
記住我





Pancreatic adenosquamous carcinoma (PASC) is an aggressive subtype of pancreatic adenocarcinoma that represents 1%–4% of exocrine malignancies according to autopsies and surgical specimen findings.1 The squamous component of PASC tends to proliferate faster than adenomatous tissue, leading to bleeding or necrotic tumor transformation, and prognosis is poor with a median survival of 8 months.1 The only potential treatment for cure of this aggressive tumor is surgical resection, although only 15%–20% meet the criteria for the surgery due to metastasis at the time of diagnosis.2 As squamous cells are absent in the normal pancreas, squamous metaplasia from ductal cells due to chronic pancreatic inflammation has been hypothesized as the pathophysiology of PASC, though still remains unclear. Other theories include histogenesis and a combination of different neoplastic cells, as well as the differentiation of multipotent primitive cells.3 As PASC is rare and progresses rapidly, diagnosis is made to be difficult. Typical initial symptoms of PASC are also very nonspecific, which includes weight loss, abdominal pain, and jaundice.3 Therefore, it is important to broaden the differentials for patients presenting with vague symptoms such as weight loss and gastric lesions to ensure that the diagnosis of PASC is not missed.
We report a case of PASC, presenting with unintentional weight loss and severe anemia in the setting of a gastric mass detected on endoscopy. Symptoms of PASC are broad, nonspecific, and indistinguishable from pancreatic adenocarcinoma. This case highlights and reminds physicians that pancreatic cancers can present with gastric invasion and thereby should remain on the differential diagnosis for gastric lesions.
CASE REPORTA 39-year-old Asian man with a history of chronic hepatitis B (positive anti-Hepatitis B e-antigen, positive Hepatitis B surface antigen, viral load 16.0 IU/L) presented with maroon stools and presyncope in the setting of a 40 lb unintentional weight loss over the previous year. He denied any history of abdominal pain, nausea, or vomiting. Physical examination demonstrated marked pallor, but no jaundice or scleral icterus. Laboratory investigations demonstrated an interval decrease in hemoglobin from 134 g/L the month prior to 47 g/L (reference range 137–180 g/L). Peripheral blood smear demonstrated microcytic anemia with hypoferritinemia suggestive of iron deficiency anemia. Blood work was otherwise significant for leukocytosis (20.0 × 109/L). CA19-9 was markedly elevated at 1,346 kU/L (reference range ≤35 kU/L).
Owing to suspicion for gastrointestinal bleeding, gastroenterology was consulted, and esophagogastroduodenoscopy demonstrated an ulcerated, friable, oozing mass measuring >3 cm in size on the lesser curve of the stomach, adjacent to a shallow ulcer (Figure 1).
 Figure 1
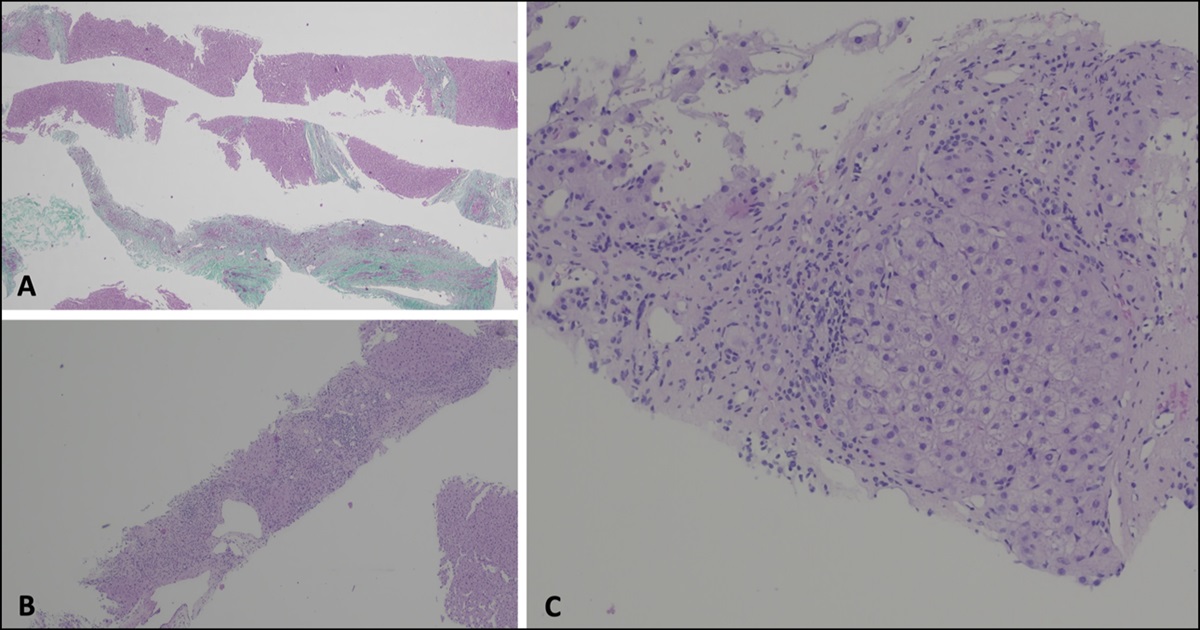
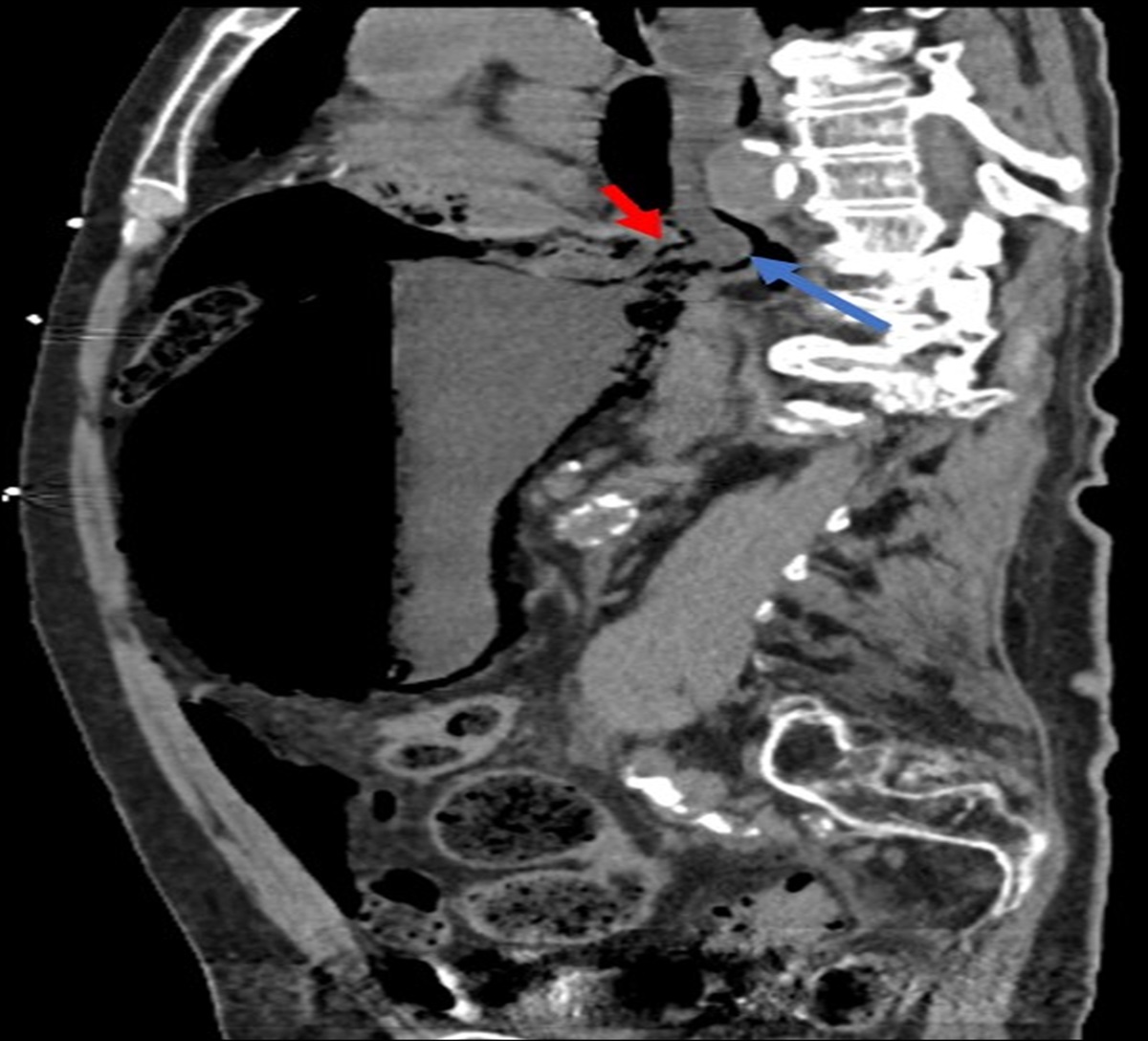
