
記住我
An in-depth description of the methodology of the literature search is provided in Supplementary Appendix 1. Ethical guidelines were followed. Internal review board approval was not required because data collection was based on an available literature review.
Selection of Guideline QuestionsCandidate predictors were selected based on clinical relevance and the presence of an appropriate body of literature. Candidate predictors and prediction models were considered “clinically relevant” if, in the subjective opinion of the content experts and guideline chairs, the predictor or components of the prediction models were: (1) accessible to clinicians (universal availability of predictors was not required) and (2) likely to be considered by clinicians while formulating a neurological prognosis for patients after msTBI.
An appropriate body of literature was considered present for any predictor evaluated in published studies that included (1) a minimum of 100 study participants and (2) an appropriate multivariate analysis with the predictor of interest, patient’s age, and GCS score or motor GCS score as variables, which are proven and universally accepted parameters associated with the outcome after msTBI. For biomarkers, an appropriate body of literature was considered present if at least one external validation study in addition to the initial report on discovery of the biomarker as an independent predictor was found. For clinical prediction models, an appropriate body of literature was considered present if at least one external validation study in addition to the initial report on development of the model was found.
Based on these criteria, the following candidate predictors were selected:
Clinical variables:
1.Age
2.Pupillary reactivity on admission
3.Admission GCS score or motor GCS subscore following adequate resuscitation
4.Hypotension (systolic blood pressure [SBP] < 90 mm Hg preadmission or in the emergency department)
5.Hypoxia (oxygen saturation < 90% or arterial partial pressure of oxygen (PaO2) < 110 mm Hg before or after admission)
6.Major extracranial injury
7.Alcohol intoxication
8.Hypernatremia
9.Prolonged elevated intracranial pressure (ICP) > 20 mm Hg for > 60 min/day
10.Acute kidney injury during ICU treatment
11.Posttraumatic cerebral infarction
Of note, no biomarker was included because none met our prespecified requirements for body of literature as described.
Clinical prediction models:
1.Corticosteroid Randomization After Significant Head Injury (CRASH)-basic model
2.CRASH-CT (CRASH-basic model extended by computed tomography features) model
3.International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT)-core model
4.IMPACT-extended model (core + CT)
5.IMPACT-lab model (core + CT + lab)
6.Marshall CT classification
7.Rotterdam CT
8.Helsinki CT
9.Stockholm CT
The population/intervention/comparator/outcome/timing/setting (PICOTS) question was then framed for the specific candidate predictors as follows: “When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should [predictor or prediction model, with time of assessment if appropriate] be considered a reliable predictor of [outcome]?”.
Selection of OutcomesThe outcomes considered “critical” for the systematic review and subsequent formulation of recommendations were functional outcome (average rating 9) assessed at or beyond 6 months after msTBI, mortality (average rating 8) assessed at or beyond discharge, quality of life (average rating 8) assessed at or beyond 6 months after msTBI, and cognitive outcome (average rating 7.67) assessed at or beyond 6 months after msTBI. However, no studies that included quality of life or cognitive outcomes met the full-text screening criteria for the systematic review and could therefore not be included in this guideline. Most articles assessing functional outcome reported “poor” outcome with highly variable definitions (e.g., mostly Glasgow Outcome Scale or Glasgow Outcome Scale Extended with variable dichotomizations or ordinal use, disability-free outcome, Functional Independence Measure, Ranchos Los Amigos Score and other). We list “poor” as equivalent to “unfavorable” for consistency throughout the text of the article. Our Supplementary Table 1 and 2 display the different outcome definitions used in the included articles to represent their variability.
Systematic Review MethodologyDatabases searched included MEDLINE via PubMed, EMBASE, Web of Science, and the Cochrane Database of Systematic Reviews. The librarian search string used for this systematic review is listed in the Supplementary Appendix 1. Full-text screening was performed with the following exclusion criteria: (1) sample size less than 100, (2) studies focused on a highly selected subgroup (such as penetrating TBI or patients with isolated subdural hematoma), (3) studies of predictors not evaluated in multivariate analysis, (4) studies focused on a genetic polymorphism as a predictor, and (5) studies of clinical prediction models that did not report model discrimination. Studies of laboratory biomarkers were included only if the biomarker was considered clinically relevant and had been evaluated in two or more published studies that met other criteria. Studies were screened for several sources of bias while selecting full-text articles for further review.
