Phosphoglyceride crystal deposition with suspected malignant ovarian tumor: a case report and literature review
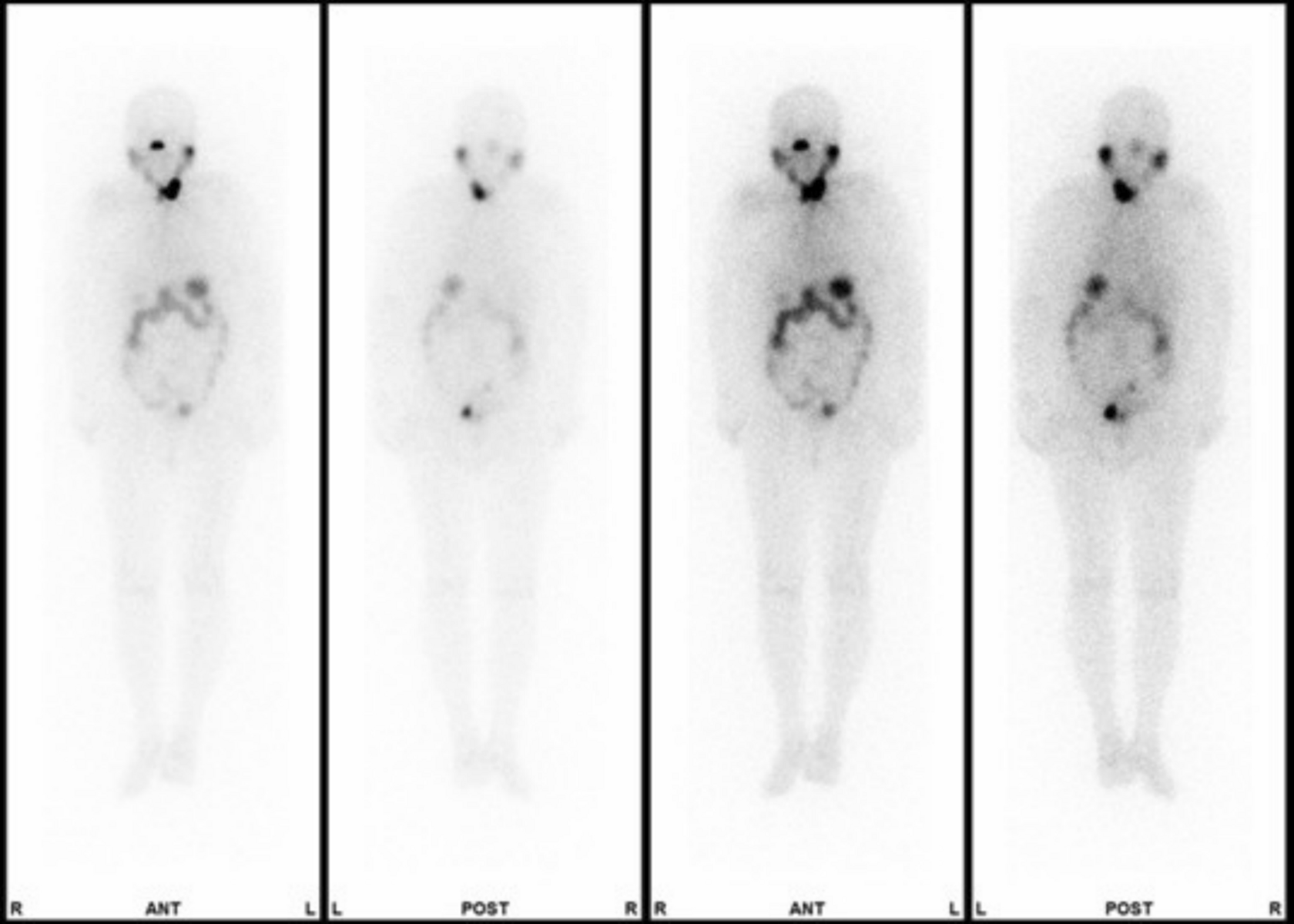
Phosphoglyceride crystal deposition disease is a rare condition occurring in soft tissues, resulting in scarring and affecting the bones, making preoperative differentiation from malignant tumors challenging. Here, we describe a case of phosphoglyceride crystal deposition disease initially suspected to be a malignant ovarian tumor before surgery. A 50-year-old woman with a history of three cesarean sections presented with lower abdominal pain. Transvaginal ultrasonography revealed a 54 × 58 mm tumor in the lower right abdomen. Pelvic contrast-enhanced magnetic resonance imaging showed a thickened cystic wall with diffusion restriction, a low signal intensity region on T1-weighted images, and a slightly high signal intensity region on T2-weighted images. The tumor markers, cancer antigen 125 and carbohydrate antigen 19–9 levels, were within normal ranges; however, positron emitting tomography-computed tomography revealed fluorodeoxyglucose accumulation (SUVmax 31.28) in the tumor wall. Suspecting a malignant ovarian tumor, a laparoscopy was performed to observe the abdominal cavity. A 10 cm white solid tumor was identified in the midline of the lower abdominal wall, leading to an open surgery recommendation. The tumor, adhering to the pubic bone, was excised. The tumor measured 9 × 7 cm, with the cut surface showing a yellow brownish solid periphery and central region with liquefied degeneration. Histologically, radial basophilic deposits, dense infiltration of macrophages, multinucleated giant cells, and foam-like tissue spheres were observed. The central region exhibited cholesterol clefts, fibrin exudation, and necrosis, leading to a diagnosis of phosphoglyceride crystal deposition disease. This disease is rare, occurring in patients with atypical fluorodeoxyglucose accumulation on positron emission tomography-computed tomography or with a history of tissue damage, such as abdominal surgery.






Comments (0)