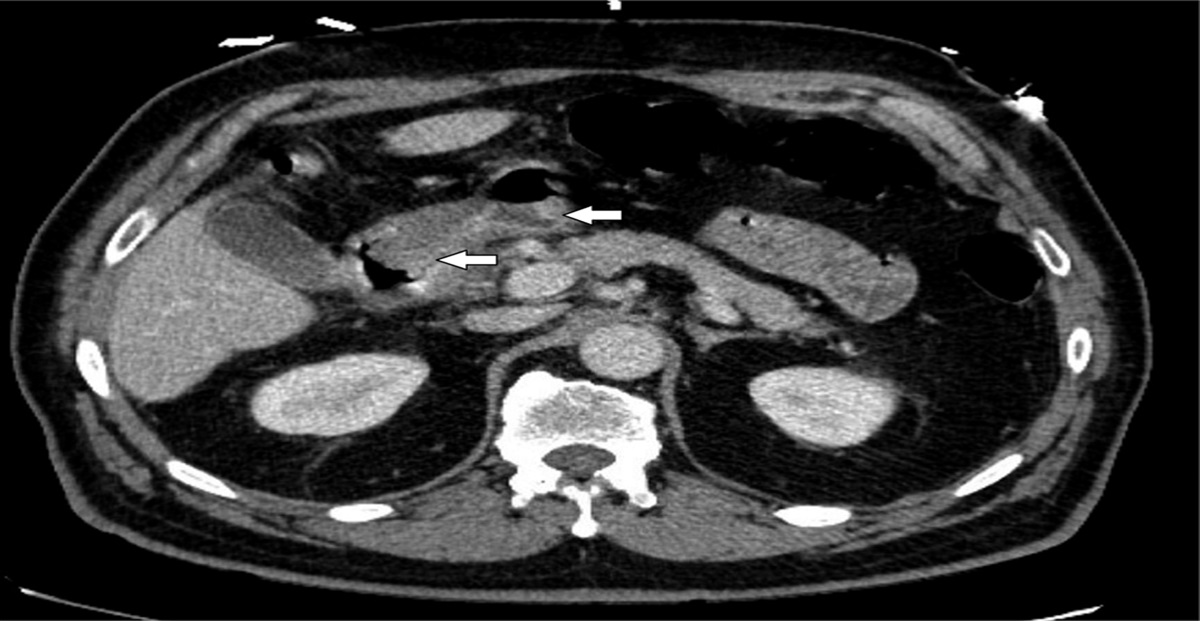
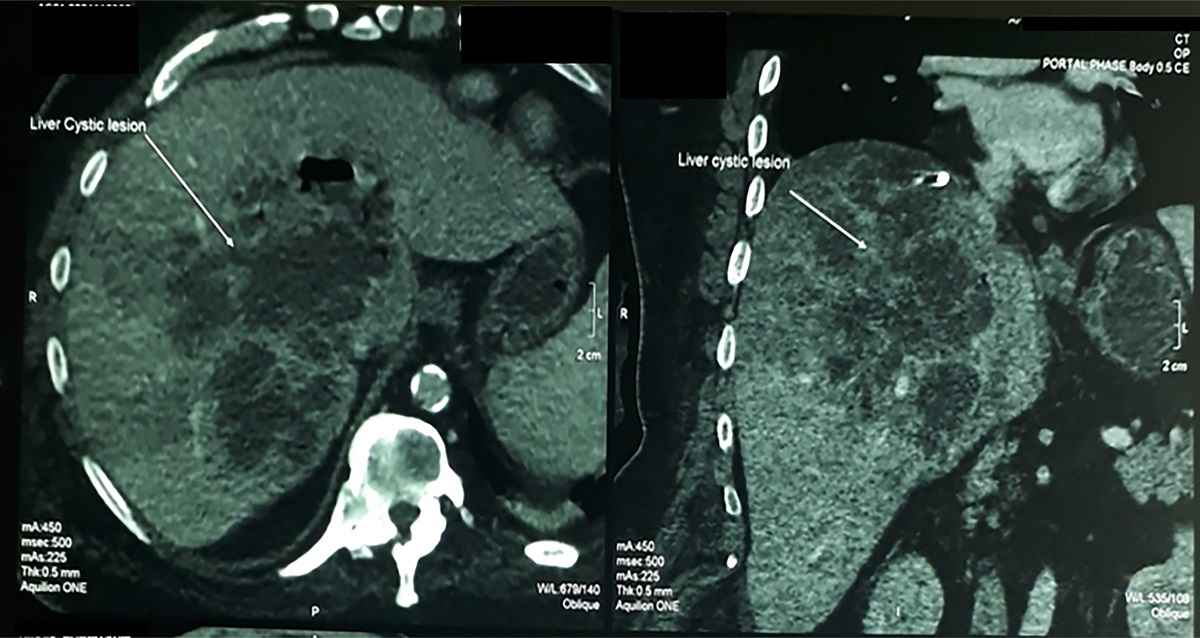
Figure 1Given the concern for malignancy, cross-sectional imaging was performed, and abdominal computed tomography (CT) demonstrated a large (10.7 × 6.7 cm) mass arising from the pancreatic tail invading the posterior wall of the gastric body into the gastric lumen and into the splenic hilum, encasing the splenic artery and occluding the splenic vein, with multiple hypodensities in the spleen and liver (Figure 2). Biopsies of the gastric mass subsequently demonstrated invasive moderately poorly differentiated carcinoma with mixed features of both squamous and adenocarcinoma growth patterns and positive lymphovascular invasion; biopsies of the adjacent ulcer demonstrated chronic Helicobacter pylori gastritis (Figure 3). The patient was diagnosed with metastatic adenosquamous carcinoma.
 Figure 2.:
Figure 2.: Computed tomography abdomen finding of large (10.7 cm x 6.7 cm) mass arising from pancreatic tail invading the posterior wall of gastric body.
 Figure 3
Figure 3Owing to the extent of disease, the tumor was deemed surgically unresectable. As the patient had an ongoing bleeding from the gastric mass, the patient underwent palliative radiotherapy (2,000 cGy/5 fractions) with stabilization of his hemoglobin and had no further bleeding. He initiated treatment with FOLFIRINOX chemotherapy. However, day 17 after cycle 3 of FOLFIRINOX, he developed abdominal pain and persistent