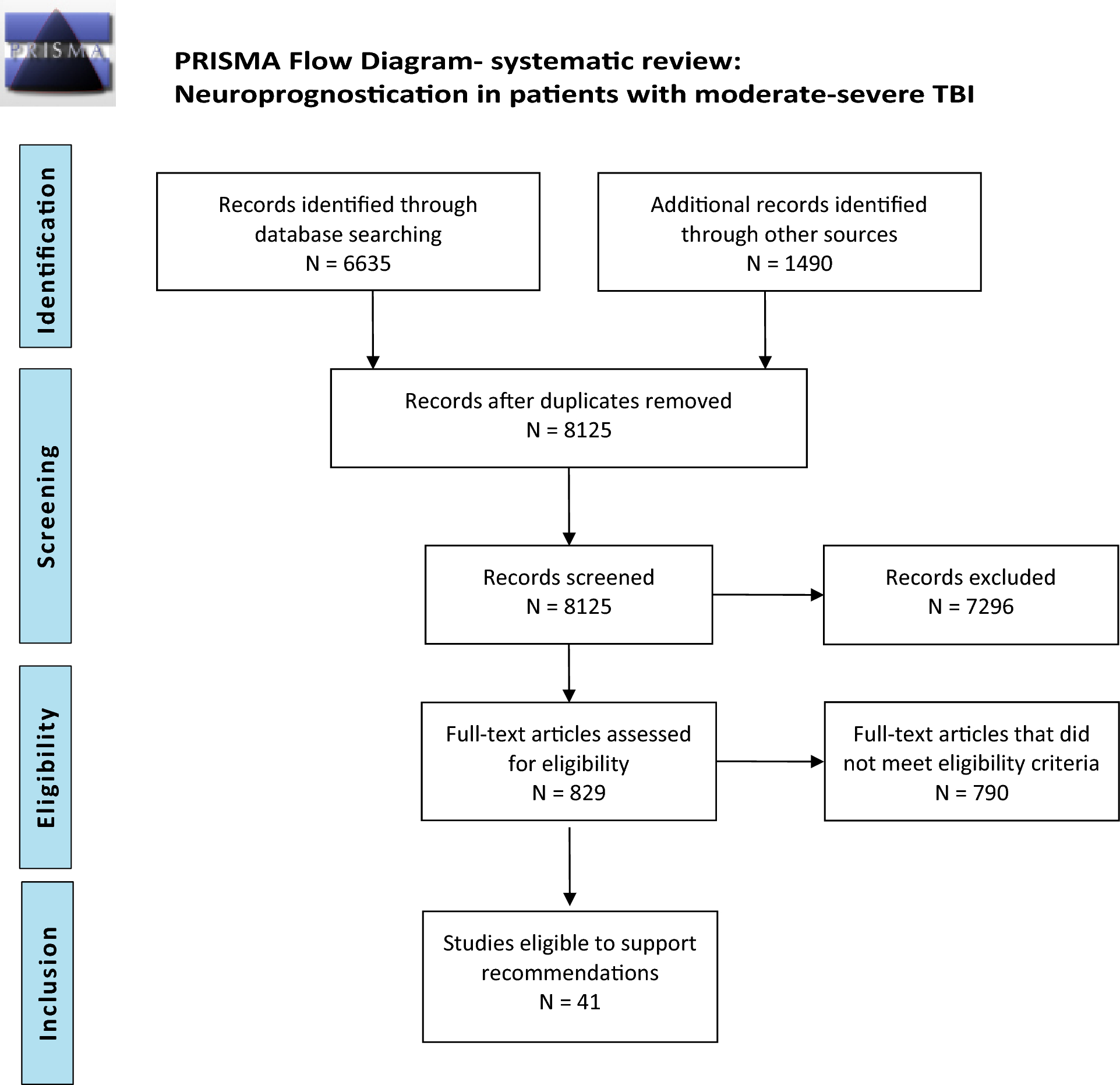
Because the librarian’s search was conducted in April 2019, we subsequently performed an additional literature search to include studies until October 2022, using the search words “traumatic brain injury,” “outcome,” and “2019” or “2020” or “2021” or “2022”, respectively. Altogether, 1,490 abstracts were found meeting these criteria. Using the same selection criteria, abstract screening and full-text evaluation was done, resulting in additional 27 articles meeting the GRADE criteria. A total of 8125 abstracts were screened, with 831 full-text articles assessed for eligibility and a total of 41studies included in our qualitative synthesis (Fig. 1).
