AL amyloidosis is a malignant disease characterized by abnormal plasma cell clone and amyloidogenic light chain deposition, causing hematologic and organ dysfunction. In recent years, MRD detection has been used to monitor patients with AL amyloidosis in the follow-up, and the value of MRD monitoring needs to be further analyzed and validated.
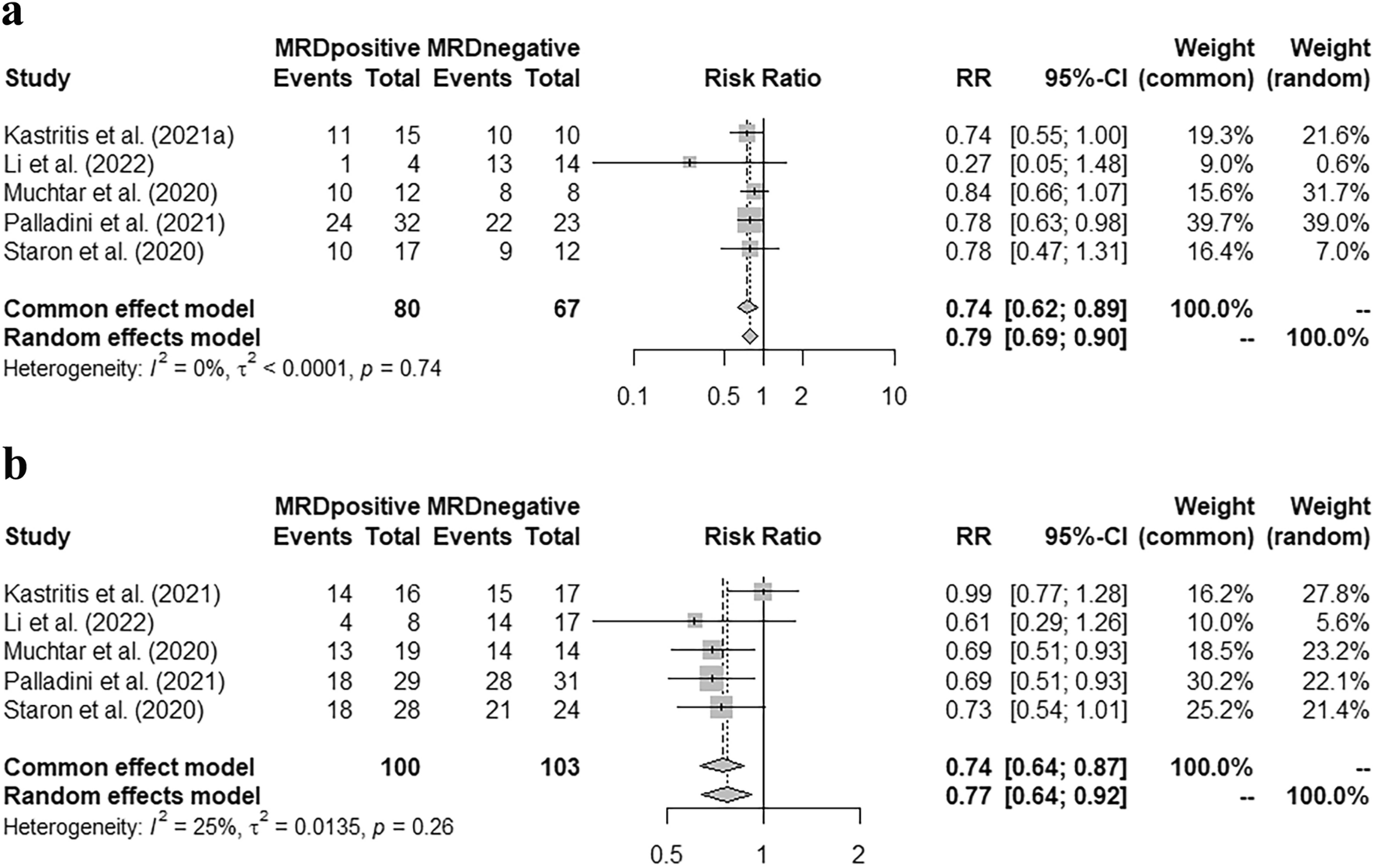
Our meta-analysis supported that once the patients achieved VGPR or CR, the recommended early therapy target, there was a statistical correlation between MRD status and the organ response rate, both in heart and kidney [pooled RR = 0.74 (95% CI 0.62–0.89), 0.74 (95% CI 0.64–0.87), respectively]. Previous studies have pointed out that, although some patients with AL amyloidosis achieved hematologic response after appropriate treatment, the recovery of organ function was not permitted and it might be due to the low level of clonal plasma cell burden (Staron et al. 2020; Szalat et al. 2021). Our study further supported that, a small burden of clonal plasma cells, with their continued production of monoclonal light chains, could still cause sustained organ damage and affect the patient's life quality. Therefore, our study highlighted the importance of reducing clonal plasma cell burden in the initial treatment.
