
Remember me








Participants included four Autistic children and adolescents. Charlie was a 16-year-old caucasian male who received approximately 10 hr per week of one-to-one behavioral intervention and had been receiving in-home applied behavior analytic intervention for approximately 6 years. English was his primary language, and he lived in an upper-middle-class neighborhood. Doug was a 9-year-old caucasian male who received approximately 6 hr per week of small group social skills training and had been receiving behavior analytic services for approximately 6 years. Of those years, he initially received 3 years of early intervention and subsequently 3 years of social skills training with one-to-one support. English was his primary language, and he lived in a middle-class neighborhood. James was an 8-year-old caucasian male who received approximately 20 hr per week of one-to-one behavioral intervention and had been receiving in-home applied behavior analytic intervention for approximately 1.5 years. English was his primary language, and he lived in a lower-middle-class neighborhood. Chris was a 9-year-old Latinx male who received approximately 2 hr per week of small group social skills training and had been receiving applied behavior analytic intervention for approximately 7 years. Of the 7 years, approximately 4 were in early intervention, and the remaining 3 were in social skills training. English was his primary language, and he lived in a middle-class neighborhood.
All participants had well-developed language skills, which included echoics, mands, tacts, and intraverbals. They spoke in complete sentences and engaged in back-and-forth conversation. They followed rules and exhibited a generalized imitation repertoire. In addition, all participants had mastered identification of what others are sensing (i.e., accurate identification of what others could see, hear, smell, taste, and feel when asked, “What do / does [person / pronoun] [see/hear/smell/taste/feel]?”; e.g., “What does mom smell?” “Popcorn!”; Welsh et al., 2019) and cause and effect (i.e., identification of potential causes when asked about visually apparent effects on stimuli in the environment, “Why [explanation of the effect]?” “Because [explanation of the cause]”; e.g., “Why is the glass frame broken?” “Because it was knocked off the shelf”; as well as identified and predicted potential effects of what might have happened when given an explanation of the cause,“What happened / will happen when / if [explanation of cause]?; e.g., “What will happen if I stick this pin in the balloon?” “It will pop!”). Moreover, predicting emotional causes (i.e., “What would make [person / pronoun] feel [emotion] in [situation]?”; e.g., “What would make your older brother so angry that playing the trick would no longer be fun?”) and effects (e.g., “How would [person / pronoun] feel if [situation]?”; e.g., “How would your grandmother feel if you played a trick on her that included you or someone else being very hurt?”) were prerequisite skill repertoires for discriminating “mean” versus “nice” tricks.
To be included in the current study, participants’ parents, clinical supervisors, and clinical team needed to regard playing tricks as clinically relevant and as an important and necessary target skill for each participant’s overall treatment and development. Playing friendly tricks was considered a clinically relevant skill to target when potential participants had a history of attempting to perform such tricks on others, but failing to do so successfully because they were missing a required component of trick-playing behavior. For example, a participant might giggle and smile uncontrollably while playing a trick or might not have been aware that most of their body was visible while trying to hide from someone.
All participants included were also required to have an active motivating operation for successfully playing tricks on others, as evidenced by either their direct report or observation of repeated, but ineffective, demonstrated efforts. In this way, each participant presented with a desire to play a trick on others, but did not effectively do so. That is, in addition to parents and clinicians stating that playing tricks was an important target of intervention to them, the participants themselves indicated that they wanted to play tricks on others. None of the participants had ever received previous direct training on how to use deception to play tricks on others, and throughout the course of the study, playing tricks was not targeted outside of the study by anyone.
All sessions were conducted within the context of normally scheduled, ongoing behavioral intervention or social skills training sessions, either in the participant’s home or in a clinic. Only one session was conducted daily, with one to four weekly, ranging in duration from 1 to 2 hr. Each session, three to seven trick trials were conducted and each trial was approximately 10 min in duration.
