
記住我





Liver biopsy is essential for diagnosing many liver diseases, identifying the origin of metastasis, and working-up unknown causes of elevated liver chemistries. Percutaneous, transjugular, or laparoscopic liver biopsy has been the mainstay of diagnostic evaluation, with percutaneous being favored because it is cost-effective and least invasive. Endoscopic ultrasound (EUS)-guided biopsy has shown to be a new, effective method of sampling due to its high-resolution images, precision, and overall decrease in sampling variability.1,2 On review of 20 different EUS studies, there was adequate sampling with few adverse events, with a rare risk of bleeding being the primary concern.1,3 In a prospective, multicenter study, EUS liver biopsy demonstrated 1 event of bleeding (0.9%) in a patient with coagulopathy and thrombocytopenia among 110 patients without any other complications.4 There has been little to no literature on the infectious risks of EUS liver biopsy.
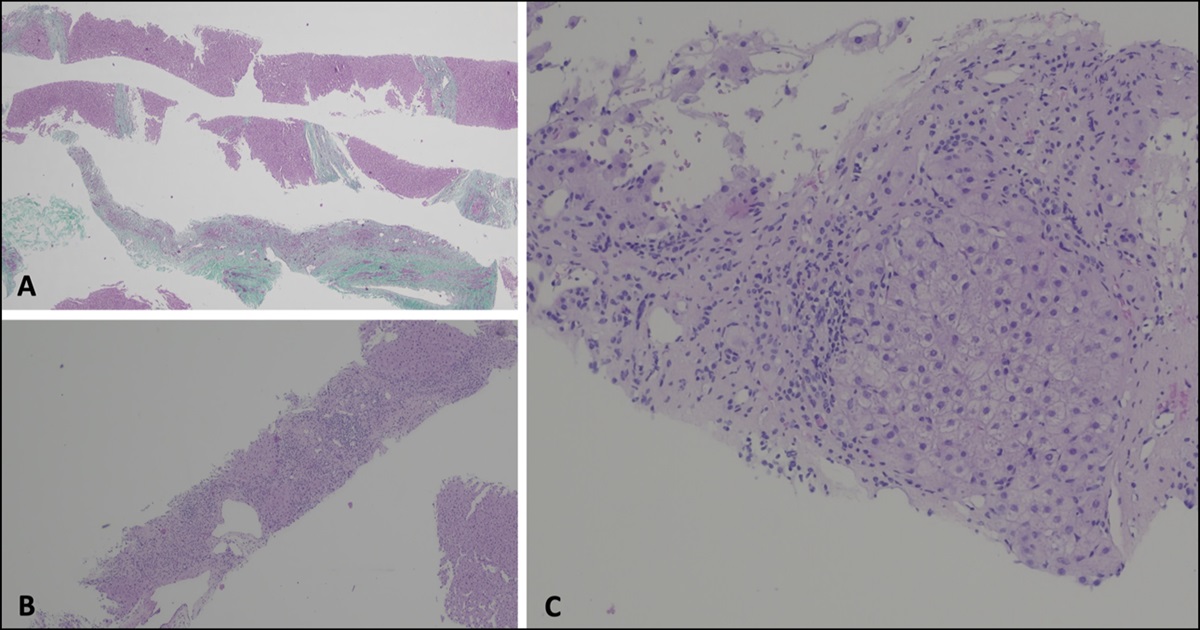
CASE REPORTA 64-year-old woman with a medical history of benign biliary stricture post Whipple procedure in 2004, intestinal hernia complicated by torsion resulting in ileostomy and reversal in 2017, and autoimmune hepatitis (AIH) on mercaptopurine was scheduled for an EUS-guided liver biopsy to confirm AIH remission. The decision for EUS biopsy was made for this patient because she preferred deeper sedation and was being evaluated for additional upper-gastrointestinal disorders. Liver biopsy was performed using a 19 g core needle and a “wet suction” technique with a heparin-flushed needle. Three passes were taken in the left lobe of the liver with good visualization; the right lobe of the liver was not well visualized on ultrasound (Figure 1). The results of the biopsy returned a week later confirming no active AIH. Her mercaptopurine was then discontinued.
