
Remember me


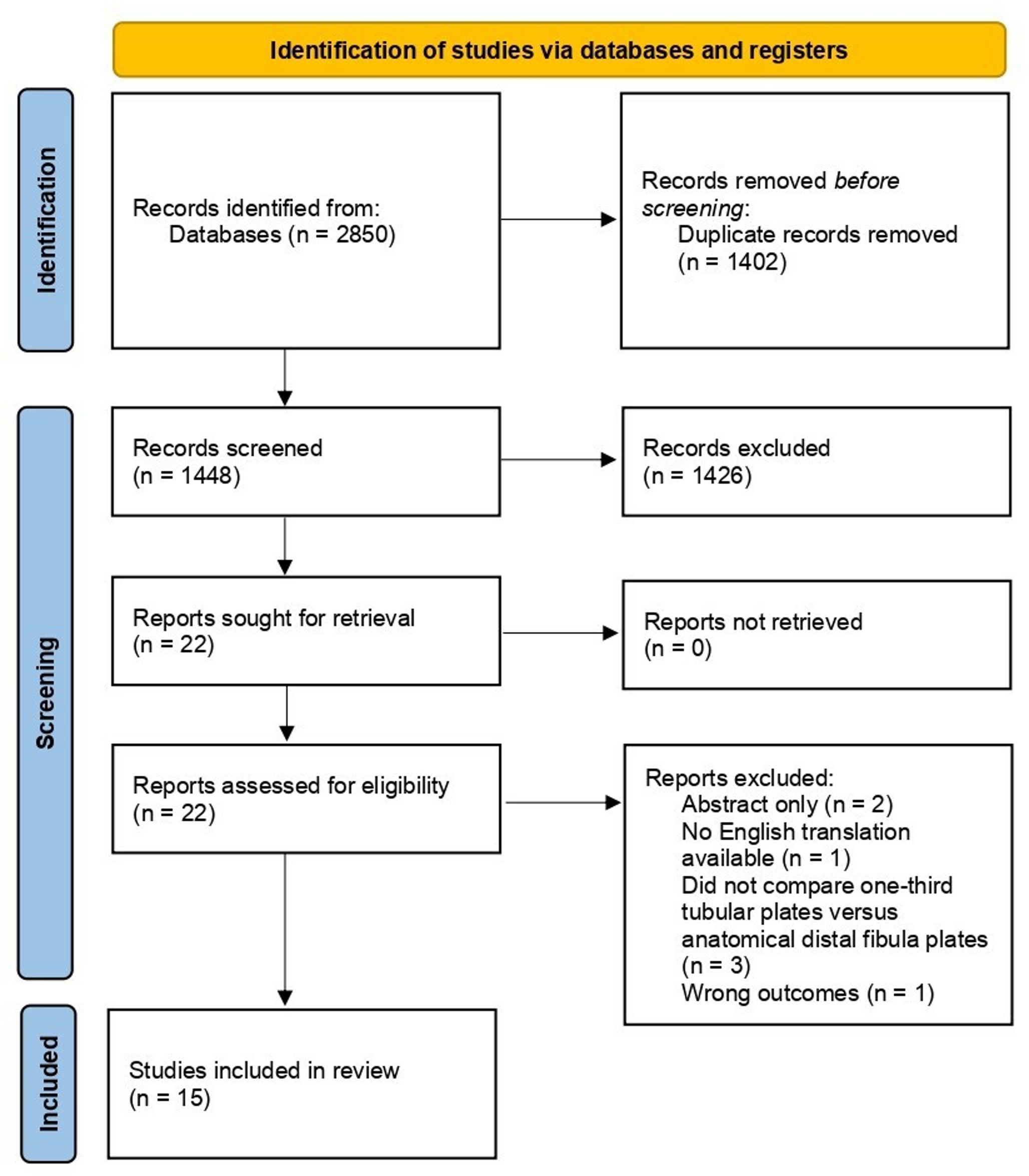

A retrospective analytical cross-sectional study was performed at Hospital Universitario del Valle in Cali, Colombia, including patients over 15 years of age who were admitted from January 2019 to December 2021 with diagnosis of civilian PBI due to firearms. The study was approved by the Health Research Ethics Committee of Universidad del Valle (Study: E034-022). The study was registered at http://openscienceframework.org (https://doi.org/10.17605/OSF.IO/SWG43). Patients with isolated PBI or associated with extracranial wounds without airway or hemodynamic instability and evaluated with CT and angio-CT in the first 24 h after admission, were included. Patients with penetrating extracranial injuries to the lung, heart, abdomen, or visceral organs that were hemodynamically unstable or required exploratory surgery, were excluded. Subjects who died in the emergency department or before arrival, or subjects with TBI without penetration of the bullet into the skull or with a tangential trajectory, were not included. Patients with technically inadequate tomographic studies (insufficient contrast, movement or metallic artifact that make it impossible to assess the image) or with multiple potential vectors due to fragmentation of the bullet were not included (Fig. 1).