Response Measurement and Interobserver AgreementPlaying a trick was defined as any instance in which the participant independently completed each of the following components of trick-playing behavior: (1) stating; (2) executing; (3) inhibiting; and (4) ending the trick.
In order for stating responses to be scored as correct, the participant had to describe the trick to be played and initiate an explanation of the deception component (within 5 s of being asked) by discussing how they were going to do something or what they were going to tell someone that was not actually true, but would make the person think was true (e.g., “Let’s play a trick on Mom where I hide her cell phone and then ask her to use it to play a game. Mom will think it is where she last left it and will look for it there, but really it will be where we hid it!”). During phase 1 of training, if the participant engaged in no response, did not describe a trick to be played, and/or did not explain the deception component appropriately, the stating response was scored as incorrect. In addition to these response requirements, during phase 2 of training, if the participant did not describe a novel trick to be played and/or described a previously generated trick to be played with the same person it was already executed on, the stating response was scored as incorrect.
Executing responses were considered independent from stating. Within 1 min of stating the trick, participants were expected to begin executing that trick for a duration of no longer than 10 min. In particular, if the participant successfully carried out the trick they described (e.g., placing oneself in a closet in preparation for “popping out” at a family member passing by), within 1 min of stating it and for no longer than 10 min, and the individual the trick was being played on reported truly being tricked (e.g., because they had no idea the participant was in the closet and were completely startled), it was scored as a correct execution response.
In order for inhibiting responses to be scored as correct, the participant had to suppress any vocalizations, intonation, facial expressions, gestures, and/or body language that would “give away” the trick to the person it was being played on until that person reacted to the trick. In other words, each participant was required to engage in inhibition for the duration of the trick, and the criterion for a correct response required that the other person was, in fact, actually tricked. If the participant laughed; smiled; engaged in nervous or excited fidgeting; discussed the trick too much, too loudly, in too close of proximity to the person to be tricked; and/or gave away the trick in any other individualized manner evident to and reported by the individual being tricked, inhibition was scored as incorrect. Inhibiting responses were considered independent from executing, in that execution instructions involved telling the participant what to do, whereas inhibition instructions involved telling the participant what not to do.
After each trick, the person who was being tricked was interviewed to determine whether the trick was implemented effectively with successful inhibition of any responses that might alert them to the fact that they were being tricked. The self-report of individuals being tricked was required, because participants would, at times, engage in individualized, discrete behavior that gave away their trick to those who knew them really well, but would have been too subtle or personalized for the experimenter to readily detect. Therefore, such individualized feedback to the participant was valuable in training participants in their own independent execution and inhibition repertoires. As such, all individuals tricked in this study were instructed to respond naturally to participants respective to whether they were really being tricked (e.g., laughter, sigh of relief) or not (e.g., confusion, stating they know it is a trick). Subsequent to the participants' trick attempt, these persons were formally asked, “Were you really tricked, or were you on to [participant]?” If the person stated that they knew they were being tricked, they were asked to describe what the participant did that gave the trick away. This cued the experimenter to any highly discrete, personal participant responses that represented an execution error from the direct perspective of the individual being tricked and their relation to the participant, as well as assisted the experimenter in customizing the specific corrective feedback to be provided to the participant. For example, if a participant was playing a “made you look” trick on their nanny using a snake prop, but the nanny indicated that the participant’s body language and facial expressions were calm and casual with a flat intonation in their speech, corrective feedback would entail evoking contextually congruent nervous body language, fearful facial expressions, and distressed intonation to help “convince” the other person that they were being truthful, when in fact they were playing a trick.
Finally, an ending response was considered correct if it met two criteria. First, a response was scored as correct if the participant made a common ending statement (e.g., “Tricked you!” or “Gotcha!”) to the person within 5 s of seeing them react to the trick. Second, the participant had to explain the deception involved to the experimenter within 5 s of being asked by the experimenter (e.g, “[Participant] tell me about the trick we just played.” “I made my sister think she left her homework at school, but really I just took it from her backpack and hid it!”). If the participant did not make an ending statement that matched the purpose of the trick and/or did not accurately explain the deception involved within the trick, the ending response was scored as incorrect.