 Figure 1.:
Figure 1.: Ultrasound image viewed endoscopically before biopsy.
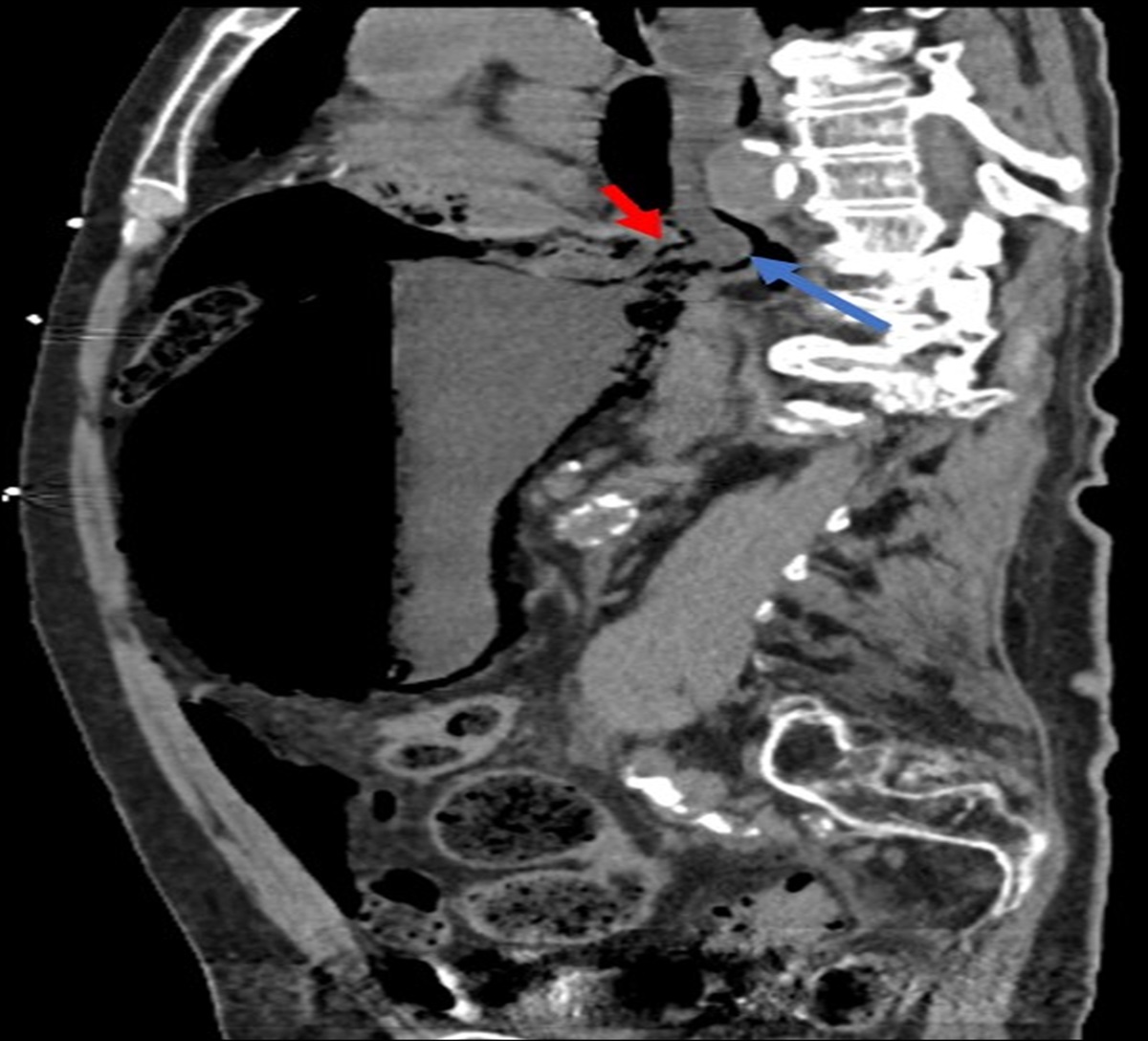
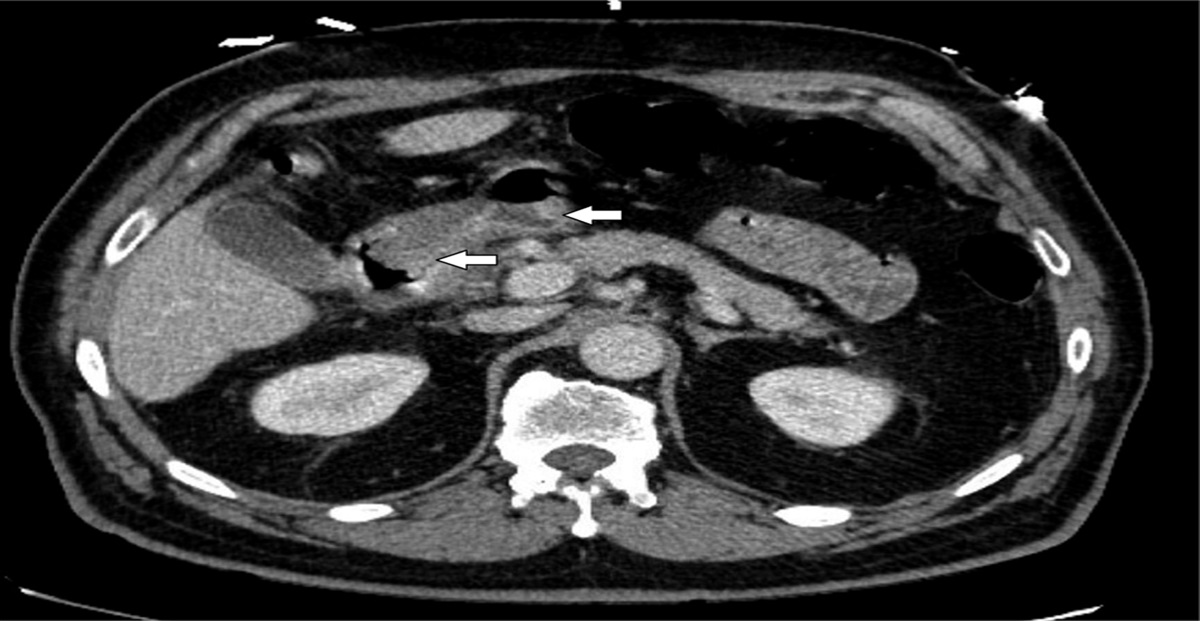
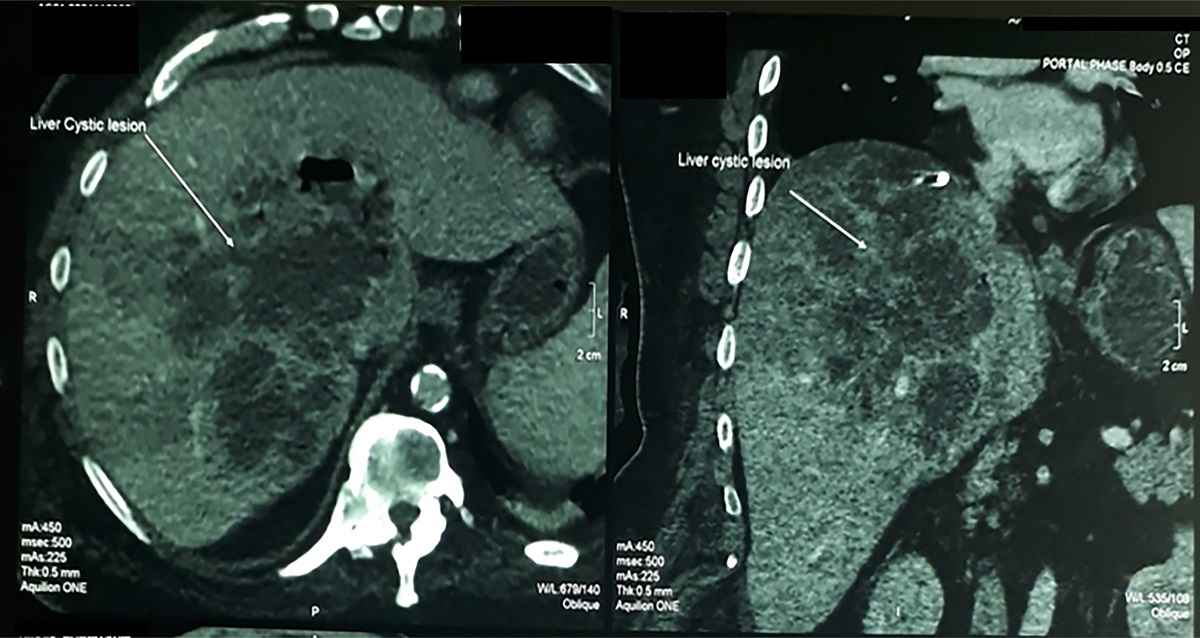
The patient presented approximately 1.5 weeks later to the emergency department reporting malaise, chills, and fever since the biopsy with right-sided flank pain, abdominal pain, and dyspnea. For these symptoms, she had been taking acetaminophen for pain relief but was unable to recall the dose. While in the emergency department, her vitals were stable, but her examination was notable for upper abdominal and costovertebral angle tenderness on the right side. Laboratory results were significant for a leukocytosis of 10.1, aspartate aminotransferase 75, and alanine aminotransferase 29, elevated from prior normal laboratory results. The patient had an abdominal and pelvic computed tomography that showed a cluster of new multiloculated cystic lesions in the hepatic segments II and III, measuring approximately 3.8 × 4.2 × 3.2 cm and a septic thrombosis/phlebitis in the branch of the left portal vein (Figures 2 and 3).
