
Remember me




Congestive heart failure, commonly known as heart failure (HF), is a chronic disease caused by insufficient pumping of blood by the heart.1 Recent evidence reports that 83% of patients with HF are admitted to the hospital at least once per year.2 One possible intervention for patients with end-stage HF who are not responsive to guideline-directed medical therapy is orthotopic heart transplantation (OHT).2 Unfortunately, donor heart availability is and continues to be limited, resulting in lengthy waitlist times for a large population of patients. Following the 2018 modifications to the United Network for Organ Sharing allocation for heart donor policy, the use of both temporary mechanical circulatory support (MCS) devices and destination therapy left ventricular assist devices (LVADs) has significantly increased in the pretransplantation setting.3 For patients admitted with acute decompensated HF and cardiogenic shock, MCS devices such as Impella microaxial flow catheter (Abiomed) and intra-aortic balloon pump (IABP) have been increasingly used in hospital settings to serve as a bridge to sustain organ function and stabilize hemodynamics.4 Patients with MCS devices may recover without further need for interventions, undergo an LVAD evaluation, or be worked up for heart transplant consideration and may be placed on a transplant waitlist.
The Impella device is a catheter-based ventricular assist device placed in the left ventricle via the axillary or subclavian artery. The device helps pump blood from the left ventricle into the ascending aorta at a rate between 2.5 and 5.0 L/min increasing cardiac output. This allows unloading of the left ventricle and decreased myocardial oxygen demand.5 The IABP is another MCS device that is placed in the proximal descending aorta via the axillary or subclavian artery. The balloon is inflated during diastole to increase coronary perfusion and is then deflated before systole to decrease afterload. This increases myocardial oxygenation, indirectly improves cardiac output, enhancing organ perfusion and reducing left ventricular workload.6
Traditionally, MCS devices were placed percutaneously via the transfemoral arterial approach.7 Despite the fact that ambulation of select patients with an IABP inserted into the femoral artery appears to be safe,8 at the authors' institution, the catheter is moved to axillary or subclavian placement to allow for fewer mobility restrictions and safer mobility compared with femoral access. Per our hospital policy, patients with MCS devices must remain in an intensive care unit (ICU) and a registered nurse must be present during patient mobility to manage the MCS device for safety.
Patients with MCS devices are at risk for decreased functional mobility or prolonged bed rest due to high acuity and complexity of the devices. The effects of prolonged bed rest have been well-documented, and consequently, patients with MCS devices are at a high risk of those deleterious manifestations. Berg et al9 showed that 4 weeks of nonuse resulted in a 7% decline in muscle cross-sectional area in the quadriceps, and a 14% decline at 6 weeks.10 Dudley et al11 revealed an 18% to 20% reduction in peak torque of knee extensors after 1 month of bed rest. Daily ambulation and physical conditioning are essential for patients waiting for surgery and to prevent the negative consequences of prolonged bed rest or decreased mobility. Research has demonstrated that a combination of aerobic and resistive exercise can improve the functional mobility of patients with HF.12-14
At the authors' hospital, patients with MCS devices are usually referred to physical therapy services after device placement. Our standard of practice has allowed the physical therapist to use their own clinical judgment when deciding to transition these patients from physical-therapy-directed gait activity to nursing-led ambulation. This clinical judgment is based on the assessment of safe mobility and level of assistance for ambulation. However, decision-making varies from therapist to therapist without using objective data for an informed decision-making process. Nevertheless, a study from Macapagal et al15 discussed the nursing role in ambulating patients with an IABP. The study described the use of new nursing protocol, staff training, and intensive interdisciplinary collaboration between physical therapists and nursing staff. Fortunately, our institution has a strong culture of mobility with well-trained nurses and mobility aides who have participated in a standardized ambulation program with a wide variety of critical care patients for many years, including those with MCS devices. The delineation of responsibility between physical therapists and nurses has never been formally defined until this project.
In an effort to minimize overutilization and maximize the value of physical therapy resources, nursing-led ambulation has been used successfully with select patients in ICUs to meet the mobility needs of patients with MCS devices. The nurses only mobilize patients with MCS who have a higher functional level and do not have significant physical impairments that require individualized skilled intervention by a physical therapist. The nurses and nursing mobility aides also receive ambulation training from a physical therapist on an as-needed basis. By using this operational set-up, skilled physical therapy services can be more allocated to those patients who are medically complex or low-functioning and who require higher level rehabilitation resources.
