
記住我

Venous leg ulcers (VLUs) are an increasingly common skin defect on the legs or feet.1 In China, the prevalence of VLUs is 1.8% but can be up to 3% among individuals older than 80 years.2 Among patients with more than 10 years of venous disease, the prevalence of VLUs is 10%, and the recurrence rate can reach 54% to 78%.3
Researchers typically evaluate ulcer healing time and rate as the primary outcome indicators, and there is less research on patients’ quality of life (QoL).4 However, comprehensive VLU management focuses on widespread problems and should not be limited only to the VLU itself.5 Quality of life refers to an individual’s feelings and experiences of his or her goals, expectations, and concerns in different cultural value systems.6 Taking patients’ QoL as the outcome indicator can reflect the new health concept and medical model and effectively compensate for the inadequacy of traditional indicators. Research indicates that QoL is generally lower among individuals with VLUs in comparison with those with no or less severe venous disease.7 In recent years, the Venous Leg Ulcer Quality of Life (VLU-QoL) questionnaire has been translated into Chinese8 and used to measure QoL among patients with VLUs.9 Xia et al9 found that QoL was low among these patients, so it is crucial to promote their QoL.
Many factors influence patients’ QoL, including disease characteristics, emotional response, self-efficacy, and social support.10,11 The occurrence of a VLU is a significant stressor: Pain, restricted mobility, depression, and social isolation cause patients severe distress, leading to a high risk of powerlessness. As a psychosocial phenomenon, powerlessness refers to the perception of a lack of control over recent and upcoming events, such that the person’s actions do not significantly affect the outcome.12 Most patients with a VLU have a strong sense of powerlessness because of the difficulty of healing and the high recurrence rate of the wound.13 In a clinical study, Huang et al14 found that in patients with chronic wounds, powerlessness was negatively associated with QoL.
Apart from psychoemotional responses (eg, powerlessness), coping resources or strategies (eg, self-efficacy and coping modes) are also relevant to patients’ QoL. Self-efficacy helps to measure individuals’ perceived ability to perform self-care behaviors.15 Improving self-care behaviors, such as elevating legs or wearing compression pressure socks correctly, can help prevent VLU recurrence.16 Thus, a high level of self-efficacy is a protective factor against VLU recurrence.17
Self-efficacy also relates to individuals’ ability to control their behavior and coping strategies (ie, coping mode).18 As an essential mechanism in the stress response, coping mode regulates and affects a person’s responses to stress. When faced with stressful events, individuals may adopt different ways of relieving stress, affecting their QoL. Confronting coping modes positively predict QoL, whereas avoidance and submission coping modes negatively predict QoL.19 Conversely, adopting a positive coping mode leads to more disease-related knowledge, improving self-management, and QoL.20
However, the relationship between powerlessness, self-efficacy, coping mode, and QoL in patients with a VLU remains unclear. Based on the stress and coping theory, this study analyzed the correlation between variables from the perspective of psychosocial factors. Further, the authors explored whether self-efficacy and coping mode mediate the relationship between powerlessness and QoL in patients with a VLU.
Research Model and HypothesesThis study was based on Lazarus and Folkman’s stress and coping theory.21 Stress results from the interaction between the individual and the external environment. When individuals believe that their resources and abilities cannot meet the needs generated by internal and external environmental stimuli, homeostasis is disrupted, and stress is generated. According to this theory, coping with stress includes stressors, cognitive appraisal, coping, and outcomes. Stressors are factors that threaten an individual’s survival or health. Cognitive appraisal refers to the individual’s view and judgment of external stimuli, including psychological activities such as perception, thinking, and decision-making. Among them, primary appraisal reflects the individual’s perception of whether the environmental stimulus is related to the self and the strength of the relationship. A secondary appraisal is the appraisal of the individual’s ability to cope with stress, the choice of coping mode, and the acquisition of coping resources. Coping is a cognitive behavioral mode individuals adopt to respond to external stressors. The final coping outcome will have a corresponding impact on the individual’s stress adaptation outcome.