 Figure 2.:
Figure 2.: Multiloculated liver abscess viewed on abdominal computed tomography in the coronal plane.
 Figure 3.:
Figure 3.: Multiloculated liver abscess viewed on abdominal computed tomography in the transverse plane.
Hepatology and interventional radiology teams were urgently consulted. She was taken quickly for percutaneous abscess drainage with 40 cc of purulent fluid drained. She had blood cultures drawn and was empirically started on cefepime and metronidazole for infectious coverage. The patient was started on systemic anticoagulation with apixaban for her local thrombosis. The next day, a rapid response was called on the patient for hypotension. Vancomycin was empirically added to her antibiotic regimen, and she was given intravenous fluids. She required a brief stay in the intensive care unit for monitoring after stabilizing with fluid resuscitation and antibiotics alone, with eventual transfer back to the medicine floor. Infectious disease was consulted to assist in determining the duration and selection of antibiotics after her cultures from the abscess grew pan-sensitive Enterococcus coli. Ultimately, the patient was discharged home on 4 weeks of cefazolin and metronidazole.
DISCUSSIONInfection is a rare complication of any liver biopsy, whether percutaneous, transjugular, or EUS-guided, and therefore, periprocedural antibiotics are not routinely administered. There are several factors which may have increased this patient's risk for infection. First, this patient was immunocompromised on mercaptopurine making her more susceptible to infection, regardless of the biopsy method. She grew E. coli in her abscess cultures which is congruent with data showing that pyogenic liver abscesses are mostly polymicrobial, with E. coli and Klebsiella being the most frequently identified organisms associated with gut translocation.5 However, in one retrospective study in orthotopic liver transplant patients undergoing EUS-guided biopsy, there were no adverse events secondary to infection in this relatively immunocompromised population.6 This suggests that while the risk for infection may be logically higher in immunocompromised individuals, the risk of infection from EUS-guided biopsy remains very low.