Fig. 1
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram depicting the method of systematic review
A summary of individual studies is provided in Supplementary Table 2 (individual predictors) and Supplementary Table 3 (prediction models). A color-coded overview summary of the quality of evidence for individual predictors and prediction models are provided in Table 2. The GRADE evidence profile and summary of findings table for predictors of mortality and functional outcome are shown in Table 3 (individual predictors) and Table 4 (prediction models).
Table 2 TBI summary table of recommendationsTable 3 GRADE evidence profile/summary of findings table: neuroprognostication: msTBITable 4 GRADE evidence profile/summary of findings table: neuroprognostication: msTBIEvidence to Recommendation Criteria 1.Quality of evidence/certainty in the evidence and effect size: For the purposes of these guidelines, predictors described as “reliable” have both a higher overall certainty in the evidence and greater effect size than “moderately reliable” predictors (Table 1). For reliable predictors, one downgrade was permitted for risk of bias but none for inconsistency, imprecision, or indirectness, and the overall quality of evidence had to be high or moderate. Reliable prediction models were required to demonstrate an area under the receiver operating characteristic curve (AUC) of > 0.8 and no evidence of miscalibration in external validation studies that reported calibration. Downgrades for risk of bias, imprecision and indirectness were permitted for moderately reliable individual predictors, but a downgrade for inconsistency was not. Moderately reliable prediction models were required to demonstrate an AUC > 0.7, and limited miscalibration in some external populations was allowed. Predictors that did not fit “reliable” or “moderately reliable” criteria were classified as “not reliable.”
2.Balance of desirable and undesirable consequences: In the context of msTBI, neuroprognostication is focused on the prediction of poor outcomes in the literature. An accurate prediction of poor outcome is expected to result in grief, a sense of loss, and anxiety about the future. However, a desirable consequence of accurate prediction of a poor outcome is the ability of surrogates and the clinical team to align goals of care to the perceived wishes of the patient with msTBI. Potential benefits to the family and surrogates in this situation include greater certainty and decreased decisional conflict in making patient value-congruent decisions, a sense of closure, and satisfaction from respecting the patient’s wishes. Inaccurate prediction of a poor outcome (i.e., a false-positive prediction of poor outcome), however, may lead to WLST in an individual who would otherwise have made a meaningful recovery. Because WLST almost always leads to death in patients with msTBI, the undesirable consequences of an inaccurate prediction of poor outcome were thought to greatly outweigh the desirable consequences, unless certainty in the evidence of the predictor or prediction model was high (i.e., a low false-positive rate). Other potential undesirable consequences include the risk of events such as loss of airway, hemodynamic instability, inadvertent removal of catheters, and cardiac arrest during transport of a critically ill patient for tests such as brain imaging.
3.Values and preferences: The panel agreed that most individuals, as well as their families and surrogates, would likely consider an inaccurate prediction of poor outcome that led to the death of a patient who might otherwise have had a reasonable recovery to be more undesirable than a prolonged period of uncertainty in the outcome. Therefore, a high certainty in the evidence of predictor or prediction model accuracy was necessary to recommend consideration when counseling families and surrogates on prognosis in this context. The values and preferences of a patient are central to any discussion with surrogates but are also difficult to determine. Shared decision-making based on careful prognostication is critical for the determination of treatment options and goals-of-care decisions.
4.Resource use: Resource use varied across predictors and models. Whereas some predictors, such as the qualitative assessment of the pupillary light response or best motor response, require no significant expenditure of resources, other predictors, such as magnetic resonance imaging (MRI) and measurement of biomarker levels, do involve significant expenditure of resources, for example, in the cost of the diagnostic test itself, the need for personnel to transport the patient and perform the test, and the potential for medical or neurological deterioration from being in the MRI scanner, a less closely monitored environment, for an extended period of time. An accurate prediction of poor outcome, however, may lead to better alignment of goals of care with the patient’s wishes and avoid extended use of resources, over days to years, in patients destined to suffer a poor outcome. The use of resources was therefore thought to favor consideration of a predictor or prediction model during prognostication, contingent on high confidence in its predictive accuracy. In situations in which goals of care have been established and are unlikely to change, however, resource use involved with performance of the test should likely be considered, and expensive tests not expected to alter the treatment plan should be avoided.