Drawing on theories of stress and coping, the researchers developed a conceptual model for the study (Figure 1). The long-term presence of ulcers leads to several adverse physical and psychological reactions in patients, coupled with the lack of effective treatment and uncertainty about the prognosis of the disease. If a VLU is considered a potential stressor acting on the individual, the resulting primary cognitive evaluation by the patient is a sense of powerlessness. On the other hand, self-efficacy, as an essential internal resource of the individual, directly affects the results of the patient’s secondary evaluation and further influences the coping mode. Ultimately, it may lead to changes in stress adaptation outcomes regarding QoL. The relationship between helplessness, self-efficacy, coping mode, and QoL in patients with VLUs has not been investigated. According to previous research and the theoretical framework of stress and coping, the hypotheses were:
 Figure 1.:
Figure 1.: HYPOTHESIZED CONCEPTUAL MODEL BASED ON LAZARUS AND FOLKMAN’S THEORY OF STRESS AND COPINGNote that a1 is the direct effect of powerlessness on self-efficacy; a2 is the direct effect of self-efficacy on coping mode; a3 is the direct effect of coping mode on quality of life; b1 is the direct effect of powerlessness on coping mode; b2 is the direct effect of self-efficacy on quality of life; c is the direct effect of powerlessness on quality of life; and c’ is the total effect of powerlessness on quality of life.
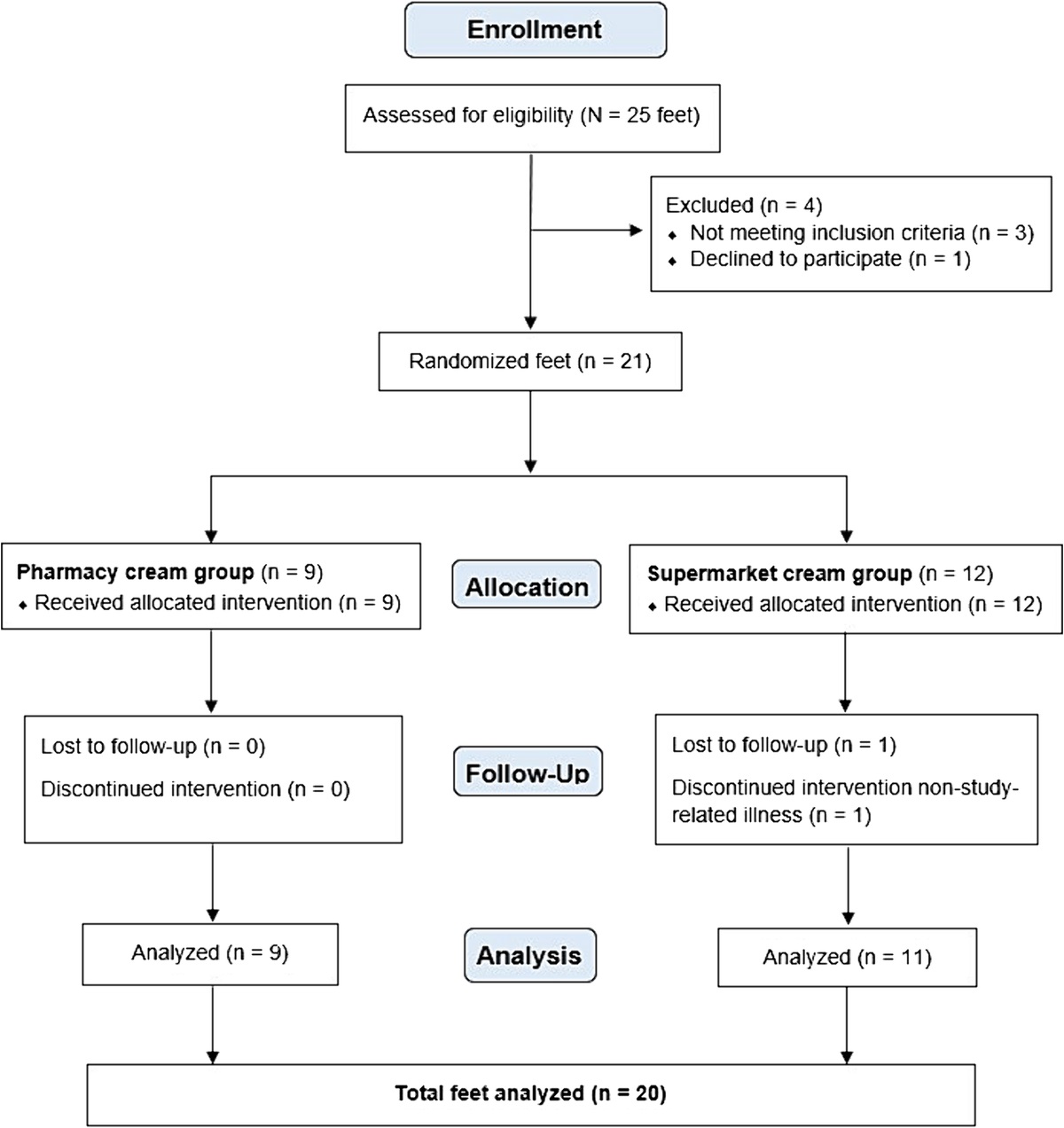
Hypothesis 1: Powerlessness is negatively correlated with QoL. Hypothesis 2: Self-efficacy may mediate the relationship between powerlessness and QoL. Hypothesis 3: Coping mode may mediate the relationship between powerlessness and QoL. Hypothesis 4: Self-efficacy and coping mode may mediate the relationship between powerlessness and QoL. METHODS Design and ParticipantsIn this cross-sectional study, the authors used convenience sampling to select patients with VLUs who were treated in four tertiary grade A hospitals in Qingdao and Tianjin from June 2021 to August 2022. Patients were included in the study if they were clinically diagnosed with VLU (suitable for compression therapy), 18 years old or older, able to communicate, and they volunteered to participate. Patients with psychiatric disorders, dementia, or other significant medical conditions were excluded from the study.