Fig. 1
The primary outcomes include mortality and disability at 6 months. The Glasgow Outcome Scale (GOS) was used to evaluate patient´s mortality and disability at discharge and after 6 months. Secondary outcomes include clinical condition on admission, CT abnormalities, ballistics analysis, surgical treatment, length of stay and CT-angio vascular compromise.
CT datasetNon-enhanced head CT and CT brain angiography followed the Department of Radiology guidelines for head CT scanning. A Siemens tomograph with 128 RF was used for obtaining the images. Slices were aligned to the foramen magnum orientation with 1 mm in thickness. To compensate the 1 mm thickness of the slices, a 2 mm (1 mm) of inaccuracy for vertical structural measurements on CT scans was assumed [5, 6]. The vertical cuts were 0.6 mm of thickness in CT brain angiography and were made in a helical fashion in such a way that they were parallel to the plane of the orbitomeatal line for the exploration of the intracranial vessels after the administration of 80 milliliters of non-ionic intravenous contrast via infuser pump at 4 milliliters per second. The scan identifiers of each patient were anonymized.
Reconstruction path in 3D slicer of CT, CTA, and MRIThe reconstruction of the projectile trajectory was made with the use of the rendering-markups format and IGT modules in 3D Slicer software (version 5.0.2) (3D Slicer (www.slicer.org). First, we uploaded the DICOM files and rendered the CT Volume of the study using the rendering module, varying the shift transfer function until the skull was seen. Presets CT-AAA and CT-AA2 were used to achieve this goal. Once the skull was seen, the bullet entry point was identified and labeled as “I” and the exit or resting point as “O”. Then, using the markups module, two points were created and named “I” and “O”, with respect to the coordinate system located in the dorsum sellae. These two points were used as a reference to create a line that connects them using a script code in Python language (Python (www.python.org)). Once the trajectory was determined, the para-axial, para-sagittal, and para-coronal angles were calculated, which were used to create the trajectory planes using the Reformat module in 3D Slicer in which the track was observed. In addition, we use metal fragments, fractured bones, and subcutaneous distortion to help determine the projectile track.
The entry site was identified in CT by the pattern of beveling of the outer and inner table, also when the fragments of the bullet remained superficial in the extracranial soft tissues of the entry site. It also usually had a smaller area than exit wounds and had an irregular stellate fracture radiating from the point of impact. The inner table often had more comminution than the outer table at the site of impact and as opposed, the outer table may have more comminuted than the inner table at the exit site. Intracranial ricochet bullets were identified by a fracture of the inner table at the point of rebound. Therefore, a bullet inside brain parenchyma with evidence of a inner table fracture in proximity to the projectile is indicative of a ricochet trajectory. The reconstruction of the ricochet trajectory involved the connection of two linear vectors, one from the entry site to the rebound site and from this internal point of inflection to the exit or resting point. All the imaging signs of entry and exit sites were correlated with the clinical examination of the patients on admission and the clinical signs that were suggestive of the entry and exit points [1, 2].
It is important to define in this section the different types of trajectories the projectile could had in relation to the skull. A penetrating trajectory only had an entrance wound, remained inside the skull and without an exit wound. A perforating trajectory had both an entry and exit wounds and a ricochet trajectory had rebounded in the internal surface of the skull [1, 2].