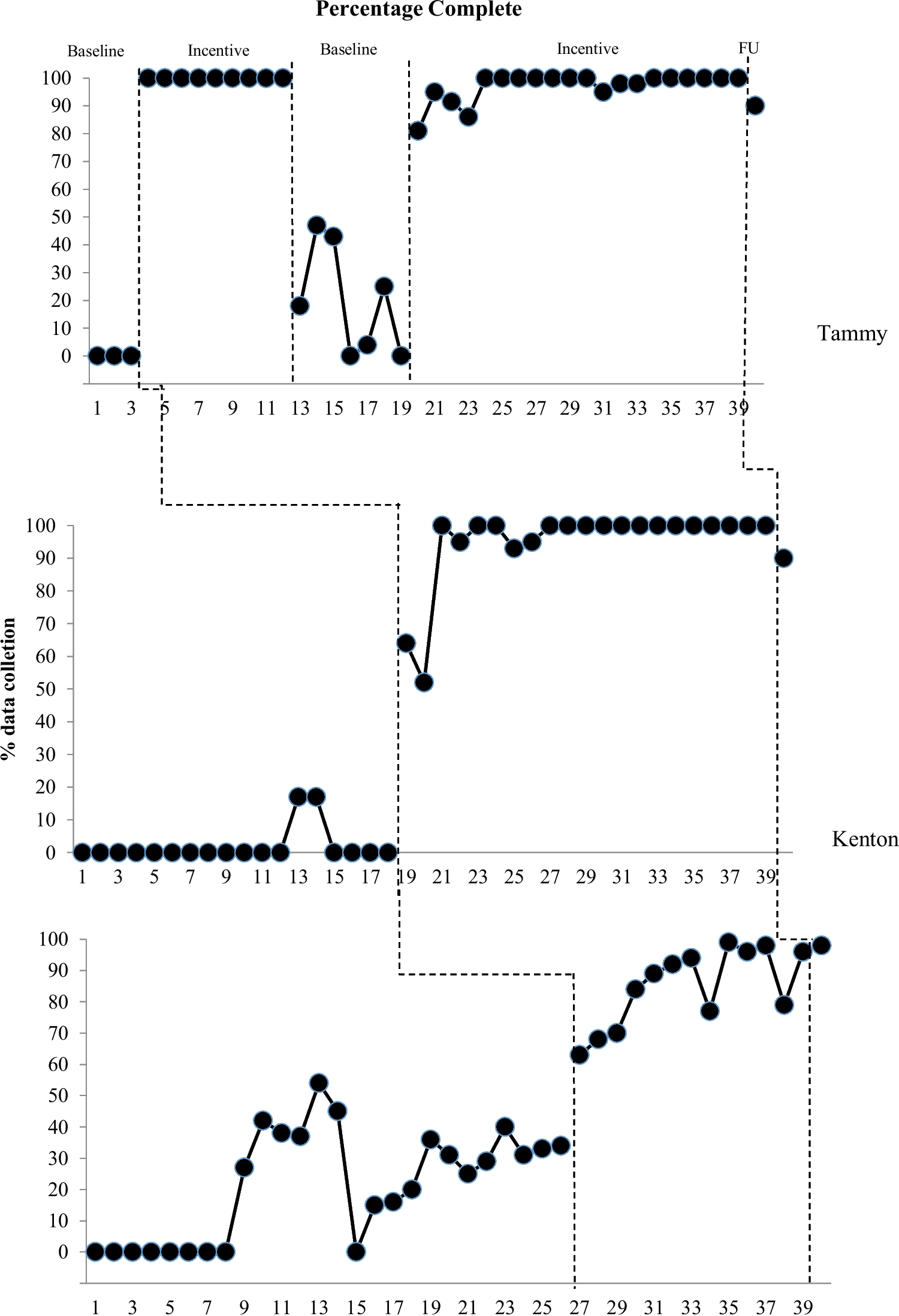
Data were collected on each of the four trick-playing behaviors within each trial. The percentage correct was calculated for each trial and then averaged across trials to calculate a total percentage correct for each session. Accuracy data on trick trials were summarized and graphed separately as percentage correct.