G*Power software (University of Düsseldorf) was used for sample size calculation. With α of .05, power of 0.95, median effect size of 0.15, and predictor of 9, approximately 166 participants would be required for the study. The researchers distributed a total of 220 questionnaires and collected 208 valid, completed questionnaires, an effective recovery rate of 94.55%.
Measures General informationThe researchers created a demographic questionnaire to collect data on patient characteristics. The questionnaire includes sociodemographic information and basic information about the patient’s disease.
Powerlessness Assessment ToolThe Chinese version of the Powerlessness Assessment Tool was used to assess the level of powerlessness among patients with VLUs.22 The scale includes 12 items and two dimensions. Each item was scored from to 1 (never) to 5 (always), with higher scores corresponding to stronger feelings of powerlessness. The scale has good reliability and validity, with an overall Cronbach α of .96, meaning it is suitable for use with Chinese patients with chronic wounds.22 The Cronbach α in the present research was .862.
Venous Leg Ulcer Self-efficacy Tool (VeLUSET)The VeLUSET was developed by Brown et al23 based on Bandura’s self-efficacy theory. It includes five dimensions, each with 30 items. Each item is scored from 0 (completely disagree) to 10 (completely agree). The researchers used the revised Chinese version of the VeLUSET, which has a Cronbach α of .917.24 In this study, the Cronbach α was .956.
Medical Coping Modes Questionnaire (MCMQ)The authors used the revised MCMQ to evaluate patients’ coping status.25 The MCMQ includes 20 items in three dimensions: confrontation, avoidance, and submission. The corresponding Cronbach αs were .69, .60, and .76, respectively, which indicate good reliability and validity.25 The scale is scored using a 4-point Likert-type scale; eight items are reverse scored. Higher scores on a dimension indicate that individuals are more inclined to adopt this coping mode. In the present study, the Cronbach αs were .872, .854, and .870, respectively.
Venous Leg Ulcer Quality of Life QuestionnaireThe VLU-QoL was compiled by Hareendran et al26 to assess the QoL of patients with VLUs over the previous 4 weeks. The Chinese version has 34 items, covering three dimensions: daily life, subjective feelings, and local symptoms.8 Items on the scale are scored from 0 to 4, with higher scores representing worse QoL. The Cronbach α was .923 in the present research.