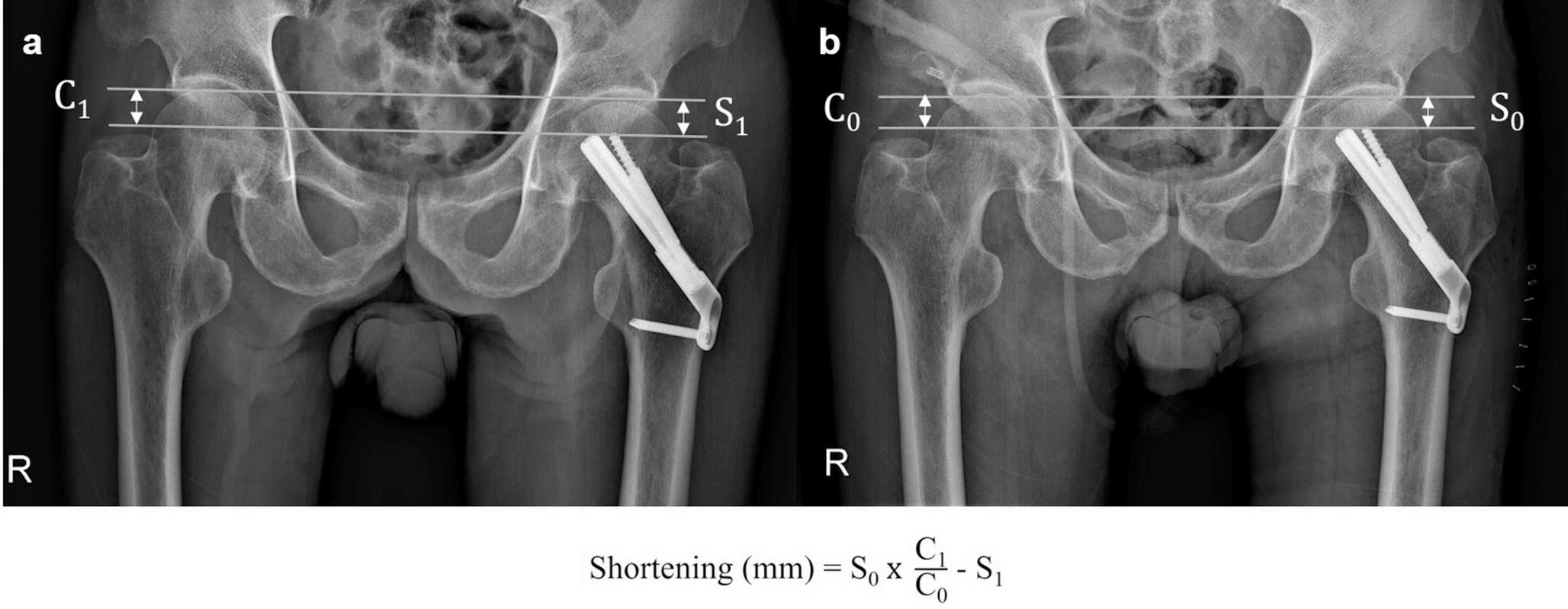
Image vector analysisThe selected images were measured in three Cartesian coordinate axes as follows: Xn: refers to the distance from the widest aspect of the outer left parietal bone cortex to the right parietal bone cortex of patient n (biparietal diameter) (Fig. 2a). Yn: was the distance from the external occipital protuberance to the glabella (glabella-occipital distance) (Fig. 2b). Zn: refers to the distance from the midpoint of the foramen magnum to the vertex (Fig. 2c). Using the IGT module, the midpoint of this Cartesian system (Point z = 0, y = 0, x = 0) was in the center of the superior part of the dorsum sellae (Fig. 2d and e). Vectors assessments were performed for all patients in non-enhanced CT and CT brain angiography.
Fig. 2
a. Biparietal measurement, Xn. b. Glabella-to-external occipital protuberance measurement Yn. c. The distance from the vertex to the center of the foramen magnum Zn. d. Sagittal view of the center of this cartesian system (Point x = 0, y = 0, z = 0). 2e. Coronal view of the center of this cartesian system (Point x = 0, y = 0, z = 0)
The measurements were extracted and their standard deviation was computed. The anthropomorphic variation was established in an error of 1 cm according to the description of Bergland et al. [7]. Each patient’s measurements were compared with those of the patient 0 in the 3D Slicer software.