Other literatures16-18 provide models of nursing-led mobility in acute care. These studies have used various assessment tools such as Activity Measure for Post-Acute Care (AM-PAC), John Hopkins Highest Level of Mobility (JH-HLM), and Banner Mobility Assessment Tool.16,19,20 Physical therapists use standardized functional outcome measurement tools to quantify patients' functional ability and predict the success of given functional tasks or activities. The outcome measures provide value in collectively comparing care and determining effectiveness.21,22 At this institution, we use the AM-PAC23,24 and the Perme ICU Mobility Score (Perme Score)25 as a standard of practice for objective mobility assessment in the ICU. In this study, we also included 5-m gait speed test (gait speed)25 to provide additional clinical picture of physical function.
There is limited evidence about the use of a cutoff score when transitioning ambulation from physical therapy to nursing service. Cutoff scores from certain outcome measures have been used to suggest patient discharge location26-28 and risk of frailty, rehospitalization, mortality, and morbidity,29-31 but never to support the transition of mobility responsibility while patients are still admitted in an acute care setting. The primary aim of this study is to explore the feasibility of using cutoff scores for AM-PAC, Perme, and gait speed to determine when it is most appropriate to transition ambulation from physical therapy service to nursing service. The secondary aim of this study is to describe the general characteristics of patients with axillary/subclavian MCS devices who receive acute care physical therapy services.
METHODS DesignThis study was an exploratory, pilot study to identify cutoff scores for 3 outcome measures (AM-PAC, Perme Score, and gait speed results) on when to transition patients to nursing-led ambulation. This study included patients who were admitted in the ICU at our hospital with a percutaneously placed subclavian or axillary MCS device (Impella and IABP), and who were referred for physical therapy services from December 2019 to December 2020. Patients referred to physical therapy services during their admission to the ICU received an initial physical therapy evaluation and subsequent follow-up intervention sessions in accordance with this hospital's standard practice. The Houston Methodist Hospital Institutional Review Board approved this study. The research protocol was strictly enforced during this study. All researchers involved in data collection completed in-depth training required as per the research protocol.
