
記住我










Cardiac masses are uncommon, with an echocardiographic prevalence of 0.15%.[1] Historically, cardiac myxomas have been considered the most common benign cardiac tumor, usually occurring as a sporadic, solitary lesion on the left atrial side of the fossa ovalis (80%). Myxomas have also been reported to arise from the right atrium (RA) in 20% of cases. More rarely, the aorta, pulmonary artery, ventricles, and even the vena cava can be the site of origin.[2] Although benign, myxomas can cause varied symptoms due to hemodynamic impairment (valve obstruction, compression of vessels, and cardiac chambers), arrhythmias, and embolism requiring therapy, either medical or surgical.[3] The imaging appearance of thrombi and sessile myxomas may mimic each other.[4] Conversely, an atrial thrombus in some cases may have a stalk, misleading clinicians into diagnosing it as a myxoma. Differentiating between them can at times become a diagnostic challenge for the intraoperative echocardiographer, which is of paramount importance in tailoring treatment strategies.[5]
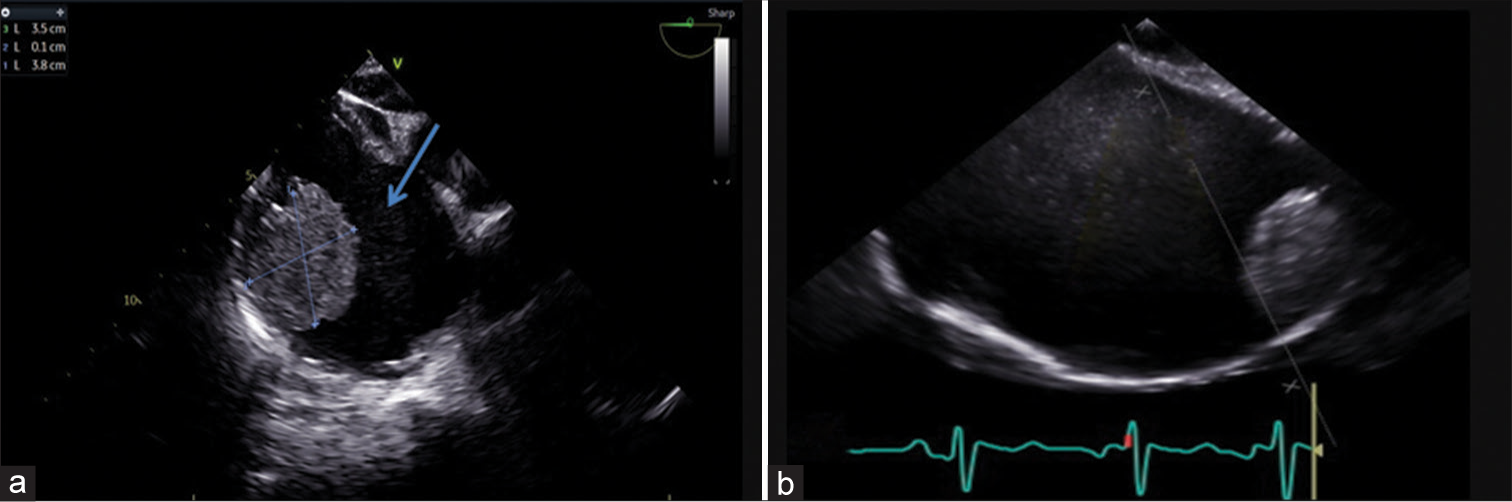
CASE DETAILSA 19-year-old male presented with gradually worsening dyspnea on exertion over 2 years with associated complaints of abdominal distension and pedal edema for 12 months. The patient also had a history of atrial fibrillation. Transthoracic echocardiography revealed a dilated RA with spontaneous echo contrast (SEC), dilated and severely dysfunctional right ventricle (RV), and a sessile solitary mass attached to the RA-free wall. Valvular pulmonary stenosis was also noted. Taking into consideration the clinical and echo findings, the mass was diagnosed as a thrombus. Low-molecular-weight heparin therapy was started, and the patient was planned for clot removal and pulmonary valvotomy. Intraoperative 2D transesophageal echocardiography (TEE) revealed a 3.5 cm × 3.8 cm echodense, homogeneous, ovoid-shaped, sessile, and immobile mass situated below the superior vena cava (SVC) on the RA free wall, suggestive of a thrombus [Figure 1]. 3D echocardiography (3DE) confirmed it to be a solitary, sessile mass; however, the 3D volume data set analysis showed that the mass had a heterogeneous, granular surface texture [Figure 2], few irregular calcifications in crop plane view, and random small areas of echolucency, suggestive of a tumor rather than a thrombus [Figure 3 and Video 1].[6] Surgically excised mass pointed toward it being a myxoma [Figure 4].
Export to PPT