Good Practice StatementsIn accordance with recommendations of the GRADE network, these statements were considered by the panel to be actionable, supported by indirect evidence where appropriate, and essential to guide the practice of neuroprognostication. The good clinical practice reflected in these statements lacked a meaningful body of direct supporting evidence (typically because of insufficient clinical equipoise) but was considered by the panel to be unequivocally beneficial.
1.We recommend that prognostication should be performed with consideration of the complete clinical condition and not be based on a single variable (strong recommendation, evidence cannot be graded).
2.We recommend that prognostication should not be performed based only on ultra-early injury characteristics in the first 3 days. TBI is characterized by a primary injury and secondary injuries, including growing hemorrhagic lesions and microcellular processes with possible neurological worsening. In addition, patients with msTBI may have additional nonneurologic trauma (“polytrauma”), which may influence a patient’s hospital course and outcome. Unless irreversible brain stem damage has occurred with imminent death or unless there are documented predetermined wishes by the patient not to receive any critical care support even when the prognosis is uncertain, we suggest a minimum of 3 days or longer of full critical care support, including surgical procedures and, if possible, at least 1–2 weeks of full critical care or medical support before attempting neuroprognostication. Even after 2 weeks, prognosis may be uncertain, especially when patients remain unconscious (strong recommendation, evidence cannot be graded).
3.We recommend that prognostication should be performed carefully with an acknowledgment of uncertainty and without nihilism and should only be performed with consideration of all available evidence and not be based on personal anecdotal experience alone (strong recommendation, evidence cannot be graded).
Recommendations: Clinical Variables as PredictorsTable 3 (GRADE summary table) shows details on quantitative ranges for the point estimates and 95% confidence intervals (CIs) for each variable and outcome.
Outcome: MortalityPICOT Question 1“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should age alone be considered a reliable predictor of mortality?”
Description of the predictor: Numeric age assessed and documented at the time of trauma.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that age alone not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation; low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of self-fulfilling prophecy, statistical analysis, study confounding, study attrition, and study participation [14,15,16,17,18]. Furthermore, the evidence was downgraded for imprecision. A large body of literature has assessed and confirmed an independent association of age and poor outcome after msTBI. Consequently, age is also a factor included in more complex prognostic models. However, an appropriate cutoff age has not been identified above which death is certain. Although increasing age was an independent predictor of mortality, with evidence being strongest for patients more than 70 years of age, the criteria for reliability as an individual predictor (compared to a component of a prediction model) were not met, as detailed in the How to use these guidelines and Evidence to recommendation criteria sections. The body of evidence was at high risk of bias from self-fulfilling prophecy. Survival and even good outcome may well be possible in older patients with msTBI.
PICOT Question 2“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should bilaterally nonreactive pupils alone, measured on admission, be considered a reliable predictor of mortality?”
Description of the predictor: Bilaterally nonreactive pupils at the time of hospital admission.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that bilateral pupillary nonreactivity measured on admission be considered a moderately reliable predictor of in-hospital mortality, conditional on accurate assessment without confounding medications or injuries (weak recommendation, low-quality of evidence).
Rationale: Only a few studies met our predetermined criteria to support any recommendations [18,19,20,21,22]. The body of evidence was downgraded for imprecision and risk of bias from participation, study attrition, and the self-fulfilling prophecy because presence of bilaterally fixed pupils may result in early end-of-life decisions [18,19,20,21,22]. Accurate assessment of the pupillary light response is crucial, without confounding by medication, external injury (e.g., orbital trauma), diffuse axonal injury in the mesencephalon, TBI-related seizures, prior surgery, and an overall clinical picture consistent with compression of the third cranial nerve with elevated ICP. Patients may have bilaterally nonreactive pupils but may not meet criteria for brain death and may be kept alive with mechanical ventilation and other life-sustaining measures, including avoidance of WLST, for a prolonged period. Therefore, together with several downgrades in the body of evidence, we suggest that presence of bilaterally nonreactive pupils alone may be considered a moderately reliable predictor of mortality.
PICOT Question 3“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should a single nonreactive pupil alone be considered a reliable predictor of mortality?”