ProcedureThis study was approved by the relevant committees and officials (no. QDU-HEC-2022215). All researchers involved in data collection (the first, third, and fourth authors) received uniform training in collecting questionnaire data to ensure consistency and minimize bias in the investigation process. Questionnaires were collected in the wound or vascular surgery clinics and wards of four different hospitals. The corresponding author contacted the medical staff at the relevant hospitals and departments to ask for permission and cooperation. With the help of doctors or nurses, researchers explained the study purpose and significance to eligible participants.
After obtaining informed consent, researchers distributed the questionnaires and informed the participant about the requirements for completion. For patients who could not complete questionnaires independently because of physical weakness, visual impairment, or other reasons, researchers read the questionnaire verbatim and completed it on behalf of the patients based on their answers. Researchers prepared small gifts (eg, masks and tissues) to thank patients for participating.
Data AnalysisThe researchers used SPSS 26.0 (IBM Corp) to analyze the data. Participants’ general information, powerlessness, self-efficacy, coping modes, and QoL were analyzed with descriptive statistics. For between-group comparisons, the authors used a t test and one-way analysis of variance. Correlations between variables were assessed using Pearson correlation analysis.
This study used a chain mediation model to explore the mediating order of self-efficacy and coping modes between powerlessness and QoL based on stress coping theory and the previous literature. Because there was a statistically significant bivariate correlation between the variables, the researchers used PROCESS macro and bootstrap methods to analyze the hypothesized mediation model. The bootstrap method was used to estimate the 95% CI with 5,000 repeated samplings and a two-sided inspection level with α = .05.
RESULTS General Characteristics of the SampleA total of 208 patients with VLUs participated in this study. They ranged in age from 43 to 88 (mean, 70.2 ± 8.84) years, and 69.7% (n = 145) were men (Table 1). Patients’ QoL scores differed significantly by economic income (F = 11.966, P < .001), current number of ulcers (t = −3.801, P < .001), ulcerated limb (t = −3.434, P = .001), ulcer recurrence (t = 3.081, P = .002), degree of ulcer pain (F = 22.950, P < .001), and Venous Clinical Severity Score (F = 6.935, P < .001).
Table 1. - PATIENT DEMOGRAPHICS AND VLU-QoL SCORES (N = 208) Variable n (%) VLU-QoL Scores, Mean (SD) t/F P Age, y 1.530 .128 <60 27 (14.8) 73.48 (20.62) ≥60 181 (85.2) 67.44 (18.91) Sex -1.250 .213 Male 145 (69.7) 67.13 (19.88) Female 63 (30.3) 70.75 (17.40) Place of residence -1.216 .226 Urban 147 (70.7) 67.28 (20.32) Rural 61 (29.3) 70.51 (16.10) Education level 1.606 .203 Primary school and below 75 (36.1) 69.04 (19.54) Middle school 92 (44.2) 65.85 (18.19) High school and above 41 (19.7) 72.07 (20.46) Economic income, RMB per mo 11.966 < .001 <2,000 45 (21.6) 75.36 (17.57) 2,000-4,000 79 (38.0) 72.00 (19.00) >4,000 84 (40.4) 60.86 (17.89) Cohabitation status 1.392 .165 Living alone 44 (21.2) 71.80 (18.54) Not living alone 164 (78.8) 67.27 (19.31) Present number of ulcers -3.801 <.001 1 158 (76.0) 65.47 (18.30) ≥2 50 (24.0) 76.54 (19.53) Ulcerated limb -3.434 .001 Unilateral limb 167 (80.3) 66.02 (19.13) Bilateral limbs 41 (19.7) Ulcer recurrence 3.053 .003 Yes 101 (48.6) 72.33 (17.70) No 107 (51.4) 64.36 (19.82) Current ulcer duration, m 0.859 .463 <3 123 (59.1) 66.52 (19.26) 3-6 36 (17.3) 69.81 (20.88) 7-12 21 (10.1) 72.19 (17.71) >12 28 (13.5) 70.71 (17.76) Degree of ulcer pain 22.950 <.001 Painless 29 (13.9) 55.52 (15.71) Mild pain 79 (38.0) 61.28 (15.92) Moderate pain 59 (28.4) 73.37 (18.47) Severe pain 41 (19.7) 83.20 (16.25) VCSS 6.935 <.001 <10 35 (16.8) 57.46 (15.88) 11-15 57 (27.4) 65.67 (16.80) 16-20 74 (35.6) 71.58 (20.70) >20 42 (20.2) 74.76 (18.18)Abbreviations: VCSS, Venous Clinical Severity Score; VLU-QoL, Venous Leg Ulcer Quality of Life Questionnaire.
