Study design
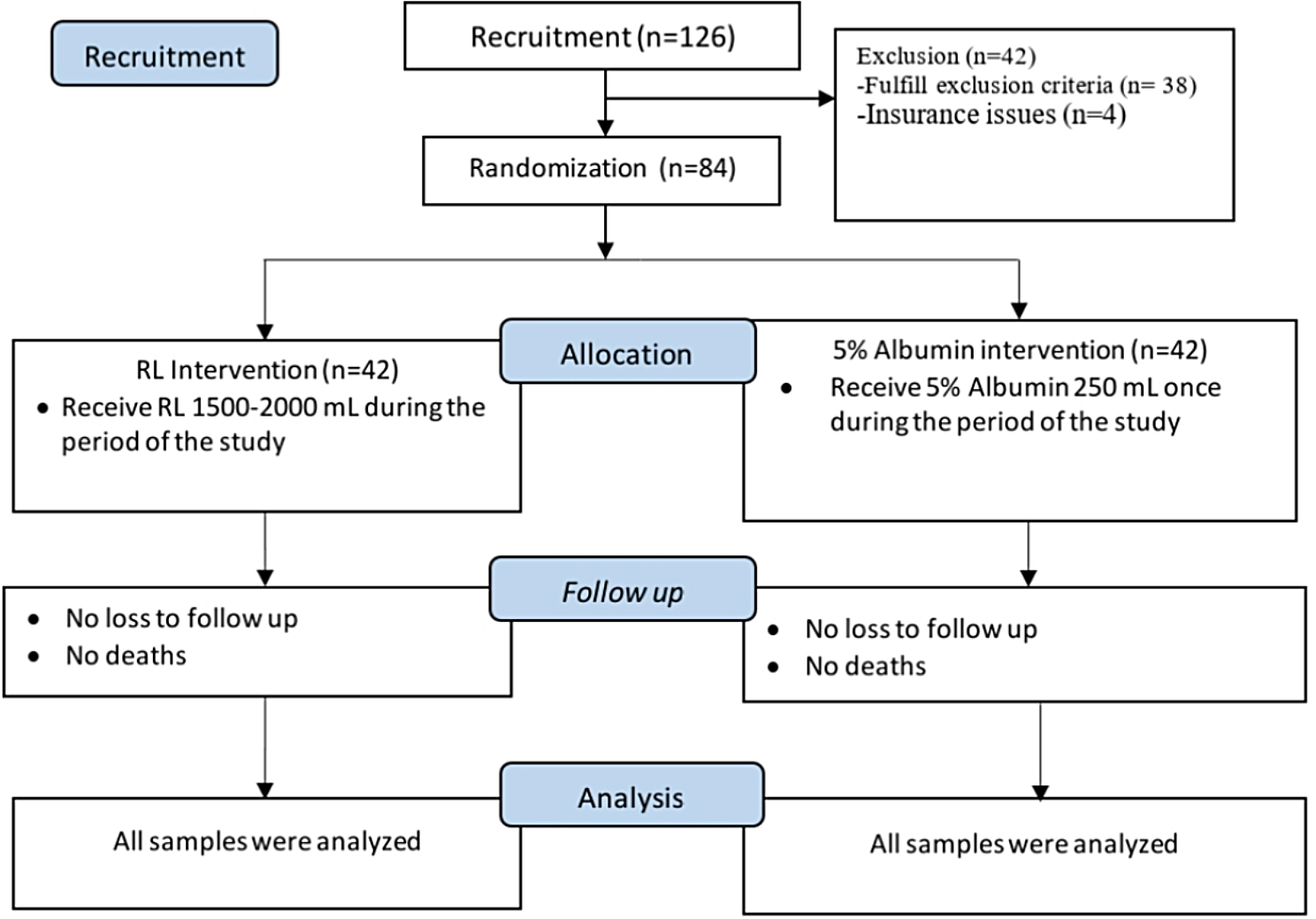
This trial used a randomized observer-blind design with 200 subjects 12 to 40 years of age. One hundred subjects were administered with an investigational vaccine (Vi-DT TCV) whereas the other hundred were administered with Vi-polysaccharide (Vi-PS) as control.
