TME is an integral part of LUAD and rich in inflammatory signaling, which attracts various immune cell populations (Allavena et al. 2011; Pitt et al. 2016; Spella and Stathopoulos 2021). Among them, tumor-reactive lymphocytes, tumor-associated macrophages (TAMs), tumor-associated neutrophils, myeloid-derived suppressor cells, and mast cells can interact with the tumor cells to ultimately shape a highly immunosuppressive TME, with enhanced tumor-promoting manifestations and diminished tumor cytotoxicity (Bronte et al. 2006; Ostrand-Rosenberg et al. 2012; Zaynagetdinov et al. 2011). Meanwhile, the efficacy of cancer immunotherapy in NSCLC is hampered by intra-tumor heterogeneity for neoantigens, neoantigen loss, immunosuppressive TME secondary to tumor aneuploidy, and immune checkpoints such as PD-L1 and TIM-3 (Anichini et al. 2018; Anichini et al. 2020; Koyama et al. 2016; Rosenthal et al. 2019). The transformation of immune response from the anti-tumor state to the tumor tolerance state is conducive to the development and progress of LUAD. Some molecular subsets show specific mechanisms for promoting immunotherapy resistance due to genetic alterations in NSCLC (Dong et al. 2017). Immune-related genes and immune cells are considered as new therapeutic targets and prognostic biomarkers of LUAD.
The eRNAs regulate gene expression and are involved in cancer immunotherapy by providing additional explanatory power in predicting immune response (Chen and Liang 2020). The eRNAs regulate gene expression in two ways: one is that the early formed eRNAs can recruit protein complexes from their synthetic site for local activation; the other is that eRNAs can recruit remote or even other chromosome-related protein complexes to play a distal regulatory role (Chen and Liang 2020; Wang et al. 2011). Accumulating evidence showed that the eRNAs are important regulators in the immune response and associated with multiple tumorigenic signaling pathways, including immune checkpoints, p53, and PPARr (Guo et al. 2020; Melo et al. 2013; Zhang et al. 2019).
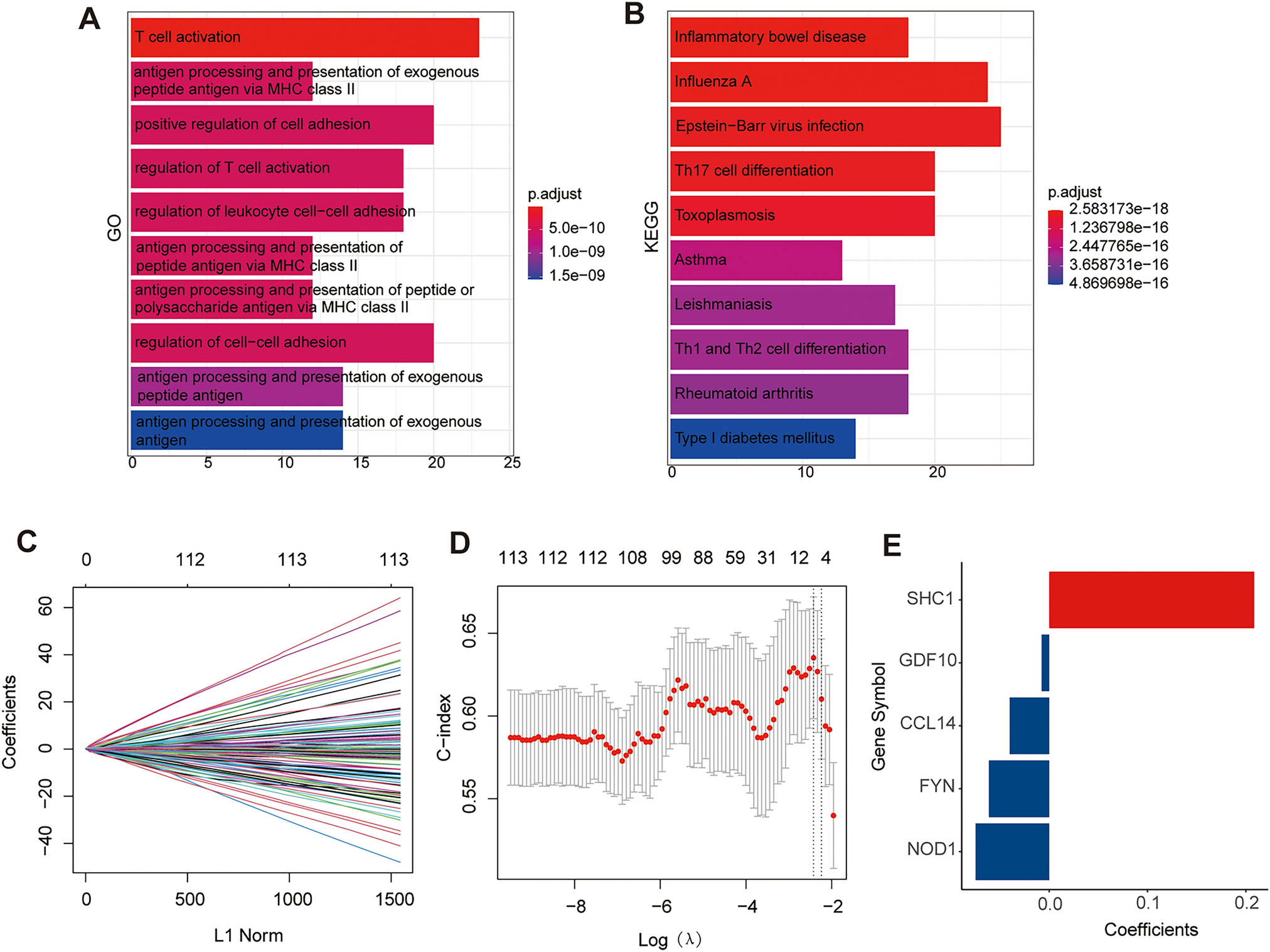
In our study, we identified five immune-related eRNA-driven genes (SHC1, CCL14, FYN, NOD1, and GDF10) to construct a new prognostic risk signature and validated its predictive capacity. Of the five genes, SHC1 expression correlated positively with poor survival. In contrast, CCL14, FYN, NOD1, and GDF10 acted as protective factors (Fig. 1E and Supplementary Fig. 1).