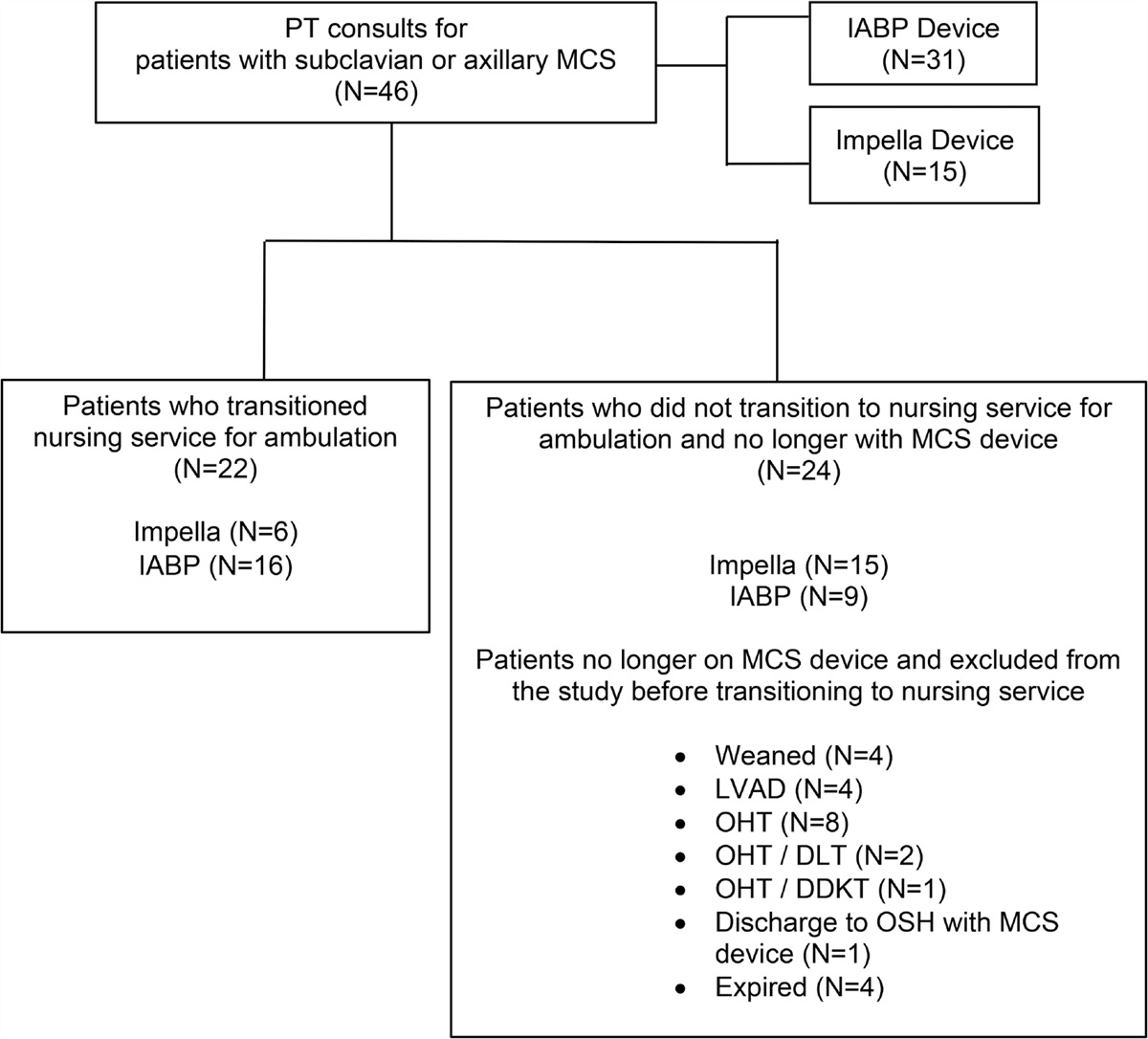
PatientsDue to the acuity of the medical condition and limited number of available target population patients, a sample of convenience (N = 46) was employed in this study using patients admitted in ICU at our hospital over a 12-month period. Our sample includes patients with a subclavian or axillary IABP (n = 31) or an Impella device (n = 15). Of the enrolled 46 patients, 22 patients were used in the data analysis for identifying cutoff scores for transitioning to nursing-led ambulation (see Figure 1). Patient inclusion criteria were (a) 18 years old and older and (b) able to meet the criteria to start physical therapy. These criteria included having an acceptable level of supplemental oxygen, hemodynamic stability, and the ability to purposefully participate in therapy. This research protocol identifies stable patients per expert consensus guidelines described by Hodgson et al.32 Exclusion criteria included patients with a femoral MCS device, on neuromuscular blocking agents, hemodynamic instability requiring more than 2 vasoactive agents, the presence of a femoral sheath, active bleeding, an open chest or abdomen, unstable fractures, a fraction of inspired oxygen of more than 60% and/or positive end-expiratory pressure of more than 12 cmH2O on ventilator, active bed rest orders, any diagnosis that prevents ambulation, previous enrollment in this study, non-English speaker, or cognitive inability to participate in physical therapy as determined by the completed prerequisite screening questions as part of the Medical Research Council Sum Score (MRC-SS) and orientation assessment. For those patients who were included in this study, collection of data was concluded when the patient no longer required MCS devices or were weaned off MCS devices, received a heart/organs(s) transplant, LVAD placement, were discharged to an outside facility, or died. Data collection was only performed while the MCS device was present; once the participants met exclusion criteria, their outcome measures and events were not part of the data analysis.
 FIGURE 1.:
FIGURE 1.: Consort Diagram. DDKT indicates deceased donor kidney transplant; DLT, double-lung transplant; IABP, intra-aortic balloon pump; LVAD, left ventricular assist device; MCS, mechanical circulatory support; N, number of patients; OHT, orthotopic heart transplant; OSH, outside hospital; PT, physical therapy; RN, registered nurse.