In the studies we reviewed, Chakraborty et al. (2022) and Sidana et al. (2020) reported the organ response rate in negative MRD patients during the follow-up after MRD detection (May 2021 to 12/31/2021; 1 year after MRD detection, respectively). In the study of Chakraborty et al. (2022), the total cardiac or renal response rate in negative MRD patients did not improve during the follow-up after MRD detection; while the cardiac and renal ≥ VGPR rates increased by 16.7% and 4.4%, respectively. In addition, the total renal response rate in MRD negative patients increased by12% in Sidana et al. (2020). However, none of the two articles reported 100% organ response rate after MRD detection, which might be due to the short time-span of follow-up, or the irreversible organ damage caused by amyloid deposition. Therefore, more clinical studies with different time-span of follow-up are needed to evaluate the impact of MRD status on organ response after MRD detection, which may further validate the value of MRD status on therapeutic decision making.
The MRD status was also associated with the disease progression in the early follow-up. Our meta-analysis validated that patients with MRD-positivity had a higher risk of hematologic + organ progression in the first year after MRD detection [pooled RR = 12.57 (95% CI 1.73–91.04)]. Like other malignant diseases, the residual tumor cells can be the source of relapse and disease progression (Bertamini et al. 2021; Jongen-Lavrencic et al. 2018). Therefore, eliminating the residual clonal plasma cells as much as possible during induction and maintenance treatment, could reduce the risk of recurrence or progression.
In other hematological malignancies, such as multiple myeloma, the MRD status had been confirmed as a significant predictor in survival analysis, both in PFS and OS (Munshi et al. 2020). Our study supported the role of MRD negativity in predicting longer PFS [pooled HR = 0.27 (95% CI 0.17–0.45)]. As mentioned above, MRD-negative patients had a higher rate of organ response at the time of detection, and a lower risk of disease progression in the following 1 or 2 years; as a result, fewer patients deteriorated into organ malfunction in the early stage among the group with MRD negativity. Besides, smaller tumor burden was speculated in MRD-negative patients, according to those findings. Therefore, longer PFS was reasonable in this group of patients.
Although the MRD-negative group had a longer OS than the other, the difference was not statistically significant [pooled HR = 0.34 (95% CI 0.11–1.07)]. Our meta-analysis included the studies of Diaz-Pallares et al. (2020), Li et al. (2022) and Muchtar et al. (2020), which analyzed the impact of MRD status on the OS, but neither of them found a significant difference in the OS between the MRD-positive and -negative groups. The non-significance in OS may be due to the time span of follow-up. With the advancement of treatment regimens and the renewal of treatment methods, the median survival of AL amyloidosis has increased steadily in the past 40 years. The median survival of AL amyloidosis in 1980–1989, 1990–1999, 2000–2009, and 2010–2019 were 1.4, 2.6, 3.3, and 4.6 years, respectively (p < 0.001) (Staron et al. 2021). The use of autologous stem cell transplantation and proteasome inhibitors has improved the overall survival of AL amyloidosis (Huang et al. 2014; Kastritis et al. 2020). Besides, anti-CD 38 monoclonal antibody, such as Daratumumab, could further deepen the hematologic response and prolong survival free from major organ deterioration or hematologic progression (Kastritis et al. 2021b). Therefore, the difference in OS between various MRD statuses could get more significant when a longer follow-up span was set. Furthermore, since MRD status was associated with the response of impaired organs, the difference might be more significant in the subgroup with more serious organ dysfunction.
Our meta-analysis confirmed that MRD status in AL amyloidosis was related to organ response rate and the risk of disease relapse or progression. However, the depth of MRD detection may also affect the results of MRD status, thereby interfering with the accuracy of clinical decision-making. Multiparameter flow cytometry (MFC) is one of the most commonly used methods for MRD detection in AL amyloidosis. Quantification of bone marrow plasma cells using MFC in newly diagnosed AL amyloidosis could help predict patients’ prognosis (Paiva et al. 2011). The studies included in this meta-analysis used MFC for MRD detection with detection depths ranging from 2 × 10–6 to 1 × 10–4. In another study using matrix-assisted laser desorption/ionization-time-of-flight (TOF) mass spectrometry (MS) for detection of residual disease in AL amyloidosis, researchers found that even in patients who had achieved hematologic complete response and were negative for bone marrow flow cytometry, evidence of residual disease could still be found in 12% of the samples of the included patients; meanwhile, patients with positive residual disease had a higher risk of disease progression (at 50 months 75% vs. 13%, p = 0.003) (Dispenzieri et al. 2020). Therefore, a more suitable method or depth of MRD detection could guide the prediction of prognosis more accurately, and it is still an area that needs further research and exploration.
In recent years, the depth and accuracy of MRD detection have improved steadily with the advances in MRD technology. Our meta-analysis confirmed the clinical values of MRD detection in AL amyloidosis, and highlighted the importance of eliminating residual clonal plasma cells. However, some of the studies selected in our meta-analysis were retrospective, and the time span of follow-up might not be sufficiently long, so our results still require further confirmation by large-sized randomized clinical trials. With more advanced therapies and monitoring methods, patients with AL amyloidosis would meet better prognoses in the future.

留言 (0)