of necrosis. This is concordant to the study by Helle et al.[2,4,6,7,10,16,17] Cell--mediated immunity is responsible for mounting immune response against the tubercle bacteria in the form of a granulomatous reaction. Thus, cases with epithelioid granulomas without necrosis exhibit the least acid-fast bacilliAFB positivity. The cases with necrosis o nly exhibit the highest AFB positivity due to a lower cell-mediated immunity due to which they are unable to mount a granulomatous reaction.[7]
SUMMARYFine-needle aspiration cytology is a rapid inexpensive minimally invasive test for tubercular lymphadenitis as epithelioid cell granulomas along with caseous necrosis are highly suggestive of TB. However, manual AFB detection has a low sensitivity as is illustrated in the present study where only AFB was demonstrated in only 53.3% of cases. GeneXpert in addition to diagnosing TB can also test for Rifampicin resistance. Among confirmed cases of TB by GeneXpert, epithelioid cell granulomas with caseous necrosis followed by necrosis only are the most frequently observed cytomorphological patterns.
留言 (0)