Data CollectionData collection occurred at initial and all subsequent physical therapy encounters. Initial enrollment data collection forms included demographic information, hospital and ICU admission and discharge dates, prior level of function, and MRC-SS.33 Per standard practice at our hospital, safety measures were observed on every encounter of physical therapy intervention. This included device position check on x-ray, device exit position check pre-/post-treatment, catheter anchor placement pre-/post-treatment, flow rates for the Impella device or ratio for the IABP device. During each encounter adverse events were monitored during and up to 10 minutes immediately following a physical therapy session, including nausea/vomiting, orthostatic hypotension, altered mental status, dislodgement of cannula, device malfunction, bleeding, and acute limb ischemia. Initial outcome measure scores are defined in this study as the scores at the time of physical therapy evaluation. The last scores are defined as outcome measure scores from the last therapy encounter before transitioning to nursing services or prior to patients meeting exclusion criteria.
The AM-PAC is applicable to all patients in the acute care setting. It is used to assess a patient's functional mobility beginning with bed mobility and ending in stair negotiation using a 4-point scale, ranging from 6 to 24. The AM-PAC has been validated for use by physical therapists in acute care; it has also been shown to correlate with discharge disposition.16,34,35 The Perme Score is used to objectively assess a patient's functional mobility in any ICU at a specific moment in time. It begins with assessing the patient's mental status and ends in the distance walked in 2 minutes. The Perme Score ranges from 0 to 32 and is derived from 15 items grouped into 7 categories. This score also incorporates environmental barriers specific to the ICU, such as mechanical ventilation, continuous infusions, and number of lines and tubes.25 Peterson et al36 reported the internal consistency, reliability, and content validity of the Perme Score, and Nawa et al37 reported interrater agreement and reliability of the Perme Score for the cardiovascular ICU patient population. For both the AM-PAC and the Perme Score, higher scores represent higher functional mobility. In this study, the term “gait speed” refers to self-selected comfortable gait speed over a 5-m distance described in meter/second (m/s).38 Kim et al39 reported validity of gait speed against physical function was higher with normal pace than with maximal pace. The authors used a stopwatch and a facility hallway with marked distance at various locations in the unit. The patient ambulated with or without an assistive device within the 5-m distance based on their functional ability. Initial gait speed refers to the first time the patient was able to ambulate in the hall during a physical therapy session. The MRC-SS measures muscle strength and uses a 6-point scale, ranging from 0 to 60. A higher score indicates greater muscle strength. The patient's ability to follow commands is initially assessed, followed by measuring the strength of 3 major muscle groups in all 4 limbs.33 Herman et al40 reported very good interrater reliability for the MRC-SS.
Data were collected for each physical therapy visit if the patient still had an MCS device and remained in the ICU. For safety, patients were monitored for 2 weeks through chart review after ambulation was transitioned to nursing. No adverse events were reported in chart review. Collection of data was discontinued if the inclusion criteria were no longer applicable, (ie, MCS device removed for heart/organ(s) transplant or LVAD, patient transferred to outside hospital, patient died, or MCS device weaned off and removed), or if patients unexpectedly met the exclusion criteria (ie, became hemodynamically unstable, >2 vasoactive medications, Fio2 >60%, etc). There were no missing data or dropouts to report.
Statistical AnalysisAll statistical analyses were performed using STATA 16 (StataCorp LLC, College Station, Texas). All categorical variables were presented as counts and percentages. Continuous variables were summarized as mean and standard deviation (SD) or median and interquartile range (IQR). The rank sum test was used to compare initial and last session outcome measures scores. Effect size (ES) was calculated using a general formula for nonparametric data. ES was calculated by dividing the Z value of Mann-Whitney U with the square root of sample size.41 Receiver operating characteristic (ROC) curves were constructed to create models in distinguishing target patients who can be ambulated by the nurses versus patients who continued to require skilled physical therapy interventions. Cutoff scores were identified to make recommendations on when to transition patients' ambulation to nursing service. An area under the curve (AUC) was used to provide visual approximation of the quality of the ROC curve in identifying the cutoff scores.42 The Liu method, as a default setting of STATA, was used to identify specific cutoff scores for the AMPAC, Perme Score, and gait speed values. The optimal cutoff scores were identified by using the product index that maximized the product of specificity and sensitivity using Liu method.43-44
RESULTS Baseline Patient CharacteristicsForty-six patients were included in this study from December 2019 to December 2020. Thirty-one patients had IABP devices, and 15 patients had Impella devices. The baseline demographics for all patients are summarized in Table 1. In this study, patients' mean age was 57.87 (SD 10.80) years and mean BMI was 28.87 (SD 5.35). Mean ICU length of stay was 43.30 (SD 37.86) days. Of the 46 patients in this study, 41 patients had left ventricular ejection fraction less than 40%. Prior to hospitalization, 45 patients were independent or modified independent for ambulation, and 42 patients were independent or modified independent in activities of daily living. Overall, 22 patients (IABP n = 16, Impella n = 6) were transitioned to nursing service for continuing ambulation. The remaining 24 patients were not transitioned to nursing, as they were deemed unsafe, required skilled physical therapy intervention for safe mobility, or because the MCS device was removed from them prior to transition for one of the following reasons: (1) receiving heart/organ(s) transplantation; (2) transitioned to LVAD; (3) weaned off from the MCS device; (4) discharged to another hospital; and (5) died prior to transition (see Figure 1).