In addition, this patient had biliary tract manipulation with the prior Whipple procedure. Patients with a history of surgery involving the biliary tract (including any form of biliary anastomosis) may have changes to bile flow, related either to relative stasis, if there are areas of narrowing, or enteric reflux in the biliary tract. Both mechanisms may increase the risk of biliary infections because anything that impairs bile flow may reduce the ability of the biliary system to clear bacterial contamination. One retrospective study of orthotopic liver transplant patients who received percutaneous liver biopsy showed that patients with biliary tract abnormalities were at higher risk for infection.7 This supports antibiotic prophylaxis before liver biopsy in immunocompromised patients with biliary tract abnormalities.
The advantages and disadvantages of EUS-guided vs percutaneous biopsy are an area of evolving debate and exploration, with several trials showing equal or improved tissue acquisition for EUS-guided liver biopsy vs percutaneous approaches.2–4 At our center, the decision between techniques is made on an individualized basis depending on availability, patient preference regarding anesthesia, and any additional needs for endoscopic evaluation (eg, combined esophagogastroduodenoscopy/EUS). EUS liver biopsy remains a preferred option for this and similar patients, given its high resolution and ability to obtain multiple core samples from different areas of the liver while avoiding important anatomic structures and without leading to postprocedural pain from biopsy sites, a frequent complaint after percutaneous liver biopsy.8,9 This case demonstrates that infection is possible with EUS biopsy. More research needs to be conducted on the risks of EUS biopsy and the patient populations it is best suited for, and whether selective periprocedural antibiotics should be a consideration in patients at higher risk for infection.
DISCLOSURESAuthor contributions: TD Andrade wrote the paper and edited final drafts. M. Awadalla edited the paper. S. Mahmood edited the paper and performed the case. TM Berzin edited the paper and was the attending physician supervising the case, and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Johnson KD, Laoveeravat P, Yee EU, Perisetti A, Thandassery RB, Tharian B. Endoscopic ultrasound guided liver biopsy: Recent evidence. World J Gastrointest Endosc. 2020;12(3):83–97. 2. Parekh PJ, Majithia R, Diehl DL, Baron TH. Endoscopic ultrasound-guided liver biopsy. Endosc Ultrasound. 2015;4(2):85–91. 3. Shah AR, Al-Hanayneh M, Chowdhry M, Bilal M, Singh S. Endoscopic ultrasound guided liver biopsy for parenchymal liver disease. World J Hepatol. 2019;11(4):335–43. 4. Diehl DL, Johal AS, Khara HS, et al. Endoscopic ultrasound-guided liver biopsy: A multicenter experience. Endosc Int Open. 2015;3(3):E210–E215. 5. Johannsen EC, Sifri CD, Madoff LC. Pyogenic liver abscesses. Infect Dis Clin North Am. 2000;14(3):547–63, vii. 6. Alsaiari AA, Mubarak MF, Therapondo G, et al. Endoscopic ultrasound-guided liver biopsy: A tertiary center experience. Gastrointest Endosc. 2018;87(6):AB211–212. 7. Larson AM, Chan GC, Wartelle CF, et al. Infection complicating percutaneous liver biopsy in liver transplant recipients. Hepatology. 1997;26(6):1406–9. 8. Nguyen P, Feng JC, Chang KJ. Endoscopic ultrasound (EUS) and EUS-guided fine-needle aspiration (FNA) of liver lesions. Gastrointest Endosc. 1999;50(3):357–61. 9. Procopet B, Bureau C, Métivier S, et al. Tolerance of liver biopsy in a tertiary care center: Comparison of the percutaneous and the transvenous route in 143 prospectively followed patients. Eur J Gastroenterol Hepatol. 2012;24(10):1209–13.
留言 (0)