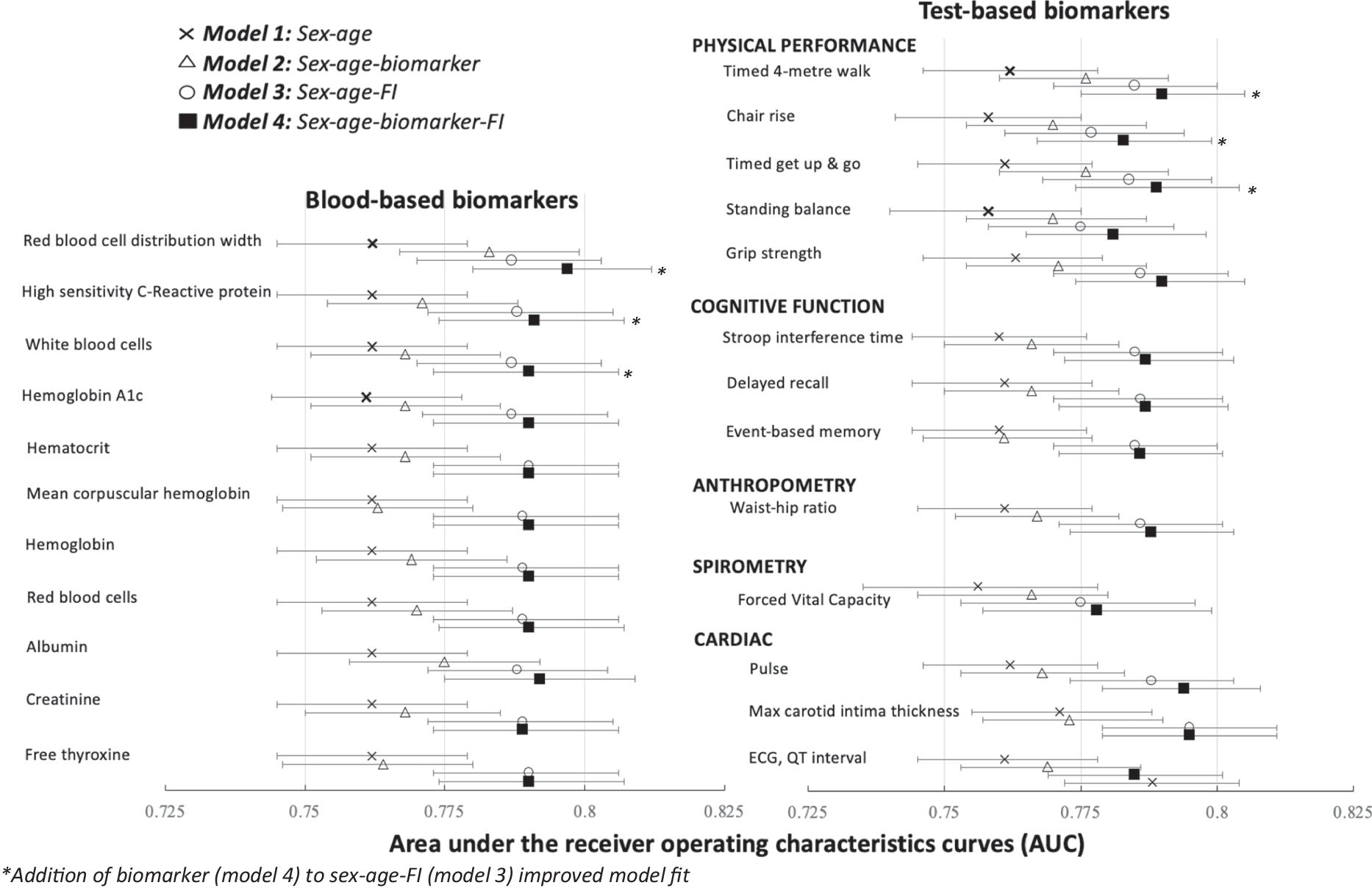
In a large cohort of nearly 30,000 individuals aged 45 + , we demonstrated that no single biomarker provided sufficient discriminative capacity in predicting mortality. Conversely, FI scores combining biomarkers demonstrated better mortality risk prediction when compared to all 70 individual biomarkers. There was some evidence to suggest that certain biomarkers (walking speed, chair rise, time up and go, pulse, red blood cell distribution width, high-sensitivity C-reactive protein, and white blood cells) can improve prognostic accuracy when considered in addition to frailty, yet on their own, they had poorer predictive validity than the comprehensive FI score. These findings reaffirm that measuring a single biomarker is an insufficient screening tool, further supporting the need for more automated and holistic FI assessment in clinical settings.