TABLE 1. - Baseline Patient Characteristics (N = 46) All Patients (N = 46) Patients Who Transitioned to Nursing Service for Ambulation (n = 22) Patients No Longer on MCS Device and Excluded From the Study Before Transitioning to Nursing Service (n = 24) Age, mean (SD) 57.87 (10.80) 58.45 (10.80) 57.33 (11.01) Sex, male, n (%) 33 (71.74%) 17 (77.27%) 16 (66.67%) BMI, mean (SD) 28.87 (5.35) 29.22 (5.27) 28.56 (5.51) Race, n (%) Caucasian 23 (50%) 11 (50%) 12 (50%) African American 14 (30.43%) 9 (40.91%) 5 (20.83%) Other 9 (19.57%) 2 (9.09%) 7 (29.17%) MRC-SS, median (IQR) 55.5 (49-60) 60 (52-60) 54 (48-56) Admitting diagnosis, n (%) Cardiogenic shock 29 (63.04%) 14 (63.64%) 15 (62.5%) Other 17 (36.96%) 8 (36.36%) 9 (37.5%) PLOF, n (%) Ambulatory with/without AD 45 (97.83%) 22 (100%) 23 (95.83%) Nonambulatory with/without AD 1 (2.17%) 0 (0%) 1 (4.17%) LVEF% range, n (%) <30 severe 35 (76.09%) 19 (86.36%) 16 (66.67%) 30-39 moderate 6 (13.04%) 1 (4.55%) 5 (20.83%) 40-49 mild 3 (6.52%) 1 (4.55%) 2 (8.33%) 50-70 normal 2 (4.35%) 1 (4.55%) 1 (4.17%) MCS device, n (%) Impella 15 (32.61%) 6 (27.27%) 9 (37.50%) IABP 31 (67.39%) 16 (72.73%) 15 (62.50%) ICU LOS (SD), d 43.30 (37.86) 41.23 (18.54) 45.21 (49.83) Hospital LOS (SD), d 60.58 (38.39) 59.18 (20.37) 61.91 (50.47) Total number of PT sessions, mean (SD) 5.15 (5.32) 4.00 (4.33) 6.21 (5.99) Outcome, n (%) Weaned from MCS device 4 (8.70%) 0 (0%) 4 (16.67%) LVAD 8 (17.39%) 4 (18.18%) 4 (16.67%) OHT 22 (47.83%) 14 (63.64%) 8 (33.33%) OHT/DDKT 2 (4.35%) 1 (4.55%) 1 (4.17%) OHT/DLT 2 (4.35%) 1 (4.55%) 1 (4.17%) OHT/OLT 2 (4.35%) 1 (4.55%) 1 (4.17%) Discharged to OSH with MCS device 1 (2.17%) 0 (0%) 1 (4.17%) Died 5 (10.87%) 1 (4.55%) 4 (16.67%)AD, assist device; BMI, body mass index; DDKT, deceased donor kidney transplant; DLT, double-lung transplant; IABP, intra-aortic balloon pump; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; LVAD, left ventricular assist device; LVEF, left ventricular ejection fraction; MCS, mechanical circulatory support; MRC-SS, Medical Research Council Sum Score; OHT, orthotopic heart transplant; OLT, orthotopic liver transplant; OSH, outside hospital; PLOF, prior level of function; PT, physical therapy; SD, standard deviation.
