In this post hoc analysis of older epilepsy patients with focal seizures, efficacy findings indicated a similar response to adjunctive cenobamate in older patients and the overall post hoc efficacy study population, with high rates of seizure reduction noted in both groups. Robust seizure reduction rates (e.g., ≥ 50% seizure reduction) in subanalyses of older patients have also been reported with other ASMs, such as brivaracetam [21, 22]. Specific considerations for ASM use in older patients with epilepsy include developmental changes associated with aging; increased polytherapy, including non-epilepsy drugs; and increased potential for drug–drug interactions and adverse medication effects [4].
Monitoring the effects of long-term ASMs on balance and the likelihood of falls, along with changes in cognition, are important for older patients [23]. During the 3-year treatment duration, older patients experienced a higher incidence of several TEAEs during long-term adjunctive cenobamate treatment compared with the overall safety study population, including dizziness (42.9%, 18/42), falls (29.3%, 12/42), and balance disorder (21.4%, 9/42). A subanalysis of perampanel in older patients (≥ 65 years of age, n = 20) with epilepsy from pooled, randomized, phase III studies also reported higher frequencies of adverse events, including dizziness and falls, during 19 weeks of treatment compared with adults 18–64 years of age [24]. The rates of dizziness and falls were 45% and 25% in the ≥ 65 years perampanel subgroup compared with 29% and 5% in the < 65 years perampanel subgroup, respectively. Falls are common in the older population and are of particular concern due to the prevalence of age-related decreases in bone density [2, 5]. According to a meta-analysis of 104 studies that included 1,741,613 people throughout the world, the prevalence of falls in older people was 26.5%. A systematic review of ASM use in older populations for any indication, not just epilepsy, noted an association between the use of any ASM and an increased risk of falls, with adjusted effect estimates ranging from a hazard ratio of 1.31 (i.e., a 31% increased risk) to an odds ratio of 2.8 (i.e., almost threefold increased odds) [25].
Older patients are also more likely to be taking a higher number of non-epilepsy medications, such as cardiovascular drugs, anticoagulants, antidiabetes drugs, etc., leading to a greater potential for drug–drug interactions that can increase the risk of dizziness. Considerations for starting cenobamate in older patients, like other ASMS, should include an assessment of comorbidities and all concomitant medications. In older patients with epilepsy, it is advisable to start an ASM with a low dose and titrate slowly to improve tolerability [7]. A lower maintenance dose of cenobamate should also be used if possible. Due to decreased creatinine clearance with age, particularly among women, an upper limit of cenobamate 200 mg/day should be considered in patients ≥ 65 years of age. Data from previous studies have shown that clearance of nearly all ASMs is reduced by approximately 20–50% on average in older patients in comparison with their younger counterparts, suggesting that doses should be up to 50% lower in older patients [7].
These recommendations are in line with our suggestions to start cenobamate at a low dose and slowly titrate to a low maintenance dose (200 mg/day). It may also be beneficial to assess fall risk in older patients before and during cenobamate treatment, as with other ASMs. These safety considerations should also be balanced with the risk of falls due to ongoing seizures.
The reduction of concomitant ASMs after the introduction of a new ASM, such as cenobamate, is an important goal to limit the number and severity of potential TEAEs [11, 12]. In this post hoc analysis, older patients had similar concomitant ASM drug load reductions compared with the overall study population after adding cenobamate. Previous data from the phase III study showed that concomitant ASM dose reductions frequently occurred following cenobamate initiation [12]. For instance, the dose of clobazam was reduced by 65.8% in patients who remained on cenobamate. Consensus recommendations for adding cenobamate to an ASM regimen include proactive dose adjustments of several concomitant ASMs that have pharmacokinetic or pharmacodynamic interactions with cenobamate, including phenytoin, phenobarbital, clobazam, and lacosamide [11]. Clinicians should consider a more aggressive, proactive reduction of concomitant ASM drug load reduction in older patients in order to reduce the risk of dizziness and falls in older patients.