Table 2 shows descriptive statistics and correlations among relevant variables. The powerlessness score was negatively associated with self-efficacy (r = −0.548, P < .001) and with confrontation coping mode (r = −0.489, P < .001) and was positively associated with QoL (r = 0.544, P < .001). The QoL score was negatively correlated with self-efficacy (r = −0.545, P < .001) and confrontation coping mode (r = −0.564, P < .001). Submission and avoidance coping modes were not significantly correlated with powerlessness.
Table 2. - CORRELATION ANALYSIS OF POWERLESSNESS, SELF-EFFICACY, COPING MODES, AND QoL IN PATIENTS WITH VLUs (N = 208) Variables Powerlessness Self-efficacy Confrontation Avoidance Submission QoL Powerlessness 1 Self-efficacy −0.548a 1 Confrontation −0.489a 0.539a 1 Avoidance 0.056 −0.104 0.058 1 Submission 0.101 −0.193b −0.156b 0.200b 1 QoL 0.544a −0.545a −0.564a 0.186b 0.092 1 Mean (SD) 32.34 (9.38) 205.41 (45.55) 20.21 (5.90) 15.65 (5.42) 11.38 (3.77) 68.23 (19.20)Abbreviations: QoL, quality of life; VLU, venous leg ulcer.
aP < .001 (two-tailed).
bP < .01 (two-tailed).
All paths between variables in the assumed model were significant when covariates were considered. Powerlessness significantly negatively predicted self-efficacy (β = −.38, t = −5.17) and confrontation coping mode (β = −.16, t = −2.20). Self-efficacy significantly positively predicted confrontation coping mode (β = .33, t = 4.91). When powerlessness, self-efficacy, and confrontation coping mode were entered into the regression equation at the same time, powerlessness negatively predicted QoL (β = .19, t = 2.83); self-efficacy (β = −.20, t = −3.01) and confrontation coping mode (β = −.24, t = −3.76) positively predicted QoL. The specific coefficients are displayed in Table 3 and Figure 2.
Table 3. - RESULTS OF THE REGRESSION ANALYSES TESTING THE SERIAL MULTIPLE MEDIATION EFFECT OF SELF-EFFICACY AND CONFRONTATION COPING MODE IN THE RELATIONSHIP POWERLESSNESS AND QoL (N = 208) Direct Effect Total Effect Self-efficacy Confrontation Coping Mode Quality of Life Quality of Life Predictors β t β t β t β t Economic income 0.13 2.01a 0.14 2.25a −0.01 −0.23 −0.08 −1.37 Ulcer number −0.11 −1.65 0.09 1.50 0.03 0.60 0.04 0.68 Ulcerated limb 0.01 0.17 −0.13 −2.15a 0.18 3.16b 0.21 3.45b Ulcer recurrence −0.02 −0.40 −0.07 −1.13 0.01 0.27 0.04 0.65 Ulcer pain −0.18 −2.62b −0.15 −2.29a 0.15 2.51a 0.24 3.75c VCSS −0.02 −0.29 −0.02 −0.33 0.10 1.78 0.11 1.82 Powerlessness −0.38 −5.17c −0.16 −2.20a 0.19 2.83b 0.34 4.93c Self-efficacy 0.33 4.91c −0.20 −3.01b Confrontation −0.24 −3.76c R2 0.33 0.38 0.49 0.41 F 15.59c 16.90c 23.47c 21.76cAbbreviations: QoL, quality of life; VCSS, Venous Clinical Severity Score.
aP < .01.
bP < .001.
cP < .001.
 Figure 2.:
Figure 2.: SERIAL MULTIPLE MEDIATION MODEL WITH SELF-EFFICACY AND CONFRONTATION COPING MODE AS MEDIATORS IN THE RELATIONSHIP BETWEEN POWERLESSNESS AND QUALITY OF LIFE (N = 208)*P < .05, **P < .01, ***P < .001.