Description of the predictor: Single nonreactive pupils at the time of hospital admission.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that single pupillary nonreactivity alone not be considered a reliable predictor of in-hospital mortality (weak recommendation; low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias and imprecision [20, 23]. A unilaterally fixed pupil may be the sign of a mass lesion (e.g., herniation from a large subdural hematoma) or traumatic axonal injury at the level of the third nerve nucleus. Thus, many patients with a single reactive pupil may survive (e.g., with time in case of traumatic axonal injury or if rapid surgical intervention is initiated in case of a subdural hematoma). Thus, a unilaterally unreactive pupil measured on admission should not be used as a predictor.
PICOT Question 4“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should the GCS score or the motor subscore of the GCS alone following adequate resuscitation be considered a reliable predictor of mortality?”
Description of the predictor: GCS score or motor subscore of the GCS examined at the time of hospital admission following adequate resuscitation.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that the GCS score or the motor subscore of the GCS alone, assessed on admission after adequate resuscitation, not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation; low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the Quality in Prognosis Studies (QUIPS) domains of participation bias, study attrition, confounding, statistical analysis, and self-fulfilling prophecy [14, 15, 18,19,20,21]. Inconsistency was present. The GCS score and motor GCS score have been assessed as a single factor or as part of prognostic models. Several studies have shown an association between a low GCS score and mortality. However, the risk for a falsely low GCS score is very high because of an imprecise assessment at the time of assessment in the field and the possible influence of the GCS by other factors (e.g., intoxication, per-intubation medications), resulting in a recommendation for the GCS/motor GCS score not to be a reliable predictor alone for mortality.
PICOT Question 5“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should hypotension alone in the field or at the time of hospital admission be considered a reliable predictor of mortality?”
Description of the predictor: Hypotension (SBP < 90 mm Hg) at a single time point or more prior to or at the time of hospital admission.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that hypotension (SBP < 90 mm Hg) alone, assessed prehospitalization or in the emergency department, not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation; low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of participation bias, study attrition, confounding, and self-fulfilling prophecy [14, 20, 24,25,26]. Inconsistency was present. Blood pressure may not be measured or documented accurately, particularly in the prehospital setting. Furthermore, the thresholds (extent and duration or dose) of hypotension with or without intracranial hypertension that predict death of an individual patient are not clearly defined. Therefore, the false-positive rate is likely to be significant and does not favor considering the predictor alone for prognostication while counseling family and surrogates.
PICOT Question 6“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should hypoxia alone in the field, at the time of hospital admission, or during ICU treatment be considered a reliable predictor of mortality?”
Description of the predictor: Hypoxia (oxygen saturation < 90% or PaO2 < 110 mm Hg) a single time point or longer prior to or on admission or during the ICU treatment.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that hypoxia alone, assessed prehospitalization, on admission, or during the ICU treatment (oxygen saturation < 90% or PaO2 < 110 mm Hg), not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation; low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the QUIPS domains of participation bias, study attrition, prognostic factor measurement, confounding, self-fulfilling prophecy [20, 24, 27, 28], and imprecision. In the studies meeting our prespecified requirements, hypoxia was defined in various ways. Oxygen saturation may not be measured or documented accurately, particularly in the prehospital setting. Furthermore, the thresholds (extent and duration, dose) of hypoxia that predict the death or poor outcome of an individual patient are not clearly defined. Therefore, the false-positive rate is likely to be significant and does not favor considering the predictor alone for prognostication while counseling family and surrogates.
PICOT Question 7“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should elevated ICP alone be considered a reliable predictor of mortality?”
Description of the predictor: Elevated ICP (most often defined in the literature as ICP > 20 mm Hg) may be observed at any time during the hospital admission. This could be a single elevated value > 20 mm Hg or a longer-lasting “dose” of ICP > 20 mm Hg (such as duration of > 5 min), both early and in delayed fashion during the hospital course.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that elevated ICP, including the duration (dose) of early or delayed intracranial hypertension, alone not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation; very low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of study attrition, prognostic factor measurement, outcome measurement, and self-fulfilling prophecy [18, 19, 25, 29]. The evidence was further downgraded for imprecision and inconsistency. Although an association of prolonged elevation of ICP with mortality and poor outcome has been documented in a variety of studies, definitions of elevated ICP varied widely, durations were not consistently assessed, and extreme values were not defined. The thresholds (extent and duration, dose) of high ICP that may result in death are uncertain. The false-positive rate may be very high.
