
記住我

Cleansing wounds with antiseptics is an important treatment to control and eradicate bacterial wound contamination.1–3 However, improvements in care can be achieved if other effective methods are combined with antimicrobial treatments. Combining other methods such as low-pressure jet lavage wound irrigation with a standard FDA-approved antimicrobial could improve treatment efficacy and patient outcomes.
CASE REPORTThis report describes an institutional review board-sponsored intention-to-treat protocol (Sterling IRB #6066, Atlanta, Georgia) investigating jet lavage wound irrigation using 3 L of jet lavage irrigation in the outpatient setting. The intention-to-treat model does not exclude participants for severe disease or unrelated medical considerations. As part of this protocol, this case patient signed a consent form that described the treatment in detail and careful measures to make all materials confidential. This consent included eventual publication of all clinical details.
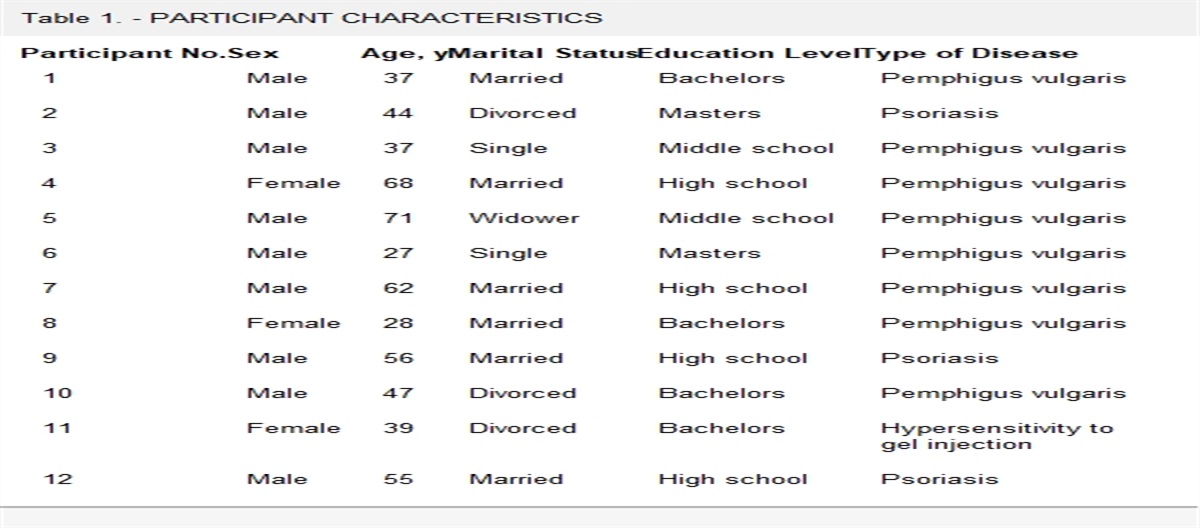
The patient was a 73-year-old man with obesity who had become bedridden 8 years prior as a result of a neurologic event and had developed a recalcitrant pelvic pressure injury (PI). The patient’s Charlson comorbidity score was 8 (scores over 5 are considered high risk); his Braden Scale score was 15 (mild risk); and he had aortic stenosis, atrial fibrillation, and chronic stroke disease.
This patient had a very large, 260 cm2 stage 4 pelvic PI over his sacrum, left greater trochanter, and left ischium (Figure 1). This longstanding chronic wound had been present for over 8 years and surgically debrided in the OR 18 times. Negative-pressure wound therapy had been used on multiple occasions but was not successful. He was referred to a university hospital trauma team who debrided the wounds on four occasions to remove debris and attempt to stabilize the wound from chronic infection. He then was referred to the author’s long-term care facility where he remained for the next 27 months. He was classified as palliative care because the surgeons determined he was not a candidate for plastic surgery reconstructive procedures.
 Figure 1.:
Figure 1.: SEVERE STAGE 4 PELVIC PRESSURE INJURYA 73-year-old man with 260 cm2, stage 4 pelvic pressure injury for 8 years involving the sacrum, left ischium, and left greater trochanter.