fevers (T-max 38.8°C) and was found to have a marked leukocytosis (27.4 g/L). Repeat abdominal CT demonstrated a fistulization between the gastric mass and the spleen, as well as multiple perisplenic and splenic abscesses. Despite drainage and antibiotics, the patient died 3 months after diagnosis.
DISCUSSIONPancreatic cancer typically presents with vague symptoms such as abdominal pain, nausea, vomiting, and weight loss, but patients may less commonly present with bleeding and anemia from local or metastatic invasion of the gastrointestinal tract, with the incidence of gastric invasion being 0.2%–5.4%.4
While the presentation of PASC is indistinguishable from pancreatic adenocarcinoma, differentiating the 2 has important prognostic implications given the aggressive nature of PASC.5 Imaging tests such as CT and magnetic resonance imaging have been suggested to help differentiate the 2.5 PASC in the pancreatic tail have been reported to cause gastric wall invasion and splenic infarcts from splenic vein and artery encasement, as in our patient.1,6 By contrast, symptoms for when PASC is in the head of pancreas have been described as causing obstructive jaundice and pancreatitis.1 As demonstrated in our case, when gastric invasion is involved, a histopathologic diagnosis may additionally be made on endoscopic biopsies, which speaks to the importance of considering PASC when performing endoscopy on patients with nonspecific gastrointestinal symptoms.
