
記住我



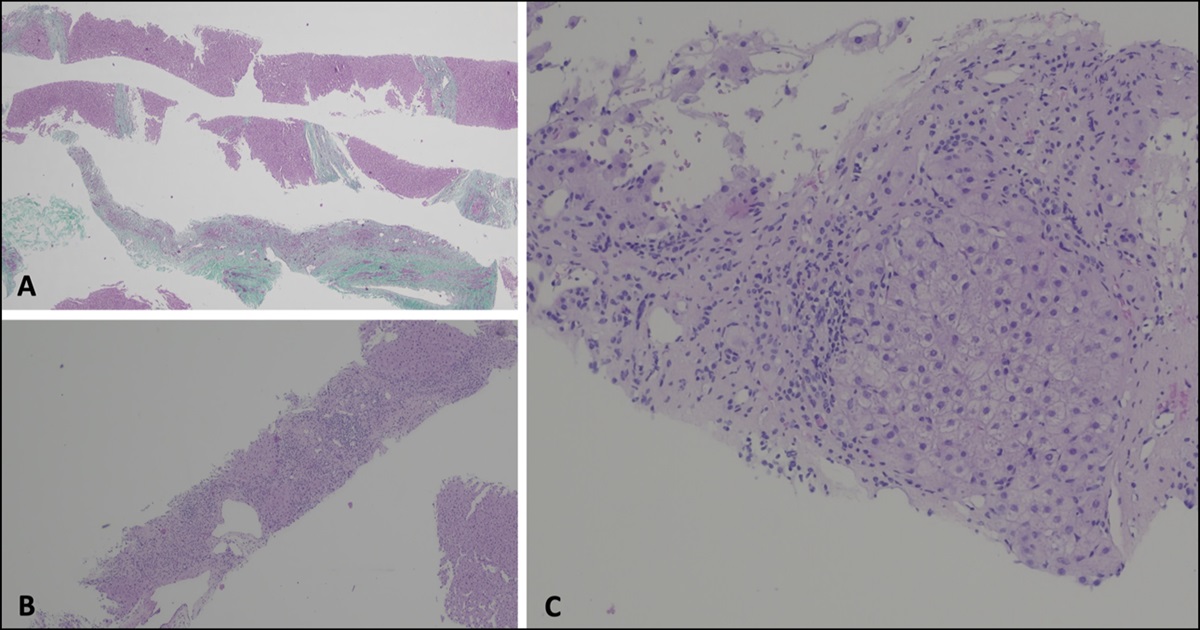


A 50-year-old man presented with acute onset of bloody diarrhea with mucous 3 days after thrombolysis for acute inferior wall myocardial infarction. The patient was empirically treated with antibiotics and antiamoebic agents. Patient's stool frequency persisted to be more than 10 per day with an increase in quantity of blood after 5 days of antibiotics and antiamoebic agents. The patient underwent flexible sigmoidoscopy which revealed circumferential ulcerations extending from rectum to beyond splenic flexure with active bleeding (Figure 1). Multiple biopsies were taken from the lesions which revealed ulcerated mucosa, few mucous glands distorted showing inflammatory exudate in lumen, submucosa showing diffuse and dense granulation tissue, and plasma cells, neutrophils, and mononuclear cells disrupting muscularis mucosae with no evidence of granuloma or malignancy or cytomegalovirus infection. A detailed drug history revealed that the patient had received 2 mg/h intravenous infusion of nicorandil for 2 days after while being treated for the acute myocardial infarction and was later converted to 5 mg every 12 hours of nicorandil tablet. The other drugs that the patient had received were enoxaparin, ranolazine, trimetazidine, aspirin, ticagrelor, rosuvastatin bisoprolol, rivaroxaban, telmisartan, and furosemide. The nicorandil was withheld, and the patient gradually improved. On follow-up, 20 days after the initial sigmoidoscopy, the patient's stool frequency had improved to one with no hematochezia over the previous 5 days.
 Figure 1DISCLOSURES
Figure 1DISCLOSURES
Author contributions: Author performed data collection, analysis, final drafting, and proof-reading of the final manuscript. V. Chaudhari is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
留言 (0)