Autofluorescent ImagingAutofluorescent imaging (AFI) with a digital device (MolecuLight; MolecuLight Inc.) is used to assess local bacterial contamination. This validated method has become the standard for assessing local wound treatments in the author’s facility.4–8
The AFI tool used in the present report uses an iPhone system with a 405-nm-wavelength UV light to illuminate porphyrins “bright red” (the heme pathway commonly is produced by 80% of bacteria).7 Destruction of the bacteria causes a dark or “black” autofluorescence image at log 2 colony-forming units (CFUs)/g of tissue. The positive predictive value for the log 4 bacterial level is 100%. The low-end sensitivity is at log 2 CFUs per gram of tissue (CFUs/g). Importantly, bacteria can be clearly identified, and the potential depth of penetration of the UV light is 1.5 mm.
For this patient, the author utilized AFI beginning July 1, 2020, extending for 20 months to April 12, 2022, with a total of 71 weekly AFI studies.
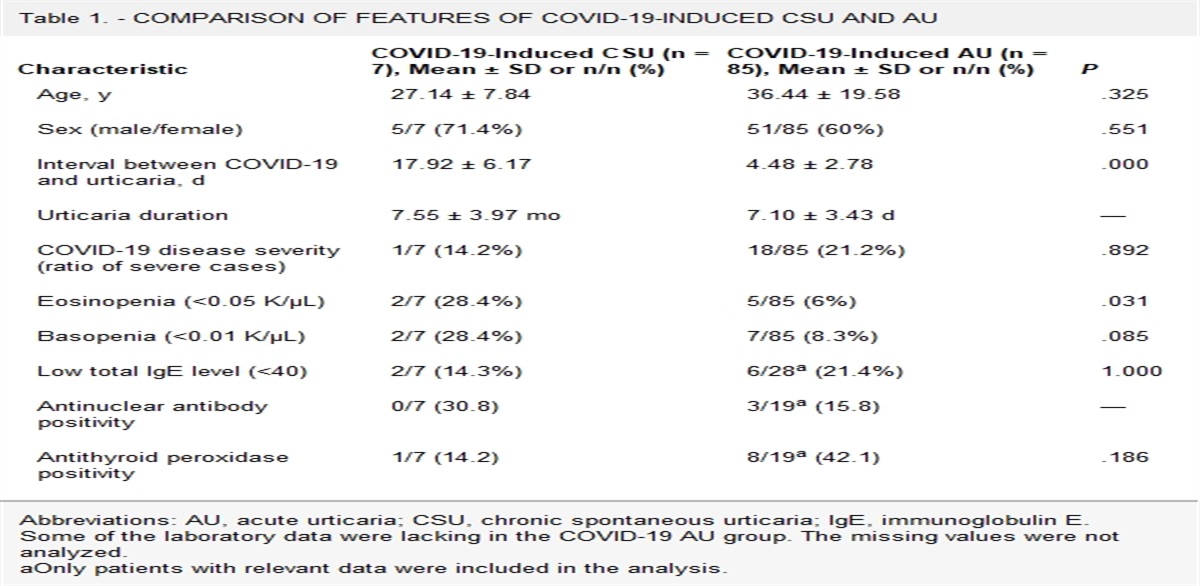
Combination TreatmentPolymerase chain reaction identifications revealed a persistent multibacterial infection in the patient’s PI growing Pseudomonas aeruginosa, Acinetobacter baumannii, and group D Streptococcus. Because standard treatments were followed by a rapid recurrence of the bacterial contamination, the provider elected to try a combination treatment that included low-pressure jet lavage irrigation in addition to applying a buffered sodium hypochlorite solution to the wound with a squirt bottle followed by a gel version of the same product. The flow pressure of the pulsatile irrigator was assessed using a computer-assisted force plate, finding that the pressure at the high irrigator setting averaged 8.5 pounds per square inch (PSI) with average flow rate of 810 cc per minute (Figure 2).