A second independent observer simultaneously collected data on 47%, 50%, 38%, and 43.75% of all sessions for Charlie, Doug, James, and Chris, respectively. Interobserver agreement scores were determined for each session by calculating the sum of agreements on the occurrence or nonoccurrence of correct trick-playing behaviors and dividing the number of agreements by the sum of agreements and disagreements and multiplying by 100%. Agreement averaged 99%, 100%, 98%, and 95.90% for Charlie, Doug, James, and Chris, respectively.
Experimental Design and ProcedureA nonconcurrent multiple baseline across participants design was used to evaluate the efficacy of the training package. Sessions were designed to be indistinguishable from participants’ regularly scheduled in-home or clinic-based intervention sessions. Trick trials were conducted during play breaks from other intervention programs. Breaks were provided between each trick trial and were long enough to conduct one or two other skill acquisition programs within the participants' behavioral intervention programs.
BaselineDuring each baseline session, the experimenter instructed the participant to engage in playing a trick on someone (i.e., “Let’s play a trick on someone. Who should it be and what should we do?”). After the delivery of the trick instruction, each participant had 1 min to initiate a trick and 10 min to complete it. If 1 min elapsed and the participant had not initiated a trick by beginning to state the trick or by engaging in behaviors to play a trick, all four components of trick-playing behavior were scored as incorrect, and the participant was redirected to another activity before moving on to the next trick trial. If the participant initiated a trick, but 10 min elapsed before the participant completed the trick, the individual components of trick-playing behavior that were completed were scored as either correct or incorrect and any uncompleted components were scored as incorrect. No prompting was used in baseline and no programmed consequences were provided for any participant's responses to the instruction to engage in playing a trick. Throughout baseline, sessions were no longer than 1 hr in duration, wherein a total of three trick trials were conducted.
TrainingThroughout training, three to seven trick trials were conducted per session, and all sessions ranged in duration from 1 to 2 hr. During training trials, experimenters honored the participants’ choice to assent to the procedures or not. Escape extinction was not implemented and participants were not required to comply with training. In particular, if a participant indicated that they did not want to play a particular trick on someone, the experimenter asked the participant if they wanted to think of a different trick or if they wanted to think of a different person to play a trick on. If a participant vocally indicated that they did not want to play any tricks on anyone or nonvocally withdrew assent by engaging in any behavioral escalation, the training trial would have been terminated; however, this never occurred.
Phase 1: Rules, Discrimination Training, Modeling, and Contrived PracticePhase 1 of training included all of the following components presented sequentially in order for participants to learn the basics of successfully completing a trick: rules with example and nonexample, modeling, and contrived practice. This phase was carried out until an effect was apparent through visual inspection of data.
Rules and Discrimination TrainingAt the beginning of session 1, the participant was provided with the rule, “Sometimes people play tricks on one another for the purposes of teasing the other person and having fun. A trick is when someone says something or does something that is not really true, but tries to make another person think it is true, even though it isn’t.” Then, the participant was given a randomly ordered example and nonexample to assist with discriminating a trick from a nontrick (e.g., “For example, I would be tricking you if I told you that you had a big, ugly stain on your shirt, because you don’t, but if you did have a stain on your shirt it wouldn’t be a trick because it would be true.”). Immediately upon the provision of the example and nonexample, participants were asked follow-up questions to ensure attending and rule comprehension (e.g., “So, why would telling you that you have a big, ugly stain on your shirt be a trick?” “Because I don’t have one / Because it isn’t true!” and “Why would telling you that you have a big, ugly stain on your shirt not be a trick, if your shirt really was actually stained?” “Because I do have one / Because it is true!”). Correct follow-up answers resulted in praise. Incorrect follow-up answers resulted in error correction in the form of the provision of the correct interpretation (e.g., “Telling you that you have a big, ugly stain on your shirt would be a trick because you do not really have one!” and “Telling you that you have a big, ugly stain on your shirt if your shirt really was stained would not be a trick because then you would actually have a stain and it would be true!”). Additional novel and arbitrary examples and nonexamples continued to be discussed until the participant correctly discriminated between a trick versus a nontrick within one presented trick scenario.
