In this report, we demonstrate that in an integrated HIV-HBV clinic in Malawi 25.2% of referred patients had sonographic signs of cirrhosis. Overall, treatment was indicated in 45 patients and POCUS alone can help to indicate same-day initiation of HBV antiviral therapy in 68.9% of them. It was further found that clinicians can be trained to provide liver POCUS with fidelity.
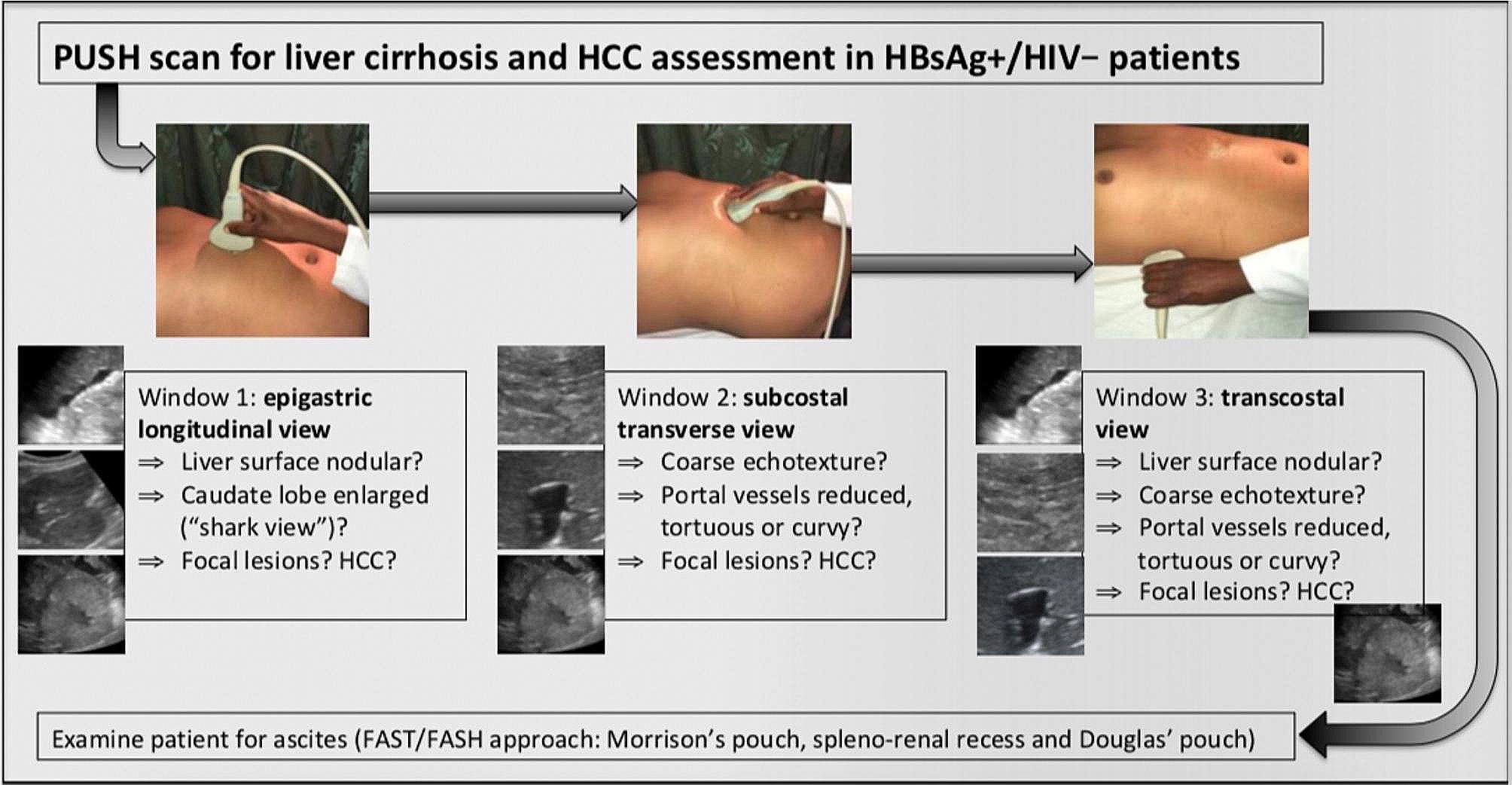
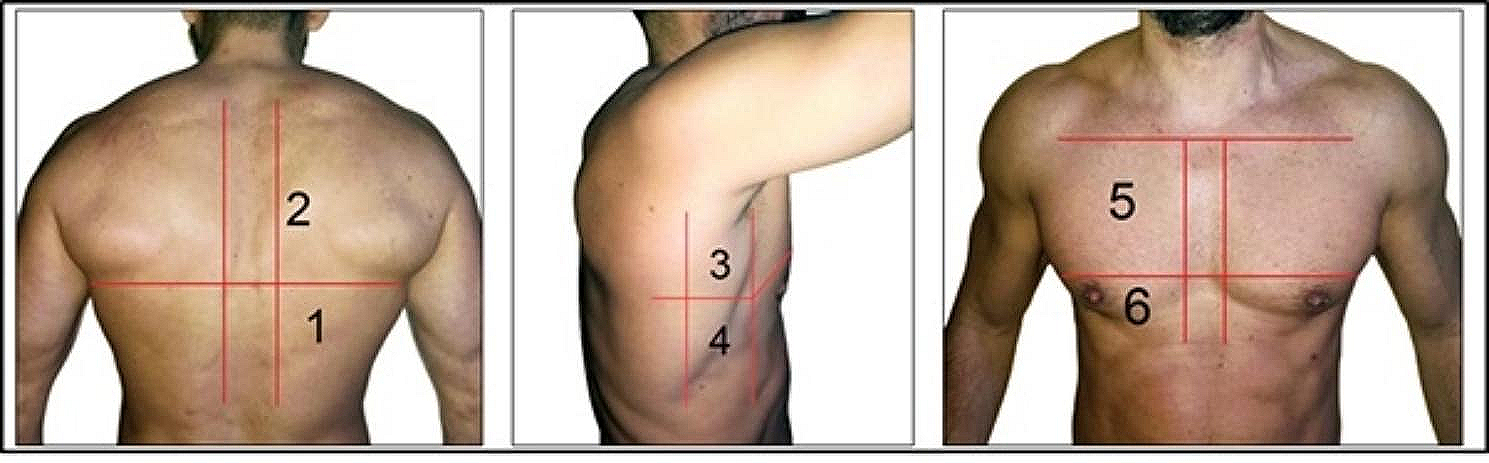
Changes suggesting liver cirrhosis well described in the literature are irregular liver surface [5, 17, 18] (Fig. 2), coarse echotexture of the tissue [5, 17, 18] (Fig. 4) as well as paucity of peripheral vessels, which may have a tortuous course [17] (Fig. 5). Liver surface nodularity is considered likely the most sensitive and reproducible US signs of cirrhosis [19, 20]. It has been suggested [21, 22] that the use of a linear high-frequency probe can increase the sensitivity of liver ultrasound, especially in detecting surface changes and echotexture. While this was not used during our study, we have since found it helpful for assessment of ambiguous cases. In line with previous reports [23], we noted that findings of cirrhosis due to HBV may be easier to visualize than those due to other causes, as CHB usually leads to macro-nodular cirrhosis [24]. This leads to more marked changes and all sonographic findings were frequently seen in our patient population.