 Figure 2.:
Figure 2.: COMPUTERIZED FORCE PLATE ASSESSES IRRIGATION FLOWThe force plate for assessing flow pressure typically measured average forces 8.5 pounds per square inch (PSI) for pulsatile irrigators. For squeeze bottles, this force was less than 1 PSI.
When low-pressure jet lavage irrigation was added to treatment with 3 L of 0.9% sodium chloride solution (saline) for wound cleansing, the wound appeared dark with AFI, consistent with reduction of bacterial tissue levels to below 100 bacteria CFUs/g. However, when not performed daily, the wound quickly appeared contaminated, with variable clinical signs of drainage and odor. According to the image results, the author estimated this contamination could become log 6 to log 8 CFUs.
No jet lavage irrigation treatment occurred from Friday morning to Monday, typical for the author’s therapy department. The nursing service performed daily saline wash and applied saline-soaked dressings. By Monday morning, after 72 hours of irrigation delay, the wound typically had moderate to heavy recurrence of bacterial contamination (more than log 6 CFUs/g).
On February 15, 2021, a change occurred with the posttreatment AFI, revealing much less clearance of the imaged bacterial porphyrin. Because all products were FDA licensed, the author decided to try irrigating the standard 3 L of saline and adding a 250-cc bottle of the antimicrobial irrigated through the pulsatile irrigator. There seemed to be a significant positive effect, and this became the protocol until the end of treatment. The patient and provider noticed over a long weekend, without irrigation after Friday morning until the following Monday morning, that a rich “red” AFI appearance of the wound occurred. This was a much brighter red than seen when daily consecutive treatments were done during the week with the normal antimicrobial treatment. The effect of that “special” treatment was then documented through April 11, 2022.
What the author eventually determined was that the greater trochanter and the ischial areas of involvement were not bacteria-free. These areas were chronically seeding the sacral wound with new bacteria through a deep channel. This was shown by eventual breakdown of small wounds over these areas. These were treated using the long tip irrigators and eventually resolved completely. Importantly, none of the other similar severe stage 4 pelvic PIs in the study showed this problem.
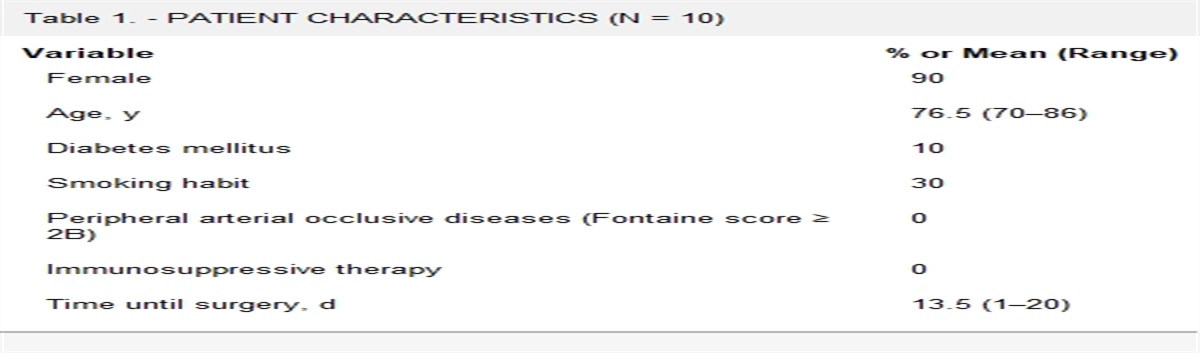
OutcomesA total of 21 imaged treatment pairs (pretreatment/posttreatment) occurred over the weekends. The AFI contamination exceeded log 4 CFUs/g of tissue in all pretreatment examinations and was reduced to less than log 2 CFUs (black) in 6 of 21 (28%) posttreatment examinations, with the remaining 15 showing an estimated 80% or higher removal of the bacterial porphyrin “red” appearance (Figure 3).