Sample size
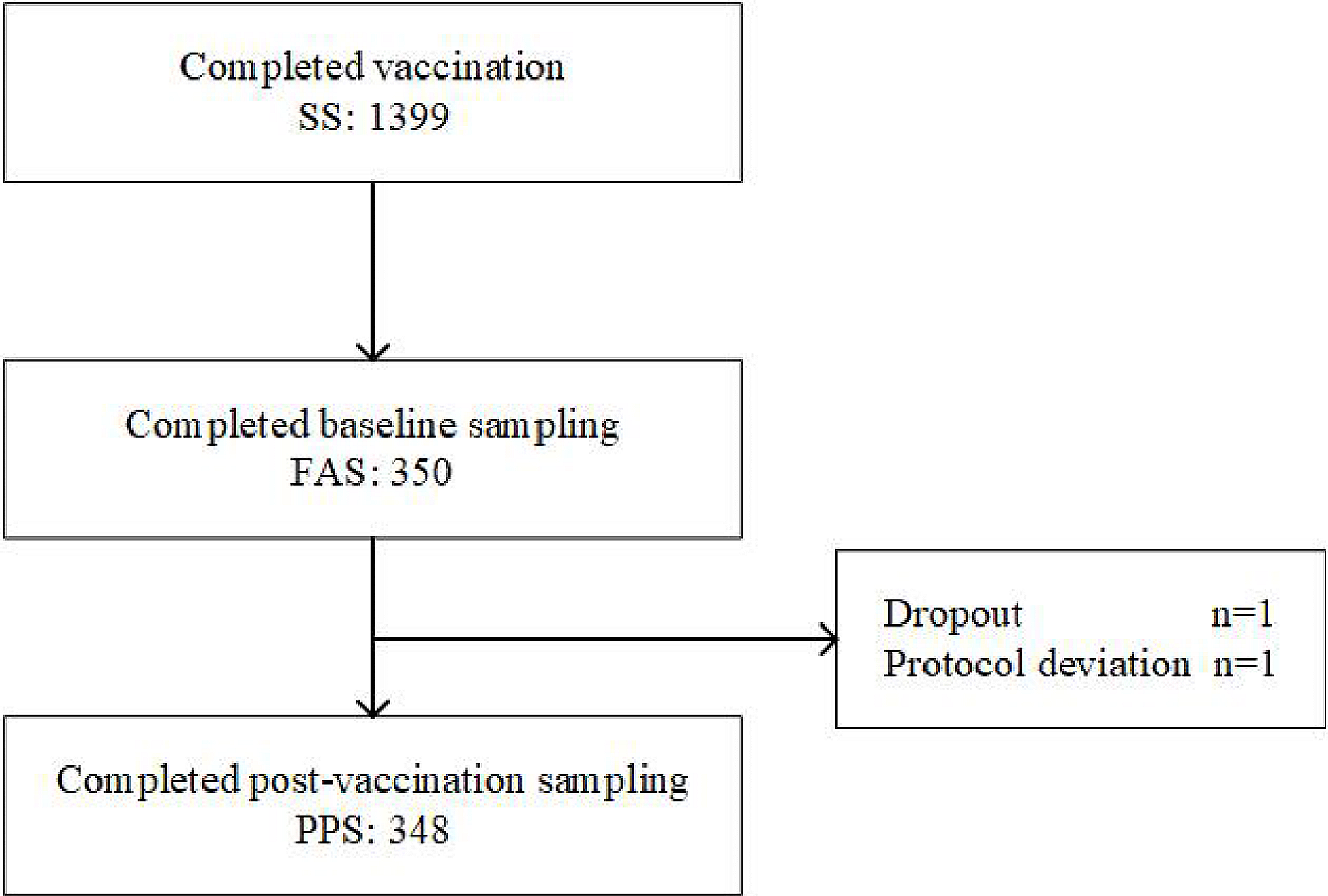
The study required 82 subjects in each group to reject the null hypothesis that seroconversion of the two groups is equal with probability power of 0.9. Assuming a 20% dropout rate, 100 subjects were enrolled in each group.
Study procedures
Subjects were given detailed information on the vaccine, solicited and unsolicited adverse events, visit schedule and contact person details. If they agreed to abide by the rules of the trial, they were given the informed consent form. After signing the informed consent form, inclusion and exclusion criteria were evaluated.
Healthy subjects who were willing to follow the rules of the trial as well as follow-up schedule and willing to sign an informed consent form were included in the trial.
Exclusion criteria were subjects who were enrolled in another trial, had a fever, had a history of allergy to the vaccine component, had a coagulopathy history, were undergoing treatment likely to alter immune response, had a chronic disease and had a history of typhoid fever. Subjects who previously received any typhoid vaccination or any other vaccine 1 month prior to vaccination and subjects who planned to leave the study area before trial completion were also excluded.
Both the trial and control vaccines were given codes, known only to the unblinded team involved in vaccine administration. The sequence of these codes was generated using a randomization website. After evaluation of inclusion and exclusion criteria by the blinded team of investigators, subjects were vaccinated with either Vi-DT or Vi-PS by the unblinded team of vaccinators based on the randomized sequence.
A blood sample was obtained prior to vaccination. Twenty-eight days post vaccination subjects were called for blood sampling and to report any adverse local and systemic reactions that occurred since vaccination. This trial was conducted in 2 primary health centers in Jakarta, Indonesia namely Senen primary health center, located in Central Jakarta and Jatinegara primary health center, located in East Jakarta.
Investigational product and control
Vi-DT vaccine manufactured by BioFarma was used as an investigational product. Each dose of this vaccine (0.5 mL) is composed of 25 µg of a purified Vi capsular polysaccharide of S. Typhi, 5 mg of 2-phenoxyethanol as preservative and 0.5 mL of phosphate buffer solution. IP was stored at a temperature of + 2 °C to + 8 °C and is in the form of multi-dose vials. Licensed Vi-PS vaccine (Typhim Vi® produced by Sanofi) was used as a control. Control was also stored at a temperature of + 2 °C to + 8 °C but is in the form of pre-filled syringes. Both vaccines were administered intramuscularly in the deltoid region.
Safety and immunogenicity evaluation
Subjects were monitored up to 30 min post vaccination to evaluate immediate local and systemic adverse reactions. Subjects were given diary cards where they had to record their daily temperature and note down any delayed local and systemic reactions that occurred after 30 min up to 28 days post vaccination. Reactions that were monitored were solicited reactions such as pain, redness, swelling, induration, fever, muscle pain, fatigue and unsolicited reactions such as vomiting, diarrhea etc. Subjects also had to record the severity of the reactions and how long they lasted. Subjects were given a telephone number of a contact person they could get in touch with if they experienced any worrisome adverse effects, had any enquiries or experienced serious adverse events. Causality of adverse events to the vaccines were determined by a data safety monitoring board (DSMB).
For immunogenicity of Vi-DT, anti-Vi IgG titers in sera were assessed pre-vaccination and 28 days post-vaccination. The ELISA method recommended by the WHO Expert committee on Biological standardization [20] was used. Geometric mean titer (GMT) and seroconversion were calculated. Seroconversion was defined as percentage of subjects with antibody increment ≥ 4 times compared to baseline.
Data for safety and immunogenicity were analyzed using SPSS.



Comments (0)