No biomarker predicted better mortality by itself when compared to the whole FI. However, the identification of seven biomarkers that improved the accuracy of the models requires further consideration, given their close relationship to aging. First, it is unsurprising that half of the physical performance tests added value to the predictive model, given these have been shown repeatedly to predict mortality [25]. Physical performance and pulse are the result of a complex interaction between bodily systems, which thus may be indicative of damage across cellular, organ, and multi-system levels. Aging has been shown to decrease this complexity, which therefore may eventually lead to adverse outcomes [26]. Each of the three blood-based markers (red blood cell distribution width, high-sensitivity C-reactive protein, and white blood cells) may suggest distinct mechanisms in the aging process, which may explain their utility in a prediction model. For example, C-reactive protein is a well-known inflammatory marker related to aging and adverse outcomes and is involved in immunosenescence and inflammaging [27]. Regarding red blood cell distribution width, a recent study showed that the hemoglobin to red blood cell distribution width ratio is associated with frailty [28]. Moreover, it is also associated with cognitive impairment, even in patients without anemia [29], suggesting multiple pathways through which it can affect the aging process. Finally, although white blood cell count is variable from day to day, it may be indicative of consistent acute infections, chronic stresses, or toxic exposures (i.e., smoking, obesity) [30] that can increase mortality risk. It is noteworthy that only overall white blood cell count, and not specific type (i.e., granulocytes, lymphocytes, monocytes), improved prognostic accuracy.
The clinical meaningfulness of the AUC differences warrants discussion. In health care settings, many clinicians strive to gather as much information as possible from the patient. Having a composite measure of frailty, such as the FI, allows clinicians to focus interventions on the whole individual, moving away from the reductionist focus that a sole biomarker would provide. For example, if C-reactive protein was the only available marker, clinical suspicion could orient the assessment and the subsequent intervention to target inflammatory disorders or cardiovascular stress. This approach would fail to acknowledge that the patient could benefit more from other interventions (e.g., exercise) and, instead, orient treatment to intervene on the single abnormal biomarker. Many of the deficits included are already routinely collected in clinical settings (e.g., pulse, vision, blood tests) or can be derived from self-report questionnaires; therefore, it is feasible to implement our findings into clinical care. Given the non-invasive nature of FI data collection, the statistically significant improvements in AUC (e.g., 0.02–0.04) are likely to provide a clinical net benefit, particularly considering the population level benefits if frailty assessments become a part of routine data collection across all clinical settings [31, 32].
Key strengths of this study include the large sample size, objective ascertainment of 70 individual biomarkers, and comprehensive triangulation of mortality status using three methods. Limitations include the lack of availability of exact date of death, missing blood samples in ~ 10% of sample, and exclusion criteria of CLSA (those with cognitive impairment, full-time members of Canadian Armed Forces, those in long-term care institutions, and those living on reserves/other aboriginal settlements). Future research should replicate these analyses while examining other adverse health outcomes including biomarker-specific disease outcomes (e.g., mobility/disability for physical performance biomarkers or cardiovascular-related outcomes for cardiac biomarkers). In conclusion, our findings provide strong support for the continual implementation of routine frailty assessment combining biomarkers in health care settings and advocate caution against trying to capture frailty and mortality risk using a single biomarker.

留言 (0)