 Figure 3.:
Figure 3.: AFI BEFORE AND AFTER JET LAVAGE IRRIGATION WITH SALINEA, Autofluorescence imaging of stage 4 pelvic PI with more than log 6 CFUs/g of tissue after treatment delay of 3 days. Note heavy “red” porphyrin imaging and small white dots that are bacterial clusters. B, Wound is irrigated with pulsatile irrigator at 8.5 PSI with flow rate of 810 mL per minute with 3 L saline, removing over 80% of the “red” porphyrin imaging.Abbreviations: AFI, autofluorescense imaging; CFUs, colony-forming units; PI, pressure injury; PSI, pounds per square inch.
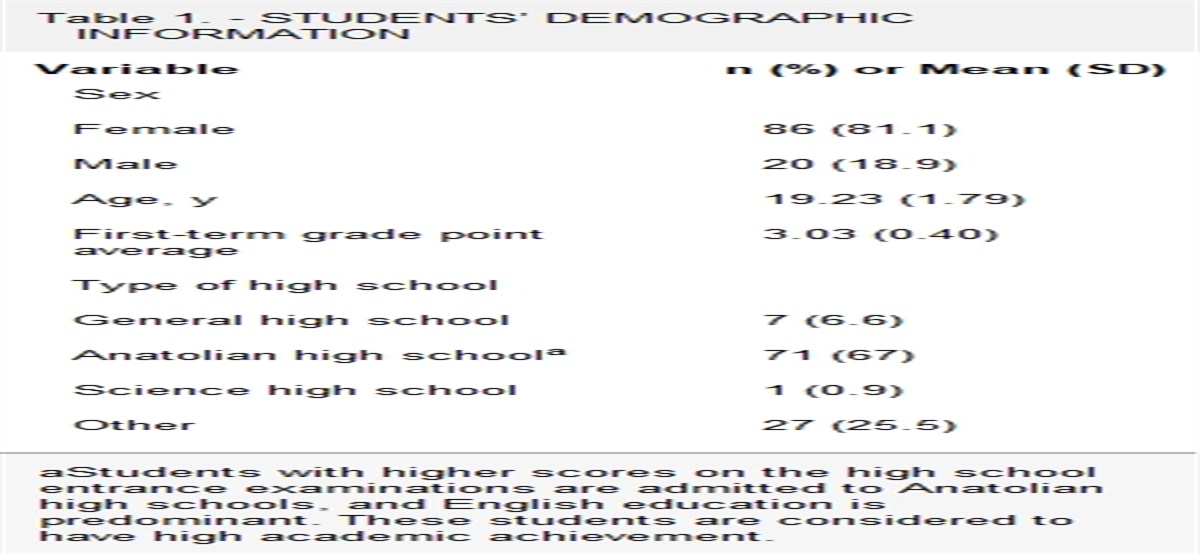
A total of 54 combination treatments occurred during the trial combining antiseptic with saline irrigation. There were 34 performed during the week with daily consecutive treatments (63%). There were no complications documented from use of the antimicrobial through the irrigator. Including treatments performed during the week, 20 of the 54 combination treatments (37%) revealed a completely “black” wound imaged with AFI, indicating less than log 2 CFUs (Figure 4).
 Figure 4.:
Figure 4.: AFI BEFORE AND AFTER JET LAVAGE IRRIGATION WITH SALINE AND ANTIMICROBIALA, Autofluorescent imaging of stage 4 pelvic PI prior to irrigation with pulsatile irrigator and 3 L of saline. B, Imaging after combination irrigation with 3 L of saline and 250 mL of buffered sodium hypochlorite solution, showing virtually all of deep “red” porphyrin imaged bacteria removed.Abbreviations: AFI, autofluorescent imaging; PI, pressure injury.
DISCUSSIONThis report describes the effect of delivering a 250-cc bottle of a standard antimicrobial to a difficult wound by using a low-pressure pulsatile irrigator. The results are positive, and of the total group of combination treatments, 37% were “black” wounds with AFI, indicating less than log 2 CFUs/g of tissues. These results are not surprising, given the biofilm challenge of the bacteria present in the wound. The “black” appearance with AFI is an important treatment target because the host physiologic agency is likely capable of eradicating contamination at this level, as described by Wright et al.9 The surgical concept is that this level of contamination is not likely to lead to a bacterial infection.