To better examine the significance of the mediating effect, the authors used the bootstrap method to calculate the 95% CI of the mediating effect. Powerlessness affected the QoL of patients with VLUs through three indirect effect paths, and the mediating effect’s total effect size was 0.29 (95% CI, 0.16-0.45). Self-efficacy and confrontation coping mode were the mediating variables affecting QoL. Powerlessness affects QoL both directly and indirectly through self-efficacy and confrontation coping mode. In other words, the mediating effect of self-efficacy and confrontation can be achieved through the following three paths: path 1 (point estimate, 0.150): powerlessness → self-efficacy → QoL; path 2 (point estimate, 0.080): powerlessness → confrontation coping mode → QoL; path 3 (point estimate, 0.062): powerlessness → self-efficacy → confrontation coping mode → QoL. The above 95% CIs did not include 0, further validating that self-efficacy and confrontation coping mode mediate between powerlessness and QoL. The specific paths are shown in Table 4.
Table 4. - BOOTSTRAPPED POINT ESTIMATES FOR ALL INDIRECT EFFECTS (N = 208) Bootstrap 95% CI Point Estimate Standard Error Lower Upper Path 1: PS → SE → QoL 0.150 0.059 0.049 0.278 Path 2: PS → CCM → QoL 0.080 0.043 0.011 0.177 Path 3: PS → SE → CCM → QoL 0.062 0.025 0.021 0.118 Total indirect effect 0.292 0.076 0.156 0.453Abbreviations: CCM, confrontation coping mode; PS, powerlessness; QoL, quality of life; SE, self-efficacy.
Note. If the CI does not include 0, the effect is statistically significant at P < .05.
This study comprehensively explored the role of self-efficacy and coping mode in mediating powerlessness and QoL among patients with VLUs. In addition to the mediating chain pathway, two mediating pathways with either self-efficacy or confrontation coping mode as the single mediator were significant between powerlessness and QoL.
The mean score of powerlessness (32.34 ± 9.38) was at an intermediate level. This finding was similar to those of Brazilian scholars for patients with VLUs and Chinese scholars for patients with chronic wounds.12,14 The mean QoL score of patients with VLUs was 68.23 ± 19.20, which similarly reflected previous research.9,27 A previous study found that ulcers were more likely to occur in low-income groups, whose QoL was lower than that of employed patients.12 Patients with VLUs require frequent wound treatment, which places a heavy financial burden on low-income patients, reducing their QoL.
Further, the prevalence of pain in patients with VLUs is as high as 90%.28 Pain also adversely affects QoL. When pain leads to restricted limb movement, patients with VLUs may have negative psychological reactions, which further affect QoL. In the present study, 48.6% of patients with VLUs had ulcer recurrence, and those with recurrence had a significantly lower QoL. In addition, patients with multiple ulcers or bilateral limb involvement had worse limb dysfunction, further reducing their QoL, in accordance with previous research.29
Powerlessness directly impacted patients’ QoL, further verifying hypothesis 1. Previous research found that patients’ powerlessness negatively correlated with their QoL.14 The direct impact can be explained by the characteristics of the disease itself: the lack of effective treatment and unpredictability of outcomes for VLUs lead to adverse psychological reactions such as powerlessness, which further severely affects the QoL. Further, powerlessness may indirectly affect QoL through self-efficacy and coping modes. These two variables are relevant for negative psychological emotions and QoL, supporting the indirect impact of powerlessness on QoL.30 Self-efficacy and confrontation coping mode each played a separate mediating role in the relationship between powerlessness and QoL.
Self-efficacy is based on beliefs rather than actual abilities. The mean self-efficacy score in this study was 205.41 ± 45.55, indicating that patients’ self-efficacy could be further improved, especially in daily self-care tasks and developing expertise. Further, self-efficacy and QoL were correlated, which aligns with previous research.11,31 Individuals’ psychological response when confronted with a particular activity influences their evaluation of their ability and thus affects their self-efficacy.15 Powerlessness is a negative psychosocial phenomenon. Patients with higher powerlessness had lower self-efficacy in disease management, consistent with other research.32 Thus, powerlessness may further impact patients’ QoL by influencing self-effi
留言 (0)