When comparing the initial functional outcome measure scores to the last scores for all enrolled patients (N = 46), it shows significant differences (P < .05) with overall small ESs (d = 0.25-0.46) (see Table 2). Table 3 shows significant improvement in all 3 outcome measures after skilled physical therapy interventions (P < .05). Of the 22 patients who transitioned to the nursing-led ambulation program, only 15 were ambulatory during the initial physical therapy evaluation (see Table 3). The remaining 7 patients were unable to ambulate on the initial evaluation session based on clinical judgment by the therapist due to unstable hemodynamics, decreased muscle strength, and activity tolerance.
TABLE 2. - Pre-/Post-Comparison of 3 Functional Outcome Measures for All Patients (N = 46) Functional Outcome Measure Initial PT Scores Last PT Scores P Valuea Effect Size AM-PAC score, median (IQR) 17 (13-20) 20 (17-22) <.001b 0.46 Perme Score, median (IQR) 27.5 (22-29) 29 (27-30) .017b 0.25 Gait speed, median (IQR) 0.44 m/s (0.38-0.55)c 0.53 m/s (0.41-0.67) .006b 0.29AM-PAC, Activity Measure for Post-Acute Care; IQR, interquartile range; Perme Score, Perme ICU Mobility Score; PT, physical therapy.
aWilcoxon signed-rank test.
bStatistically significant.
cThirty-one patients completed their initial gait speed at the follow-up session.
AM-PAC, Activity Measure for Post-Acute Care; IQR, interquartile range; Perme Score, Perme ICU Mobility Score; PT, physical therapy.
aWilcoxon signed-rank test.
bStatistically significant.
Based on the ROC curve analysis (see Figures 2-4) of the 22 patients, the optimal cutoff scores representing a minimum score for transitioning to a nursing-led ambulation were (a) for AM-PAC score, a 19.5 raw score (>45.44 t-scale score) (AUC = 0.86), with sensitivity = 86%, and specificity = 75%, (b) for Perme Score 29.5 (AUC = 0.68), with sensitivity = 55%, and specificity = 75%, and (c) for gait speed, 0.57 m/s or more (AUC = 0.83), with sensitivity = 77%, and specificity = 82%.
 FIGURE 2.:
FIGURE 2.: Cutoff Score for Patients Transitioning to Nursing Service Using AM-PAC Score, ROC Graph (N = 22). AM-PAC indicates Activity Measure for Post-Acute Care; ROC, receiver operating characteristic curve.
 FIGURE 3.:
FIGURE 3.: Cutoff Score for Patients Transitioning to Nursing Service Using Perme Score, ROC Graph (N = 22). Perme Score indicates Perme ICU Mobility Score; ROC, receiver operating characteristic curve.
 FIGURE 4.:
FIGURE 4.: Cutoff Score for Patients Transitioning to Nursing Service Using Gait Speed (Meter/Seconds), ROC Graph (N = 15). Gait speed indicates 5-m gait speed; ROC, receiver operating characteristic curve.
Adverse Events During and After Physical Therapy SessionsOut of 237 total physical therapy encounters, we documented 6 adverse events during treatment sessions and only 1 after a treatment session. Adverse events documented during a physical therapy session were orthostatic hypotension (n = 3), nausea/vomiting (n = 2), and a new onset of arrhythmia (n = 1). The only adverse event after a physical therapy treatment session was nausea/vomiting (n = 1). The physical therapy session was stopped at the onset of an adverse event and patient safety was maintained.
Follow-up After Transition to a Nursing-Led AmbulationPatients were asked to track their daily ambulation for 2 weeks to ensure compliance with activity recommendations and to see whether this transition was successful. Patients documented their follow-up ambulation as distance in feet or, total number of laps around the unit (one lap is approximately 660 ft) on a calendar sheet provided to them. This ambulation was also documented by nursing in the electronic medical record under the mobility section. On average, patients walked 1 to 3 laps (660-1980 ft) more than 5 times a week with the nursing staff. None of the patients who were transitioned were referred back to physical therapy for mobility reasons.
DISCUSSIONThe main purpose of this study was to propose cutoff scores that can be used to transition ambulation from skilled physical therapy services to a nursing-led ambulation program. Since the AM-PAC and the Perme Score are always whole numbers, we suggest an AM-PAC score of more than 19 (>45.44 t score), Perme Score more than 29, and gait speed of 0.57 m/s or more.
The standard clinical practice at our hospital involved an initial physical therapy evaluation for patients with MCS devices. As patients' mobility and functional independence improved over time, the responsibility of ambulating the patient was transitioned to the nursing service. This transition of responsibility was done without the use of more definitive objective measurement in the decision process. Each physical therapist used their own expert clinical opinion for when to transition these patients.