Patient 0 (baseline patient) was selected from a list of 22 possible candidates. His head size includes the average measurements of the patient’s heads in this study in terms of mean and standard deviation. Additionally, the lack of midline shift and brain edema, made him an ideal candidate to be the standard brain and cranium for comparison. This patient was a 52-year-old man with a history of structural focal epilepsy who was admitted to the hospital due to focal-onset seizures with progression to bilateral tonic-clonic seizures. In the non-contrast brain magnetic resonance imaging (MRI) he presents small areas of gliosis in the right cerebellar hemisphere and both temporal lobes. The CT brain angiography was normal. There was no healthy control for MRI and CT brain angiography in our institution that fulfill the average measurements of the patients in this study in terms of mean and standard deviation. The patient in mention was selected because represent the best of our sample. The minor structural alterations did not affect de vector analysis for TBI patients. Patient 0 had a brain non-contrast MRI in which we plot the CT findings using Cartesian coordinates, where all patients CTs measurements were replotted for further analysis of potential zones associated with adverse or favorable outcomes.
When the dimensions of patient 0 were compared with the average Xn, Yn, and Zn coordinates (X mean 137.80 mm, Y mean 176.10 mm and Z mean 141.80 mm), the difference between previous measurements and X0 = 141.70 mm, Y0 = 180.30 mm Z0 = 140.00 mm were well within the standard deviation XSD: 5.62 mm,YSD:9.62 mm, and ZSD:5.88 mm.
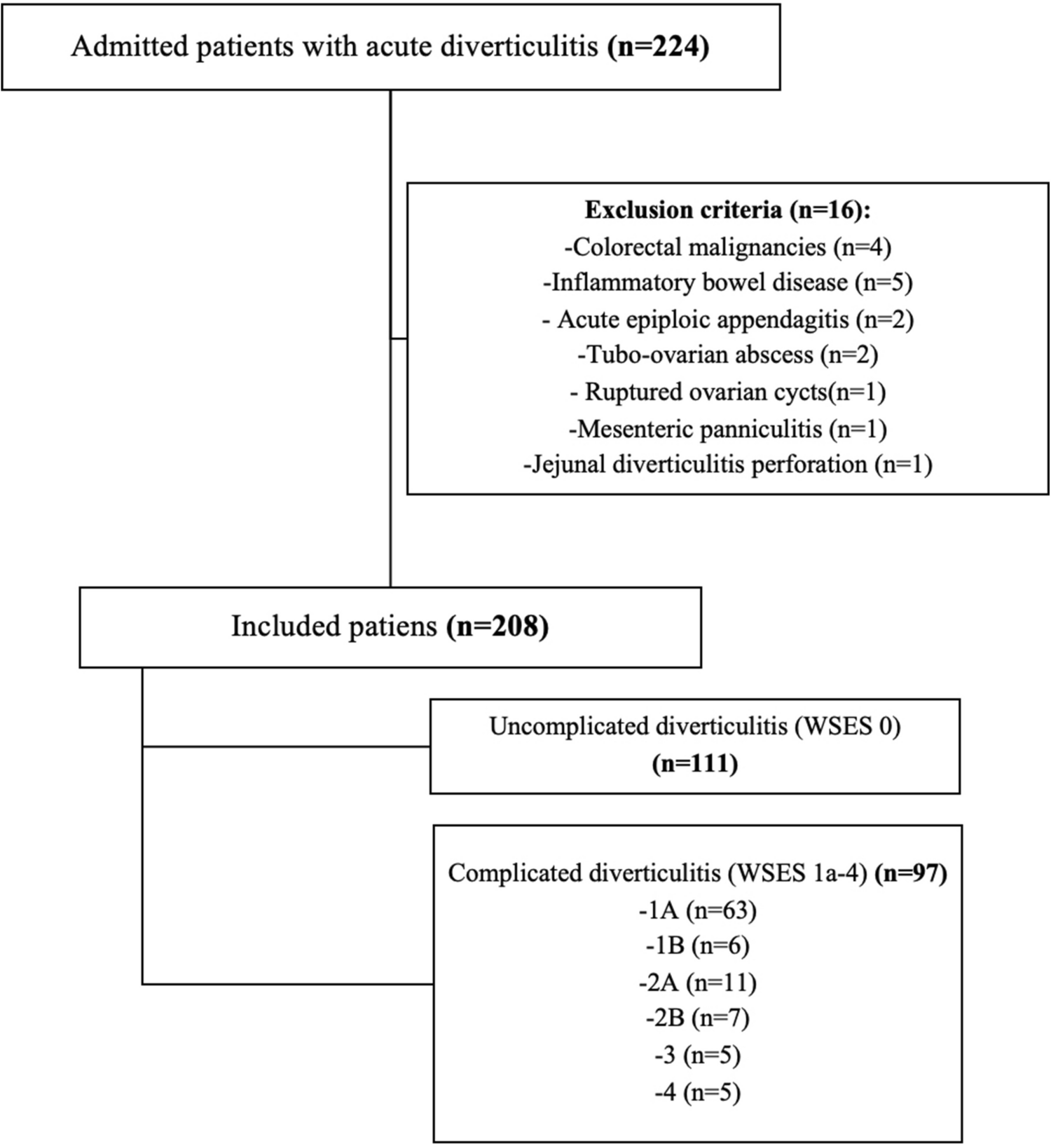
The measure of entry anglesThe angle measure was made after obtaining the trajectory and selecting the patient 0. All the trajectories were plotted with respect to this coordinate system on the dorsum sellae. Then, using the markups module, an axial, sagittal, and coronal plane was created with respect to the coordinate system to measure the angles using the following equation sinθ = bnbn in python script. The b is the vector director of each trajectory and n is the normal vector of each plane. These angles are very useful in multi-planar reconstruction (MPR) [8] because they provide the ability to reconstruct complex planes that match the plane in which the trajectory is seen best (Fig. 3).
Fig. 3