Export to PPT

Export to PPT

Export to PPT
Video 1: Video showing loops from 3D transesophageal echocardiography view through various crop planes of the mass. DISCUSSIONPrimary cardiac tumors, cardiac metastases, vegetations, thrombi, fluid-filled lesions, and artifacts form the differential diagnosis for cardiac masses [Table 1].[6,7] Among them atrial myxomas show the most variability in shape and consistency. Right heart thrombi are often serpiginous, highly mobile, and associated with deep vein thrombosis and pulmonary embolism. Treatment with anticoagulants can help dissolve the thrombus, as was tried in our case.
Table 1: Echocardiographic features of cardiac tumors and mass.
Tumor/mass Characteristics Myxoma Usually smooth surface, mobile, pedunculated, heterogeneous, and minimal enhancement with contrast echo Papillary fibroelastoma Mobile pedunculated, homogenous, multiple fibrillar projections, small<1 cm, attached to valvular structures/cords Lipoma Smooth surface, increased echogenicity, minimal enhancement with echo contrast Rhabdomyoma Small, well-defined, solitary/multiple homogenous nodules or pedunculated mass, age <1 year Sarcoma Heterogeneous echogenicity, and hypoechogenic area may be suggestive of tumor necrosis Cardiac hemangioma Vascular channels with large echolucent areas, and high echogenicity with echo contrast Vegetations Irregular, lobulated, echo dense, chaotically mobile, can be multiple, attached to the upstream surface of valvular leaflets or mural endocardiumEchocardiography is the first line of diagnostic tool for the evaluation of intra-cardiac tumors.[8] TEE with better resolution becomes the imaging modality of choice for posteriorly located lesions, in perioperative assessment and guidance for surgical removal. The RA mass in our patient was not suspicious of myxoma, given the absence of stalk, location in RA, attachment site on the RA free wall, immobility along with dilated RA, RV, history of atrial fibrillation, and SEC or “smoke-like” echo, indicating a predisposing stasis, which almost always accompanies a thrombus on 2D echo. Table 2 gives the differentiating features between tumor (myxoma) and thrombi. Although cardiac magnetic resonance imaging (MRI) could have been performed for better tissue characterization of the RA mass,[9] in addition to it being expensive, it is not a part of routine investigation at our institute.
Table 2: Differentiation between thrombus versus myxoma.
Characteristics Thrombus Tumor (Myxoma) Area of origin LAA or LA (Rarely other chambers) LA, fossa ovalis3DE can delineate structural details difficult to image with 2D [Table 3].[10,11] 3DE refined the diagnosis as a myxoma in a case of cardiac mass by visualization of the peduncle.[12] A 13-patient study concluded, that 3D TEE is a valuable tool in morphologic imaging, bridges the gap between 2D and anatomy, useful in making decisions and surgical interventions.[13] 3DE was superior even to MRI in confirming a myxoma by identifying the stalk and attachment at the base of the interatrial septum close to the origin of the right inferior pulmonary vein.[14] 3D with its ability to acquire a pyramidal volume of 2D image,[15] which can be rotated and multi-planar cropping[16] capabilities to focus on the region of interest assists in identifying atypical masses allowing better tumor characterization, spatial relations, attachment, differential diagnosis, surgical planning, rationalized use of hospital resources, and eventual patient outcome.
Table 3: Advantages of 3D echocardiography over 2D.
Characteristics 3D 2D Localization +++ + Attachment ++ + Atypical anatomical features +++ + En-face view +++ _ Dropout artifacts for thin structures _ ++ Spatial relationship +++ ++ Mobility +++ + Multiplane cropping +++ _Intraoperative caution should have been exercised had the mass been a thrombus – during central venous catheterization, bicaval venous cannulation site since the mass was near the SVC-RA junction, to avoid inadvertent dislodgement and iatrogenic pulmonary embolism, which could have increased the cardiopulmonary bypass (CPB) duration and difficult weaning from CPB in a pre-operative dysfunctional RV.
CONCLUSIONAn intracardiac mass should be evaluated taking into consideration the clinical setting, age of the patient, tumor location, and echocardiography findings. 3D TEE gives us greater imaging quality and additional information, improving the sensitivity and specificity of diagnosis compared to 2D imaging.
留言 (0)