Furthermore, the risk signature had promising predictive capacity in diverse situations. The high-risk patients were significantly associated with the malignant features, including increased mortality, advanced stage, larger tumors, more lymph node metastases, distant metastasis, and poor survival outcome. Moreover, we also validated the capacity of this signature in two independent cohorts from the GEO database.
Among the signature genes identified in this study, SHC1 expression was significantly increased in patients with lung cancer, and its expression level and methylation level were associated with survival (Liang et al. 2021). In addition, SHC1 was also significantly associated with DNA methylation, m6A RNA methylation, tumor mutational burden (TMB), Mismatch repair proteins (MMRs), microsatellite instability (MSI), TAMs, tumor-associated immune cell infiltration, and immune checkpoints in cancers (Chen et al. 2022). Pan et al. showed that SHC1 was overexpressed in LUAD and interacted with EGFR to promote the metastasis of lung cancer cells. The complex of SHC1 and EGFR was the potential therapeutic target to restrain lung cancer metastasis (Yang et al. 2022).
CCL14 was considered to be a good prognostic biomarker in multiple cancer types and triggers the activation of monocytes, macrophages, and THP-1 cells through its binding affinity with CCR1, CCR3, and CCR5. Multiple studies suggest that CCL14 contributes to the development and advancement of different medical conditions, such as allergic airway inflammation and certain types of cancer (Gu et al. 2020; Wong et al. 2016; Zhu et al. 2019). However, the roles of CCL14 have not been described in LUAD.
As a TGFβ family member, GDF10 is highly expressed in the lung. Overexpressing GDF10 could attenuate tumor formation. Conversely, GDF10 expression silence reversed these effects (Upadhyay et al. 2011), and GDF10 is regarded as a tumor growth inhibitor and a silenced gene in lung cancers (Chen et al. 2023; Dai et al. 2004; Tandon et al. 2012).
As a non-receptor tyrosine kinase in the Src family of kinases, FYN plays important roles in the epithelial–mesenchymal transition (EMT) through regulating cell proliferation, morphology, apoptosis, and motor ability, which promotes tumorigenesis and progression, and is significantly associated with patients’ prognosis (Goel and Lukong 2016). FYN tyrosine kinase is a downstream target of receptor tyrosine kinases and modulates the immunotherapy response in the glioma (Comba et al. 2020). However, the role of FYN in LUAD has not been described.