Comparison between the axial, sagittal and coronal views (classical views), regarding the para-axial, para-sagittal and para-coronal views of patient S4, a survivor, for determining resultant pathways in trajectories. a. Axial view. b. Sagittal view. c. Coronal view. d. Para-axial MPR showing trajectory 67.07° with respect P_Axi_RA (RA Axial plane), seems like the para-coronal plane. E. Para-sagittal CT MPR showing trajectory 22.8° toward the occipital bone, demonstrating the para-coronal orientation of the wound path. F. Para-coronal CT MPR showing trajectory 1.3° toward the patients Right, demonstrating the para-sagittal orientation of the wound path
Measures of distance to the circle of WillisFor each patient a measurement was made between the line of the trajectory and the closest node located in the circle of Willis. This measurement was made in each patient using the markups module and angio-CT, the coordinate system was placed in the dorsum sellae. All the measurements were taken and registered, and the median and standard deviation were calculated. The measurements were made using the formula D = APvv, where D is the perpendicular distance between a point P(X1,X1,X1) and a line with direction vector V(Vx, Vy, Vz). A is a point on the line.
Measures of the directional cosines of bullet trajectoriesA vector trajectory can be fully described by the point of entrance and exit, the length of the trajectory, and the “direction of cosines”. In the study methodology we use octans to group or classify the trajectories entry and directional cosines to describe the direction of the path. The direction of cosines are angles that were calculated with the next formulas: arc VxV, arc VyV and arc YzV. Vx, Vy and Vz are the components of the vector that defines the trajectory and V = Vx2 + Vy2 + Vz2, is the vector norm or the extent of the vector (length of the trajectory). These “direction cosines” are the angles between the vectors and each cartesian axes (X, Y, Z) and have the direction information of the trajectory. Using the Python iteration window in 3D Slicer, a script was created to calculate the “direction of cosines” in each trajectory.
Statistical analysisA descriptive analysis for each individual variable was conducted. We determined the proportions, central tendency, and dispersion measures. A bivariate analysis was made using the chi-square test and Fisher test to verify the strength of association between categorical variables considering a p < 0.05, taking mortality as the outcome variable. The analysis was performed in SPSS statistics software (IBM, Spain).
Comments (0)