After providing one correct, independent discrimination of a trick versus a nontrick, session 1 continued by instructing participants to differentiate between mean versus nice tricks using the rule, “Remember, playing tricks is for fun and to make people laugh! Tricks should not be played if they hurt someone’s feelings or if they cause something to break that cannot be fixed.” Next, the participant was required to identify a potentially mean trick (e.g., “Can you think of any mean tricks?”), as well as explain why it is considered mean (e.g., “Why would that trick be mean?”). When the participant accurately identified one trick that would be mean and explained why, they were told that they were correct and praised. If the participant did not accurately identify and explain a mean trick, the experimenter modeled an example (e.g., “For example, a trick would be mean if we really stained someone’s shirt, because we might not be able to fix it and that person’s shirt would be ruined!”). Then, the experimenter asked the participant to present their own example. This continued in a back-and-forth manner until the participant ended on a correctly generated example of a mean trick and explained why it was mean. The same procedure was used for identifying a nice trick. Once participants could identify and explain at least one novel mean and nice trick example, this phase of discrimination training with social rules was considered complete.
ModelingNext, a nice trick was modeled by the experimenter in order to demonstrate what an appropriate trick would look like when conducted with another person (see Table 1 for categories of tricks and examples of tricks in each category). At least one of each type of trick was modeled for each participant; however, there was no direct instruction given to participants about the different categories of tricks. First, stating was modeled (e.g., “Playing a trick on someone looks something like this: “[Participant] I’m going to tell [person] we broke a vase, even though we did not break a vase, because I know she would not like for her vase to be broken and she might freak out! [Person] will think we broke her vase, but really her vase will be fine and she will be so relieved when we show her!”) using inhibition (e.g., whispering or relocating if the person with whom the modeled trick was to be played was near). Second, executing was modeled according to the plan by addressing the person with whom the trick was to be played (e.g., “[Person] we broke your vase!”) in a panicked tone of voice, with tense body language, and a concerned facial expression. Third, inhibiting was modeled by clearly withholding any laughing, smiling, or talking about the trick in a way that could give away the trick. Fourth, ending the trick was modeled by letting the third person know that they were being tricked (e.g., “Gotcha!”) and subsequently explaining the deception just modeled (e.g., “We made [person] think we broke her vase, but really, her vase was not broken!”).
Table 1 Examples of Tricks in Each Category Contrived PracticeAfter one trick was modeled, contrived practice was conducted to afford participants opportunities to carry out a trick. During contrived practice, participants were expected to independently follow through with each of the four trick-playing behaviors using either previously learned tricks (e.g., those modeled) on the same person for continued practice, a previously learned trick with a novel person, or novel tricks that they thought of but had never played before. There were no requirements put in place regarding which categories (displayed in Table 1) of tricks the participants should carry out, as we wanted them to have the autonomy to choose the tricks they wanted to perform, based on their personal preference.
The participant was instructed to play a trick on someone who was physically present in the home or clinic but was not the experimenter (e.g., “Let’s play a trick on someone, who should it be and what should we do?”). After the delivery of each trick instruction, each participant had approximately 1 min to initiate the trick they stated and 10 min to complete the trick, just as in baseline. When participants responded correctly on all four components of a trick, they received descriptive verbal praise (e.g., “You did it! You played a very funny trick and [person] really believed [false statement for trick] even though it wasn’t true! Great job!”) and brief access to a preselected preferred item (5 min or less) or activity (10 min or less). Preferred items or activities were determined via an informal preference assessment, wherein participants were provided with choices of items or activities eligible for earning, from which they made their preferred selection.