PICOT Question 8“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should major extracranial injury alone be considered a reliable predictor of mortality?”
Description of the predictor: Many patients with msTBI present as polytrauma patients with other injuries to other organ systems other than the brain. Commonly, the severity of such extracranial injury is measured by the injury severity score.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that major extracranial injury alone not be considered a reliable predictor for hospital mortality or disease-related mortality beyond discharge (weak recommendation, moderate-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of study participation, study attrition, study confounding, and self-fulfilling prophecy [14, 20, 30,31,32]. Extracranial organ trauma may be a separate cause of death or may cause low brain perfusion or oxygenation. However, the spectrum of extracranial injuries additional to msTBI varies widely, with exact definitions for major organ injury or failure completely missing or imprecise in some studies. Thus, major extracranial injury should not be used as a predictor of mortality.
PICOT Question 9“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should acute kidney injury (AKI) alone be considered a reliable predictor of mortality?”
Description of the predictor: AKI according to the Kidney Disease Improving Global Outcome criteria during hospitalization is defined as an acute increase in the absolute serum creatinine level of at least 0.3 mg/dL (or an increase of 50%) or a decrease in the urine output (oliguria: urine level < 0.5 mL/kg per hour for more than 6 h).
Recommendation When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that AKI during ICU treatment alone not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation; low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias in the domains of study participation, study attrition, self-fulfilling prophecy, and outcome measurement [33, 34]. The evidence was further downgraded for imprecision. AKI affects 2–12% of patients with msTBI; however, various definitions have been used in different studies. Also, the different stages of AKI were not analyzed for their impact on mortality. Furthermore, AKI may be fully reversible; therefore, the risk for a false-positive finding may be very high. Thus, AKI should not be used as a predictor for mortality.
PICOT Question 10“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should the presence of alcohol in the blood alone on admission be considered a reliable predictor of mortality?”
Description of the predictor: Positive alcohol test on admission.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that positive testing for alcohol on admission alone not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation, low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of study participation, study attrition, prognostic factor measurement, study confounding, and self-fulfilling prophecy [35, 36]. Inconsistency was present. Intoxication with alcohol may cause a falsely low GCS score on admission and subsequently a false stratification of patients into msTBI. Intoxicated patients may improve significantly as their alcohol levels diminish with time, often by the next day. Thus, a positive alcohol test on admission should not be used as a predictor for mortality according to the PICOTS question.
PICOT Question 11“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should hypernatremia alone be considered a reliable predictor of mortality?”
Description of the predictor: Hypernatremia defined as a serum sodium level > 160 mmol/L during the ICU stay.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that hypernatremia during ICU treatment alone not be considered a reliable predictor of hospital mortality or disease-related mortality beyond discharge (weak recommendation, very low-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of study attrition, confounding, and self-fulfilling prophecy [37, 38]. Inconsistency and imprecision were present. From a pathophysiological point of view, hypernatremia may be indicative of a particularly severe TBI with hypothalamic dysfunction or may be a marker of the frequent administration of osmotherapy (mannitol, hypertonic saline). Hypernatremia, especially when iatrogenic, is a treatable and reversible condition. Numerous studies have found an association between the occurrence of hypernatremia and outcome/mortality. However, only very few studies met our criteria. These studies had different cutoff points for hypernatremia. One study suggested that possibly co-occurring hyperchloremia, and not hypernatremia itself, may be associated with mortality [37].
Outcome: Functional Outcome at 6 Months and BeyondPICOT Question 12“When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, should age alone be considered a reliable predictor of poor functional outcome at 6 months and beyond?”
Description of the predictor: Numeric age assessed and documented at the time of trauma and correlated with outcome.
Recommendation: When counseling family members and/or surrogates of patients with msTBI admitted to an ICU, we suggest that age alone not be considered a reliable predictor of functional outcome at 6 months and beyond (weak recommendation, moderate-quality evidence).
Rationale: The body of evidence was downgraded for risk of bias, with various studies demonstrating potential bias in the domains of study attrition, confounding, statistical analysis, and self-fulfilling prophecy [15, 16, 23, 39,40,41]. A large body of literature has assessed and confir
留言 (0)