2.1 Study Design
This was a retrospective, observational, single-center study to assess the effects of cenobamate on cognition in a real-world setting. The study was conducted in the Epilepsy Unit of Hospital Regional Universitario de Málaga, Spain. The study protocol was approved by the hospital’s ethics committee and was in accordance with the code of ethics set out in the 1964 Declaration of Helsinki and its later amendments.
Patients with drug-resistant FOS who received cenobamate within the Epilepsy Unit of Hospital Regional Universitario of Málaga between January 2022 and July 2022 as part of a Spanish EAP were retrospectively screened for inclusion in the study.
Inclusion criteria were: (1) age ≥ 18 years; (2) diagnosis of drug-resistant epilepsy (DRE) with FOS; (3) inclusion in the Spanish cenobamate EAP; (4) standardized cognition assessments prior to (i.e., baseline) and 6 months after the start of treatment; and (5) written informed consent from the patient or their legal representative. EAP authorization was limited to highly drug-resistant patients; patients with severe hepatic impairment, end-stage renal disease or nonfocal seizures were excluded from EAP authorization. Patients were excluded if they were unable to undergo neuropsychological evaluation due to intellectual, sensory, or motor deficits.
The first 20 patients who met the inclusion criteria were included in the study, and there were no exclusions during the study period.
2.2 Data Collection
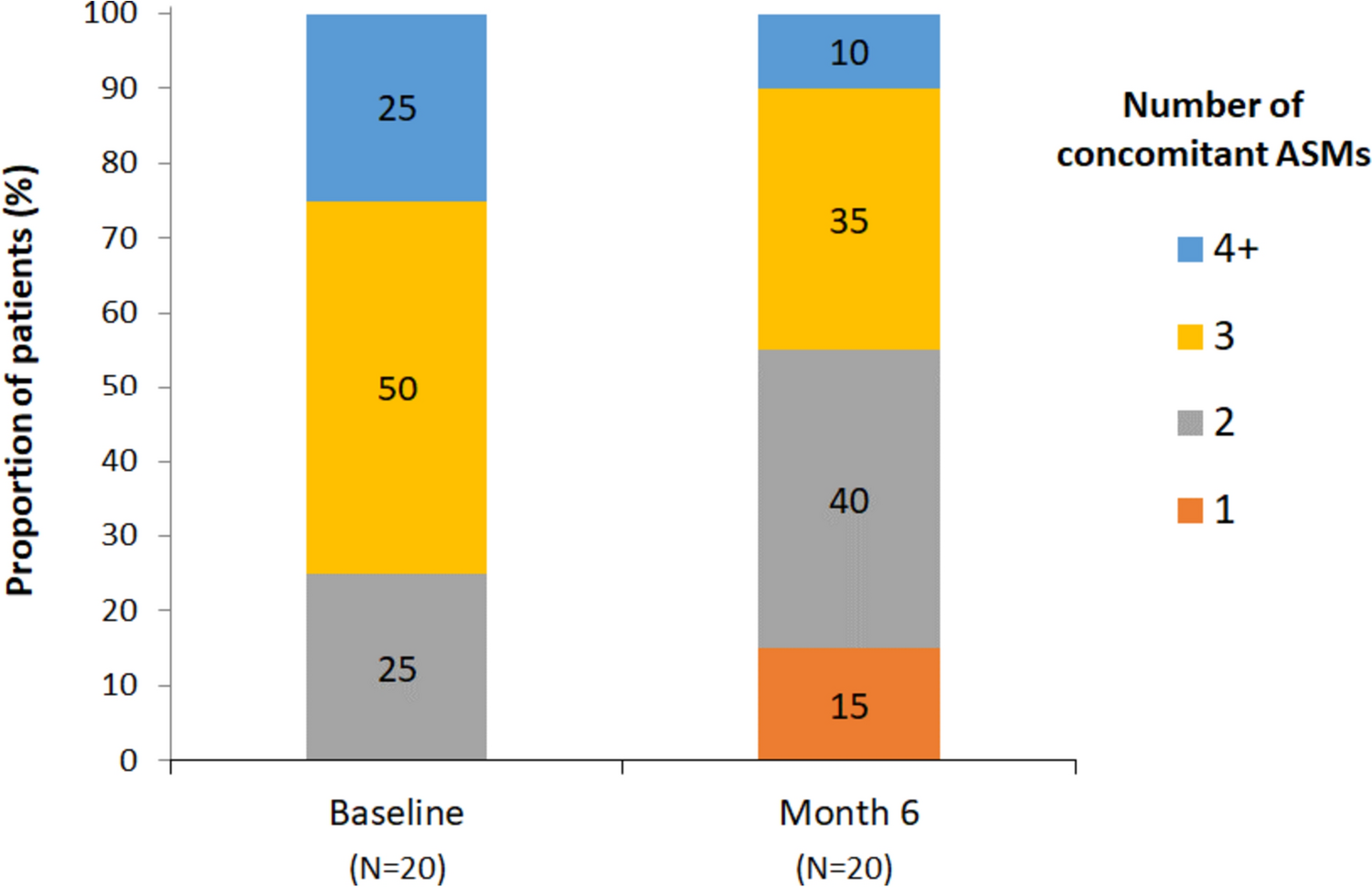
Data were collected from patients’ clinical records and stored according to usual clinical practice by participating physicians. The following data were collected at baseline: patient demographics, age at epilepsy onset, etiology, epileptogenic focus, baseline seizure frequency, prior epilepsy surgery, previous and concomitant ASM use, cenobamate dose, and cognition endpoints (see below). The following data were collected from clinical charts at 6 months: cenobamate dose, number of seizures, changes in concomitant ASM use, and cognition endpoints.