Treatment options proven to be of benefit include radical surgery, chemotherapy, immunotherapy, and combination therapy with platinum-containing agents, with surgery being the only method of cure.7 The median survival for the surgical treatment option was shown by a study to depend on the type of resection: 14.4, 8, and 4.8 months for R0, R1 resection, and no surgical treatment, respectively.8 The efficacy of neoadjuvant and adjuvant chemotherapy as well as radiation therapy continues to be in question and explored through studies. Some studies demonstrated a significantly better survival rate with adjuvant platinum therapy for patients with PASC, whereas radiation therapy also showed benefit in overall survival but without statistical significance.9 Radiation therapy may have an additional role in treating PASC due to its hemostatic effect in gastrointestinal bleeding. A study has shown that radiation therapy in comparison with endoscopic treatment caused less recurrence and higher immediate efficacy in hemostasis in patients with GI bleeding due to gastric invasion of pancreatic cancer.10
Our patient had complete cessation of bleeding with palliative radiotherapy but unfortunately died of complications of the progressive disease. More knowledge on PASC including appropriate treatment strategies and different forms of clinical presentations is still needed to increase the rate of overall patient survival.
DISCLOSURESAuthor contributions: D. Kim was involved in drafting of the manuscript. T. Ogilvie was involved in acquisition of data and providing intellectual content. M. Woo was involved in study concept and design, supervising the project, and drafting the manuscript, and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Cedeno Kelly K, Moore C. Two rare cases of pancreatic adenosquamous carcinoma: A review of the literature with focus on radiologic findings. Radiol Case Rep. 2019;14(7):809–13. 2. Paramythiotis D, Kyriakidis F, Karlafti E, et al. Adenosquamous carcinoma of the pancreas: Two case reports and review of the literature. J Med Case Rep. 2022;16(1):395. 3. Del Arco H, Chakiba-Brugère C, Salabert L, Béchade D. Adenosquamous carcinoma of the pancreas. Clin Med Insights Oncol. 2019;13:1179554919886587. 4. Umezaki N, Hashimoto D, Nakagawa S, et al. Cystic gastric metastasis from pancreatic cancer. Surg Case Rep. 2018;4(1):31. 5. Toshima F, Inoue D, Yoshida K, et al. Adenosquamous carcinoma of pancreas: CT and MR imaging features in eight patients, with pathologic correlations and comparison with adenocarcinoma of pancreas. Abdom Radiol. 2016;41(3):508–20. 6. Takeuchi N, Emori K, Yoshitani M, Soneda J, Mohri K. Adenosquamous carcinoma of the pancreas that had penetrated into the stomach and transverse colon: A case report. J Med Cases. 2017;8(1):24–8. 7. Xiong Q, Zhang Z, Xu Y, Zhu Q. Pancreatic adenosquamous carcinoma: A rare pathological subtype of pancreatic cancer. J Clin Med. 2022;11(24):7401. 8. Smoot RL, Zhang L, Sebo TJ, Que FG. Adenosquamous carcinoma of the pancreas: A single-institution experience comparing resection and palliative care. J Am Coll Surg. 2008;207(3):368–70. 9. Borazanci E, Millis SZ, Korn R, et al. Adenosquamous carcinoma of the pancreas: Molecular characterization of 23 patients along with a literature review. World J Gastrointest Oncol. 2015;7(9):132–40. 10. Aguilera Munoz L, de Mestier L, Lamallem H, et al. Gastrointestinal bleeding in patients with pancreatic cancer: Causes and haemostatic treatments. United Eur Gastroenterol J. 2020;8(9):1106–14.
留言 (0)