For incorrect responses, error correction procedures were implemented. Error correction involved prompting the participant to identify the steps of the trick performed incorrectly and how to respond appropriately in later trials in a least-to-most intrusive presentation (i.e., experiential–leading question–role play–partial vocal directive–full vocal directive). In particular, experiential prompts permitted the participant to make mistakes during execution, while the experimenter prompted the person the trick was being played on to respond appropriately (e.g., by showing that they were not tricked). This afforded the opportunity for the participant to undergo the natural consequences of their misperformed trick. Leading question prompts included asking the participant questions such as, “What did you forget to do?” or “Why do you think [person] didn’t fall for the trick?” Role-play prompts involved practicing each trick-playing behavior aloud to identify if the participant could detect errors when reenacted. Partial vocal directive prompts included giving the participant a hint that they were missing a trick-playing step or implementing it inaccurately, for example, “You forgot something!” or “There is something you need to fix to make the trick happen.” Finally, full vocal directive prompts involved directly explaining to the participant which trick-playing step(s) was performed incorrectly and giving an explanation for why.
Phase 2: Rules, Contrived Practice, and METDuring phase 2 of training, discrimination training and modeling were discontinued and the remaining sessions of training included the following components presented simultaneously: rules, contrived practice, and MET. MET (Erhard et al., 2021) was conducted to establish the generalized behavior of creating and playing tricks across multiple exemplars. Within this teaching phase, participants were expected to differentially and independently follow through with each of the four trick-playing behaviors using only novel tricks the participant designed and had never played before or a previously learned trick with a novel person they had never played it on before. In this way, MET was implemented to promote the acquisition of a trick-playing repertoire, rather than rote, rigid, or repetitive acquisition of a particular trick or trick type.
The following instruction was provided to participants: “Let’s play a trick on someone that we have never played on them before, who should it be on and what should we do?” Unlike in phase 1, to be scored as correct, participants could no longer repeat any previously learned tricks with the same person during phase 2. In this manner, this phase took into consideration the trick-playing history of the participant with others and how this could affect successful deception. For example, if a participant repeatedly went up to the same person, pointed to any piece of their clothing (e.g., shirt the first time and pants the next), and said, “Oh no! What happened?” (i.e., suggesting a stain), eventually the person may respond, “Not this again!” in recognition that they are being tricked in the same way they already have been before. The same reinforcement and error correction procedures described in the contrived practice section of phase 1 of training were employed in phase 2. During phase 2, data were collected until participants’ responding was considered stable at or near 90%–100% correct upon visual inspection.
Social ValidityAt the conclusion of training, parents were asked to complete a seven-item survey to provide written feedback regarding the overall acceptability of the clinical procedures that were used to teach their child or adolescent to play friendly tricks on others and the total satisfaction with treatment outcomes. This measure was designed to assess potential positive and adverse effects the study may have had on participants. For six of the seven questions, parents were asked to provide a rating on the scale of 1 (strongly disagree), 2 (disagree), 3 (neutral), 4 (agree), or 5 (strongly agree). Question 1 stated, “I am happy with the procedures that my child’s clinical treatment team used to teach them how to play friendly tricks on others.” Question 2 stated, “My child enjoyed learning how to play friendly tricks on others.” Question 3 stated, “My child benefited from learning how to play friendly tricks on others.” Question 4 stated, “I think that the ability to play friendly tricks on others was important for my child to learn.” Question 5 stated, “I would recommend the playing tricks training program implemented by my child’s treatment team to other parents who have a child with autism.” Question 6 stated, “The playing tricks training program did not have any negative side effects.” The final question was open-ended and stated, “Is there any additional feedback you would like to add regarding your child’s participation in the playing tricks training program?”
Comments (0)