At our hospital, a multidisciplinary approach to mobility has been used for many years. In a previous retrospective study by Macapagal et al,15 patients waiting for heart transplants with percutaneously placed axillary or subclavian IABPs were safely mobilized by nursing, consequently, avoiding the complications of prolonged bed rest. The authors in that study used Functional Independence Measure (FIM) scores as their functional outcome measure and only studied patients with IABPs. However, since FIM scores are no longer being used in our hospital, this study offers alternative functional outcome measures to use when deciding to transition patients to a nursing-led ambulation program.
Outcome measures have been used to assess physical function to justify current and future rehabilitation needs, predict functional improvement, and recommend discharge destination. Fernandez et al26 reported that an AM-PAC score of 18.5 was the optimal nonconverted cutoff value for discharging skilled acute care physical therapy to home. If patients have the functional ability to return home, they are likely no longer in need of skilled physical therapy services in the hospital or in a postacute care (PAC) facility. Patients with MCS devices (Impella and IABP) are unable to leave an ICU setting due to the nature of the devices. The outcome of this study recommends an AM-PAC score of more than 19, which is similar to Fernandez's guideline for discharge from skilled physical therapy services. The Whitlock et al27 prediction model indicates that patients in a cardiac ICU with lower AM-PAC scores had a higher chance of being discharged to a PAC facility. This recommendation supports our findings to keep patients with lower AM-PAC scores on the physical therapy caseload, rather than transitioning them to ambulate with nursing staff. Patients who are being discharged to a PAC facility may not be mobile enough for nursing staff to manage their daily functional activities. These suggestions may be able to help both physical therapy and nursing services better identify mobility responsibilities in the era of growing staffing difficulties.
Perme et al28 determined that patients with a higher Perme Score (>26/32) on initial physical therapy evaluation had a greater chance of returning home, whereas a lower Perme Score increased the likelihood of discharge to a PAC facility. However, this study results found that patients with MCS devices may require a higher Perme Score (>29/32) before transitioning the responsibility of ambulation to the nursing staff due to the complex nature of their monitoring devices and infusion needs.
Other studies29-31 have suggested that slower gait speed cutoff scores (<0.8 m/s) put patients at higher risk for frailty, hospitalization, mortality, and poor outcomes. While this study had a slower Gait Speed cutoff (≥0.57 m/s), this could be due to a more acute critical condition, use of a self-selected gait speed, and/or the logistics of managing lines and tubes, as well as the number of support personnel required to ensure safety. Graham et al45 reported older adults who are acutely ill and hospitalized walk much more slowly than the previously published standards.
Patients were followed up by the physical therapist at a low frequency for strengthening exercise and patient education after transitioning to nursing-led ambulation. This did not interfere with their daily nursing-led ambulation. Collaborating with the multidisciplinary team improved patient mobility by identifying the specific roles between the nurses and physical therapists. This study shows, at the time of transition to nursing-led ambulation, the participants showed significant improvement in functional mobility following skilled physical therapy interventions. All the patients who were transitioned to nursing continued to ambulate successfully and without further reported adverse events. None of these patients were referred again to physical therapy service for mobility. To our knowledge, this is the first study that uses these specific functional outcome measures to transition ambulation from physical therapy to nursing services.
LIMITATIONSThis study has several limitations. First, this study was conducted in an academic hospital with highly trained staff, and it is unclear whether the findings would be generalizable to other institutions. Second, this study includes a relatively small sample size using sample of convenience. Nevertheless, according to Julious,46 a sample of 12 is a “minimum number of subjects per group in pilot studies.” Moreover, using the 95% confidence interval (CI) in cutoff scores to determine the relative stability of our cutoff scores,42 the AMPAC and gait speed have a narrow CI, while the Perme Score has a wide CI. Nevertheless, we believe that the proposed cutoff scores in our study are sufficient to justify our recommendations. Third, this study looked at a very specific patient population with sophisticated and invasive mechanical circulatory devices that may not be available to other nonacademic, tertiary medical centers. An ICU with a robust early mobility program with highly capable and trained nurses will be required for reproducibility of this study.