Zhang et al. observed that NOD1 and NOD2 overexpression promote tumorigenicity and metastasis through the NOD1/2-NF-κb/ERK and IL-8 axis in human squamous cervical cancer (Zhang et al. 2022). However, Nod1 was also found to be an innate immune receptor and protects the intestine from inflammation-induced tumorigenesis (Chen et al. 2008). NOD1 absence was associated with tumor growth and cell proliferation induced by an increased sensitivity to estrogen in MCF-7 cells (Silva et al. 2006). However, the role of NOD1 required further study in LUAD.
We utilized GO and KEGG analyses to investigate the underlying molecular mechanism of the prognostic risk signature. Our findings indicate that this gene signature may play a critical role in regulating these tumor-related immune pathways. Additionally, recent research has shown that many types of LUAD are immunogenic and sponged in cancer-infiltrating lymph cells (Steven et al. 2016). Our team examined the relationship between the signature and immune infiltration in LUAD using the ssGSEA algorithm. Interestingly, we found that the risk signature was significantly associated with the Infiltration levels of various immunocytes, such as activated B cell, immature B cell, CD8 T cell, effector memory CD8 T cell, dendritic cell, central memory CD4 T cell, eosinophil, immature dendritic cell, macrophage, MDSCs, natural killer T cell, natural killer cell, regulatory T cell, type 1 T helper cell, and type 17 T helper cell. To further confirm the correlation between the risk signature and immune status, we used the ESTIMATE algorithm to obtain the immune/stromal/estimate scores and tumor purity in the TME and collected survival data to explore the effect of these scores on survival rates. The results revealed that high immune/stromal/estimate scores were associated with prolonged survival in LUAD patients, which is consistent with the result from the previous study (Xiang et al. 2021). The current immune checkpoint biomarkers have limited sensitivity and specificity, meaning that not all patients who are positive for the biomarker will respond to immunotherapy, and some patients who are negative for the biomarker may still respond. Our signature exhibited higher predictive power for the survival status of LUAD patients and response outcomes for immunotherapy and is a potential immune-oncogenic biomarker for prognosis, therapeutic drug selection, and follow-up.
In addition, through drug sensitivity prediction, we screened drugs with better sensitivity for patients in the high-risk scoring group from numerous clinical and preclinical chemotherapy and targeted drugs, such as the current clinical drugs lapatinib (a dual tyrosine kinase inhibitor that inhibits both EGFR and HER2), docetaxel, and paclitaxel, as well as candidate anti-cancer drugs BI-2536 (a known potent human polo-like kinase 1 inhibitor) and sepantronium bromide (a small molecule survivin inhibitor), and ULK1 (a ULK1 inhibitor). This result provides a basis for the development of new drugs and the selection of clinical medication and is expected to improve the poor prognosis of high-risk patients. Our signature suggests that high-risk patients may derive benefits from EGFR- tyrosine kinase inhibitors (TKIs) and ALK-TKIs, indicating a potential association between our risk scores and EGFR mutations or ALK fusions, which is an important. However, due to the limited proportion of samples with EGFR and ALK alterations in our study cohort, and the lack of clarity regarding the treatments used, a larger sample size is needed to explore the relationship between EGFR/ALK mutations and our risk model.
Above all, we used the data from the public database to identify five immune-related eRNA-driven genes, established a risk prediction model, and verified the signature in multiple datasets. The established signature can be used to predict the survival with high robustness and specificity and assist clinicians to make more beneficial decisions in LUAD. Moreover, specific eRNAs and target genes could be potential therapeutic targets for refractory tumors other than LUAD. In addition, our study provides a potential new predictive biomarker for the prognosis and survival of patients with LUAD and is expected to provide some possible options for improving immunotherapy. However, the effectiveness of risk score signatures needs to be further tested in a larger cohort of LUAD patients. More in vitro and in vivo experiments are needed to validate the biological functions and mechanisms of the genes related to the risk model in LUAD, which will help to better understand the role of these genes in disease development. The interactions between the genes in the risk model and other biological pathways and regulatory factors need further study to reveal more potential mechanisms of LUAD development and prognosis and provide more therapeutic targets. Furthermore, an LUAD cohort with a large sample size is required to further validate and confirm the predictive ability and reliability of our risk model in different clinical situations and independent cohorts.

留言 (0)