This case was unusual in its recalcitrance. Six other patients with chronic stage 4 pelvic PIs who received the same combination treatment all responded after only a few treatments without recurrence of detectable autofluorescence.10 For the present case, the poor response can perhaps be attributed to the very large chronic wound that could not be controlled of the bacterial contamination. However, the effect of the antimicrobial treatment is realistically documented, and the author was confident in the improvements offered. Notably, the deep undermined area was treated by similar irrigation over several months and appeared to have resolved.
There are few in vivo studies that offer evidence regarding bacterial clearance with antimicrobials. This requires quantitative bacterial culture and, in recent years, the use of quantitative polymerase chain reaction technologies to estimate infection at log 5 to 6 CFUs/g. However, AFI has emerged as a compelling method to measure bacterial contamination at a point-of-service setting.4–6 The extensive Fluorescence Imaging Assessment and Guidance Trial by Serena and coauthors8 confirmed the specificity of this technology, with 82% of wounds having bacterial loads greater than log 4 CFUs/g tissue. However, 85% of assessments utilizing clinical signs missed this detection.8
Biofilm produced by most bacteria can limit the effectiveness of antimicrobials by enveloping the “persister” bacteria with a protective matrix. Davison et al11 characterized this phenomenon as the reaction diffusion effect. This concept states that highly reactive antiseptic drugs react very quickly on the surface of the biofilm matrix, effectively becoming neutralized.11 These drugs cannot penetrate enough to destroy the deeper bacterial persisters. This problem is the primary reason justifying mechanical debridement to physically disrupt the biofilm bacterial matrix.
Low-pressure jet lavage is a simple and highly effective disruptor of the biofilm matrix because the bond to the underlying substrate is finite and can be overcome by this treatment.12–14 Bench laboratory studies reveal that, depending on the bacterial species involved, irrigation removes 75% to 92% of the biofilm with jet lavage.15,16 In 1994, the Agency for Healthcare Research and Quality regulated fluid force not to exceed 15 PSI.17 The ultimate mean pressure of the irrigator should be 8 to 9 PSI. Although better biofilm removal is possible with higher pressures, the safety factor makes the lavage system desirable in all settings and by midlevel providers in the clinic. That was the treatment context for this patient, who received all treatment at the bedside in the nursing home.
Each chronic wound has a spectrum of bacterial contaminants ranging from planktonic, highly active, cell-dividing bacteria to those with intermediate activity levels that are seeking surface attachment for colonization, to very low activity “persisters” whose morphologic features enable them to evade and resist the human host inflammatory system. Short of operative surgical debridement by an expert, or the use of antiseptics and antibiotics that are potentially toxic to local tissues, the “persisters” will not be destroyed by common treatment modalities. However, the local host inflammatory system can identify and destroy those “persister” bacteria. Thus, the goal of clinical wound treatment can be defined as reducing biofilm bacterial contamination to less than log 2 CFUs/g tissue such that the host can manage the local “persisters.”
The current literature supports the concept that independent antiseptic use cannot remove or control chronic biofilm matrix. Johani et al18 tested a large variety of antiseptics and found that short time exposures, as typically performed in standard clinical practice, were inadequate. The squirt bottles, which have a force of 1 PSI based on the author’s force place tests, are inadequate to disrupt the biofilm substrate interface. Generally, only mechanical debridement with surgical excision or the jet lavage irrigators can clear log 5 to 6 CFUs/g contamination to less than log 2. However, there appears to be a place for antiseptics as an adjunct to destroy planktonic and faster-multiplying bacteria. This synergy is a relevant treatment goal, particularly if that biofilm suppression can be extended for several days. Ultimately, the host must have the capability to handle the phenotypic “persisters” that will not be destroyed by these means.9 If that does not occur during treatment, the surgeon and patient are faced with difficult choices, possibly even tissue ablation.