2.3 Cognition Tests
In all participants, a battery of 20 neuropsychological outcomes was used for cognitive evaluation at baseline and at 6 months. The time window between repeat neuropsychological assessments tests was at least 6 months, in line with ILAE guidelines which suggest a minimum of 6–9 months between tests to account for learning and repetition effects [16].
The Free and Cued Selective Reminding Test (FCSRT) [17] was used to evaluate verbal episodic memory and learning. Briefly, participants were shown a card containing four words and invited to recall the words freely, or if unsuccessful, following a cue. Three trials were conducted with a 20 s period of counting backwards between each. This procedure was repeated after a 30 min interval. Four outcomes were recorded: total free recall (TFR; sum of free recall), total recall (TR; sum of free recall + cued recall), delayed free recall (DFR; sum of delayed free recall), and delayed total recall (DTR; free delayed recall + cued delayed recall). Parallel tests were conducted to account for learning and repetition effects, as validated previously [18].
The Rey–Osterrieth Complex Figure Test (ROCFT) [17, 19] was used to evaluate visuospatial episodic memory, planning, and problem solving (executive functions). Briefly, participants were asked to reproduce a geometric figure to assess copying capacity and the time to completion was recorded. The picture was then removed, and participants were asked to reproduce the figure from memory. Participants were then distracted for 20 min and asked to repeat the figure again from memory. Copying capacity (ROCF-COP), memory (ROCF-MCP), and execution time (ROCF-T) were evaluated. Parallel tests were conducted to account for learning and repetition effects.
The Verbal Fluency Test and Executive Functions Verbal Fluency Test was used to evaluate verbal fluency, semantic memory, language, and executive function [20, 21]. Briefly, participants were asked to recite as many words as possible beginning with a “p” in 1 min (Fluency-Phonetics, FP). They were then asked to name as many animals as possible (Fluency-Semantics, FAN).
Frontal executive function was evaluated using INECO frontal screening (IFS), including a battery of subtests [22]: conflicting instructions; go–no go; backward digit span; verbal working memory (backward digit); spatial working memory (backward Corsi); proverb interpretation; and verbal inhibitory control (Hayling Test). This test battery obtains information on conceptualization, cognitive flexibility, motor programming, sensitivity to interference, verbal working memory, visual working memory, motor inhibitory control, and prehension behavior [22].
The forward and backward digit span test (WAIS-III) [23, 24] was used to evaluate working memory and attention. Briefly, participants were invited to repeat a series of numbers read out by an examiner, initially in the same order (DD) and then in reverse order (DI).
The Trail-Making Test (TMT) was used to assess attention, speed of visuomotor tracking, divided attention, mental flexibility, and motor function [24, 25]. Briefly, participants were invited to connect disordered numbers on a sheet of paper without lifting the pen from the paper (TMT-A). They were then invited to connect disordered letters and numbers alternately and in order as quickly as possible on a new sheet of paper (TMT-B).
The Five Digit Test was used to assess speed of processing, cognitive flexibility, sustained attention, automation, and inhibition [26, 27]. Briefly, participants were shown cards containing digits arranged in groups that were to be interpreted either from the value of the digit or their arrangement (e.g., five twos could be read as five or two depending on instructions from the examiner). Scores were divided into six categories (5A, alternate; 5C, counting; 5E, choice; 5F, flexibility; 5I, inhibition; 5L, reading).
For each test, reference values were derived from normative data from the Spanish NEURONORMA Project [17, 21, 24].
2.4 Statistical Analysis
Continuous variables were expressed as means (± standard deviation, SD) or medians (range) according to their distribution, and categorical variables as frequencies and percentages. The Student’s t-test was used to compare continuous variables between groups, as appropriate, and continuous related variables were analyzed using the Wilcoxon test. Reliable change indices were calculated as described by Brooks et al. [28] All statistical analyses were performed using IBM SPSS Statistics version 25.0. The threshold for statistical significance was 5% (p < 0.05).


留言 (0)