CLINICAL RELEVANCEThis study provides clinicians an objective guideline for when to transition ambulation to nursing staff using functional outcome measures. This type of information may help promote an overall culture of mobility in an acute care setting by identifying the responsibility of mobility to the appropriate multidisciplinary team member.
FUTURE STUDIESFurther research could explore whether functional differences in patients with IABP or Impella devices exist and to further distinguish potential cutoff scores for ambulation training. This study measured 3 common functional outcome measures frequently used at this institution, but future studies are needed to investigate the use of other measures to determine whether there is a stronger predictor of successful transition to nursing staff. We did not compare the effectiveness of one outcome measure versus another. Additional studies are required to determine the reproducibility of these results at multiple centers. Lastly, a bigger sample size can be used for future feasibility study.
CONCLUSIONThis study demonstrates the efficacy of using cutoff scores for commonly used outcome measures in the ICU setting to safely transition responsibility for patient mobility to nursing staff.
REFERENCES 1. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e876-e894. doi:10.1161/CIR.0000000000001062. 2. Macauley K. Physical therapy management of two patients with stage D heart failure in the cardiac medical intensive care unit. Cardiopulm Phys Ther J. 2012;23(3):37-45. 3. Mullan CW, Chouairi F, Sen S, et al. Changes in use of left ventricular assist devices as bridge to transplantation with new heart allocation policy. JACC Heart Fail. 2021;9(6):420-429. doi:10.1016/j.jchf.2021.01.010. 4. Peura JL, Colvin-Adams M, Francis GS, et al. Recommendations for the use of mechanical circulatory support: device strategies and patient selection: a scientific statement from the American Heart Association. Circulation. 2012;126(22):2648-2667. doi:10.1161/CIR.0b013e3182769a54. 5. Shah M, Patnaik S, Patel B, et al. Trends in mechanical circulatory support use and hospital mortality among patients with acute myocardial infarction and non-infarction related cardiogenic shock in the United States. Clin Res Cardiol. 2018;107(4):287-303. doi:10.1007/s00392-017-1182-2. 6. Rey F, Giraud R, Bendjelid K. Intra-aortic balloon pump and ischemic cardiogenic shock may still be a valuable association. J Clin Med. 2021;10(4):778. doi:10.3390/jcm10040778. 7. Naqvi SY, Salama IG, Yoruk A, Chen L. Ambulatory intra aortic balloon pump in advanced heart failure. Card Fail Rev. 2018;4(1):43-45. doi:10.15420/cfr.2018:22:1. 8. Ramsey SC, Lucas J, Barrett P, Ballard WL, Kaul P, Klein AJ. Safe ambulation of critically ill cardiac patients with femoral balloon pumps: a case cohort study. J Card Fail. 2020;26(7):621-625. doi:10.1016/j.cardfail.2020.05.010. 9. Berg HE, Dudley GA, Häggmark T, Ohlsén H, Tesch PA. Effects of lower limb unloading on skeletal muscle mass and function in humans. J Appl Physiol. 1991; 70(4):1882-1885. doi:10.1152/jappl.1991.70.4.1882. 10. Hather BM, Adams GR, Tesch PA, et al. Skeletal muscle responses to lower limb suspension in humans. J Appl Physiol (1985). 1992;72(4):1493-1498. doi:10.1152/jappl.1992.72.4.1493. 11. Dudley GA, Duvoisin MR, Convertino VA, Buchanan P. Alterations of the in vivo torque-velocity relationship of human skeletal muscle following 30 days exposure to simulated microgravity. Aviat Space Environ Med. 1989;60(7):659-663. 12. Shoemaker MJ, Dias KJ, Lefebvre KM, Heick JD, Collins SM. Physical therapist clinical practice guideline for the management of individuals with heart failure. Phys Ther. 2020;100(1):14-43. doi:10.1093/ptj/pzz127. 13. Lewinter C, Doherty P, Gale CP, et al. Exercise-based cardiac rehabilitation in patients with heart failure: a meta-analysis of randomised controlled trials between 1999 and 2013. Eur J Prev Cardiol. 2015;22(12):1504-1512. doi:10.1177/2047487314559853. 14. Fisher S, Smart NA, Pearson MJ. Resistance training in heart failure patients: a systematic review and meta-analysis. Heart Fail Rev. 2022;27(5):1665-1682. doi:10.1007/s10741-021-10169-8.
Comments (0)