CONCLUSIONSThe evidence presented supports that jet lavage wound irrigation is a valuable treatment for contaminated and infected wounds. The antiseptics applied are a significant adjunct treatment but cannot be relied on for primary mechanical debridement. Autofluorescence imaging provides excellent point-of-care information that may inform treatment and future strategies.
REFERENCES 1. Percival SL, McCarthy SM, Lipsky B. Biofilms and wounds: an overview of the evidence. Adv Wound Care 2015;4(7):373–81. 2. Percival SL, Finnegan S, Donelli G, Vuotto C, Rimmer S, Lipsky BA. Antiseptics for treating infected wounds: efficacy on biofilms and effect of pH. Crit Rev Microbiol 2016;42:293–309. 3. Wolcott R. The role of biofilms: are we hitting the right target? Plast Reconstr Surg 2011;127:28S–37S. 4. Rahma S, Woods J, Brown S, Nixon J, Russell D. The use of point-of-care bacterial autofluorescence imaging in the management of diabetic foot ulcers: a pilot randomized controlled trial. Diabetes Care 2022;45:1601–9. 5. Rennie MY, Lindvere-Teena L, Tapang K, Linden R. Point-of-care fluorescence imaging predicts the presence of pathogenic bacteria in wounds: a clinical study. J Wound Care 2017;28:452–60. 6. Price N. Routine fluorescence imaging to detect wound bacteria reduces antibiotic use and antimicrobial dressing expenditure while improving healing rates: retrospective analysis of 229 foot ulcers. Diagnostics (Basel) 2020;10(11):927. 7. Jones LM, Dunham D, Rennie MY, et al. In vitro detection of porphrin-producing wound bacteria with real time fluorescence imaging. Future Microbiol 2020;15:319–32. 8. Le L, Baer M, Briggs P, et al. Diagnostic accuracy of point-of-care fluorescence imaging for the detection of bacterial burden in wounds: results from the 350-patient Fluorescence Imaging Assessment and Guidance Trial. Adv Wound Care (New Rochelle) 2021;10(3):123–36. 9. Wright AM, Fleming A, Colebrook L. The sterilization of wounds by physiological agency. War Med (Paris) 1918;2(2):203–6. 10. Stiehl JB. Antiseptics combined with jet lavage irrigation for biofilm bacterial control in severe stage 4 pelvic pressure injury: a case report. Adv Skin Wound Care 2023;36(8):441–6. 11. Davison WM, Pitts B, Stewart PS. Spatial and temporal patterns of biocide action against staphylococcus epidermidis biofilms. Antimicrob Agents Chemother 2010;54:2920–7. 12. Svoboda SJ, Bice TG, Gooden HA, Brooks DE, Thomas DB, Wenke JC. Comparison of bulb syringe and pulsed lavage irrigation with the use of a bioluminescent musculoskeletal wound model. J Bone Joint Surg 2006;88:2167–74. 13. Brown LL, Shelton HT, Bornside GH, Cohn I Jr. Evaluation of wound irrigation by pulsatile jet lavage and conventional irrigation. Ann Surg 1978;187:170–3. 14. Ho C, Bensitel T, Wang X, Bogie KM. Pulsatile lavage for the enhancement of pressure ulcer healing: a randomized controlled trial. Phys Ther 2012;92:38–48. 15. Deng Y-H, Ricciardulli T, Won J, et al. Self-locomotive, antimicrobial microrobot (SLAM) swarm for enhanced biofilm elimination. Biomaterials 2022;287:121610. 16. Rodeheaver GT, Smith SL, Thacker JG, Edgerton MT, Edlich RF. Mechanical cleansing of contaminated wounds with a surfactant. Am J Surg 1975;129(3):241–5. 17. Bergstrom N, Bennett MA, Carlson CE, et al. Treatment of Pressure Ulcers. Clinical Practice Guideline, No. 15. AHCPR Publication No. 95-0652. Rockville, MD: Agency for Health Care Policy and Research; 1994. 18. Johani K, Malone M, Jensen SO, et al. Evaluation of short exposure times of antimicrobial wound solution against microbial biofilms: from in vitro to in vivo. J Antimicrob Chemother 2018;73:494–502.
留言 (0)