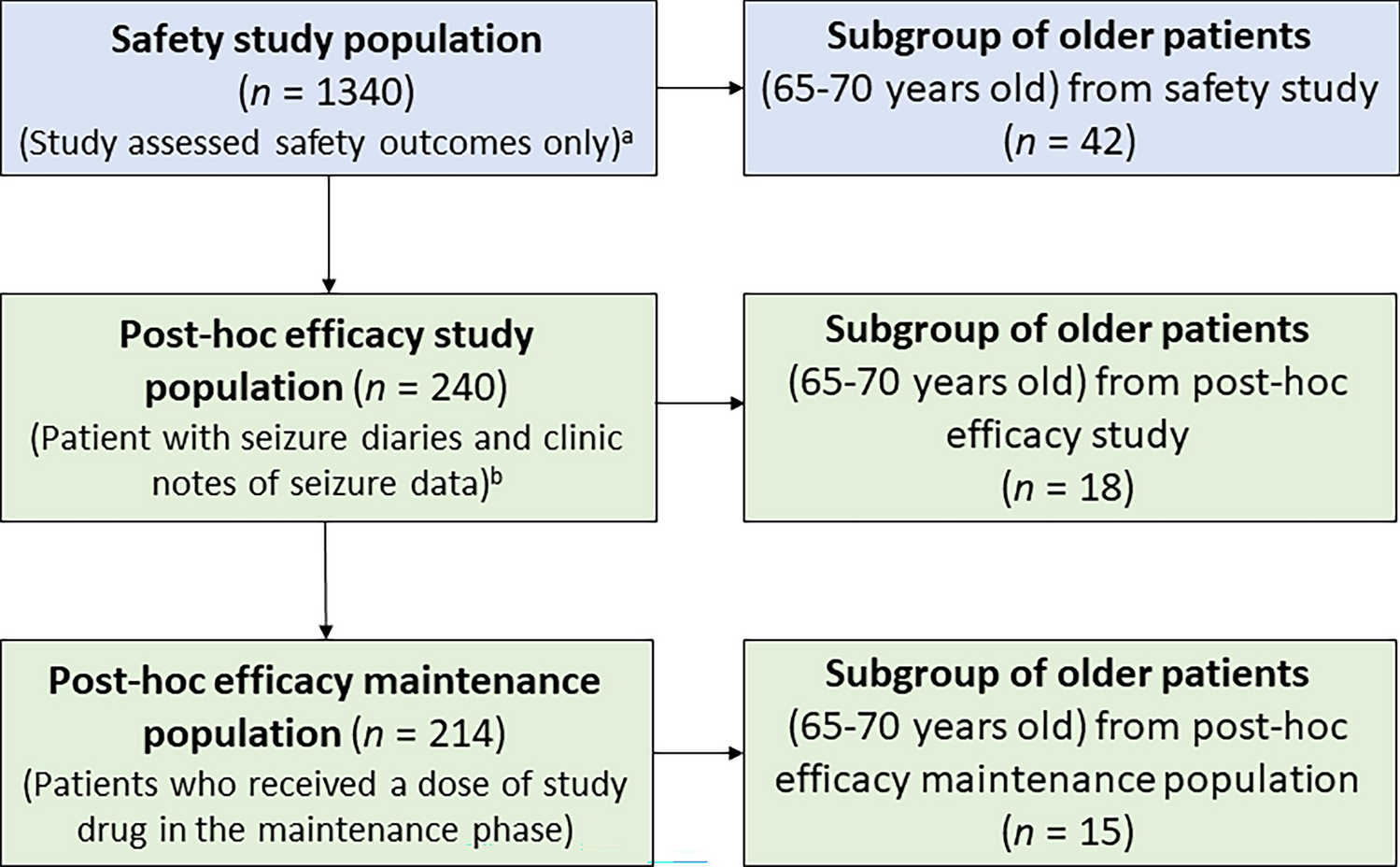
The strengths of this study include the relatively long study duration, allowing analysis of safety and efficacy up to 36 and 24 months, respectively. Responder rates, including 100% seizure reduction, were also reported across the entire maintenance phase, with a median duration of approximately 2.5 years. Limitations of the study include the small number of older patients in the safety (n = 42) and efficacy subgroups (n = 18). The post hoc, retrospective analysis is another limitation, and there is a possibility of selection bias associated with the open-label study design. Older adults are a heterogenous population and in a controlled study such as this, including strict inclusion/exclusion criteria, we may fail to observe certain challenges that have been found in real-world observations of older patients treated for epilepsy, such as lack of adherence to a treatment regimen or increased risk of dosing errors due to a decline in memory [23]. This may limit the generalizability of the study. The age cut-off for the study (70 years) also limits the generalizability somewhat, as there are many epilepsy patients >70 years of age who may face different sets of challenges. Additional analyses of ASMs such as cenobamate in a larger population of older patients, including age-stratified groups, severity and timing of adverse events, and their associations with specific concomitant ASMs, will help further inform clinicians. Furthermore, although the study design allowed for dose adjustments, which may be more reflective of real-world practice, cenobamate monotherapy was not allowed. While the older patients enrolled in this study had uncontrolled seizures despite treatment with one to three ASMs, many older patients, particularly those with newly diagnosed epilepsy, may be successfully managed with monotherapy. Future prospective research is needed to provide more guidance on the use of cenobamate in older patients, ideally following the suggestions for cenobamate dosing and dose adjustments of concomitant ASMs set out in this study.

留言 (0)