Changes of the liver shape in cirrhosis are also well described [17, 18] with shrinking of the right lobe and relative enlargement of the left and especially of the caudate lobe. It is attributed to relative obstruction of the hepatic veins, causing greater blood flow through the caudate lobe and thereby hypertrophy [25]. In our protocol, we did not use the measured comparison to the right liver lobe originally proposed [26], but instead eyeballed its size using the liver shape in the sagittal view [17] (Fig. 3). Detection of more subtle anatomical changes in cirrhotic livers, like expansion of the gallbladder fossa [27] and enlarged hilar space [28], were not included in the protocol. In our experience, the coarse echotexture (85.7%) and the nodular surface (83.1%) were most frequently detected followed by scarcity of vessels (71.4%) and were comparable in their diagnostic value. An enlarged caudate lobe was only recognized in 32.1% of our patients and was always associated with other changes, so it did not add to diagnostic accuracy and could potentially be dropped from the protocol.
Many patients with HCCs present late in our setting and have large palpable tumors, sometimes visible as an abdominal bulge [29], which makes their sonographic detection easier (Fig. 6). Ultrasound findings described of advanced HCC are a mosaic pattern, which is often hyperechoic and may have peripheral halo [30]. Dilated intra-tumoral blood sinusoids and perinodular daughter nodule formation are seen. It should be noted that unlike in chronic HCV and other chronic liver diseases, HCC can occur in the context of CHB without cirrhosis, and is an especially featured cancer in young male African patients with CHB [31].
As discussed, while ultrasound is useful to identify cirrhosis, it is not sufficiently sensitive in detecting early stages of liver fibrosis [7, 32]. It is therefore important to use other approaches of non-invasive liver assessment in parallel like e.g., the APRI score with an adapted threshold [13]. Ultrasound elastography is recommendable [3, 4, 8] and would be helpful if simple, stable and affordable devices were available. These gaps in assays for liver disease staging and absent HBV markers like viral load are expected to undermine scale-up of HBV therapy; therefore, a liver POCUS protocol with even moderate sensitivity may help close gaps in the care cascade.
The feasibility to train clinicians in a POCUS approach to the cirrhotic liver and HCC is essential for a wider utilization of ultrasound in the resource-poor setting as radiological services are often scarce [33]. The agreement in our study between trainer and trainee showed substantial or near perfect agreement for all findings except for assessment of caudate lobe size, where only moderate agreement (κ = 0.58) was seen. These values suggest that trainees can recognize the changes with fidelity. A recent study in a high-resource setting showed that emergency physicians can significantly increase their sensitivity and specificity in diagnosing cirrhosis using ultrasound [34]. The study assessed only image interpretation but not image acquisition; nevertheless it convincingly argues, that viewing the liver is frequently required in protocols like the FAST exam, and clinician thus should have competency to obtain images of liver parenchyma and surface. Another recent study favorably compared hand-held POCUS by clinical hepatologists to radiology ultrasound, transient elastography, and liver biopsy [35].
Our study has a few weaknesses that warrant discussion. Our trainee clinicians were previously trained in POCUS, especially in FAST and FASH [9] but also e.g., in cardiac applications [36]. These are frequently used, so they cannot be described as “inexperienced” in clinical ultrasound. Therefore, the feasibility to train clinicians with less POCUS experience will still need to be established. Another limitation was that, in our evaluation, trainee clinicians were not blinded to the clinical and the laboratory results. Furthermore, they were able to discuss scans between each other as part of their clinical routine. Therefore, they may have reported ultrasound findings of cirrhosis based on taking a history, physical examination, and/or review of lab values. Feedback by the expert was given on each case thus improving their learning curve over time. The high concordance between the scans should thus not be over-interpreted. In further studies, the PUSH protocol should be validated in a blinded study design, i.e., without US operators being aware of the laboratory results as these could influence the interpretation of ultrasound findings. Additionally, future evaluations should possibly include comparison to other modalities (e.g., elastography). Nevertheless, our pilot data shows that liver ultrasound using a simple, standardized approach like the PUSH protocol can be integrated in clinical care in resource-poor settings when ultrasound is available and training can be provided.


Comments (0)