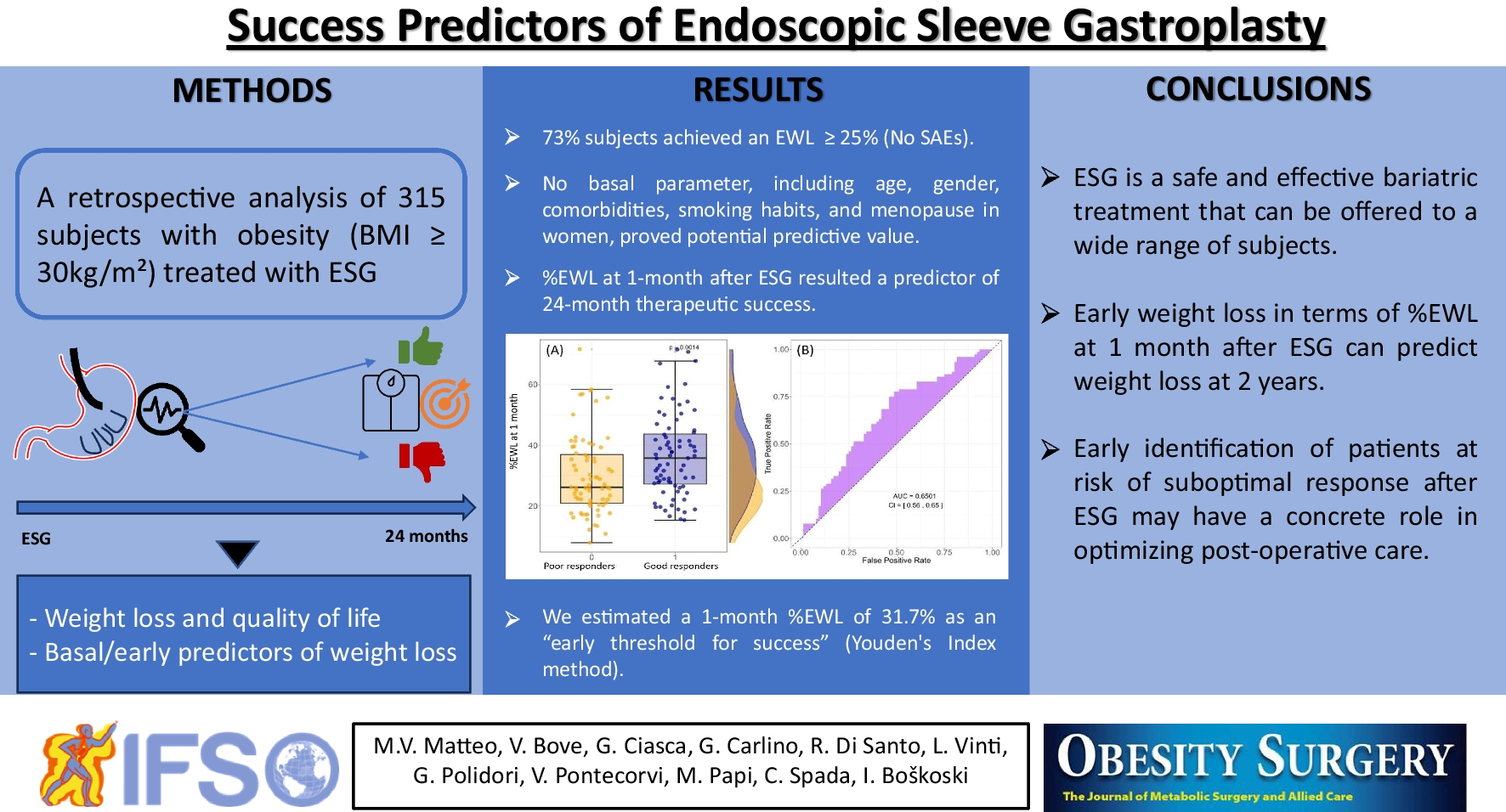
In the past 10 years, endoscopic sleeve gastroplasty emerged as an effective and minimally invasive bariatric treatment enriching the available tools to fight the obesity pandemic. Several studies reported the safety and efficacy of ESG, including a recent randomized controlled trial showing an additional 12.6% of %TBWL in patients undergoing ESG compared with participants undergoing moderate-intensity lifestyle modifications alone [6, 8,9,10,11,12,13,14]. Our study further confirms the efficacy of ESG up to 2 years after the procedure, with 73% and 64% of treated subjects showing a %EWL >25% and a %TBWL >10%, respectively, which is consistent with the data reported in the ESG group of MERIT trial [14]. Furthermore, we observed no severe adverse events on a pretty large cohort of patients thus supporting the favorable ESG safety data [14, 21].
Our model allows a visual representation of the weight loss and quality of life outcomes over time. As anticipated, the temporal trends of the three parameters are closely interlinked. Our data show a rapid weight loss and improvement in quality of life reaching a peak at about 8–9 months after the procedure, followed by a slow decrease. As such, the time point at which we expect to see the best results is about 9 months after the procedure. However, the following decrease is slow and exponential towards a plateau suggesting that a large part of the results achieved are maintained over time.
Although the values are consistent within the experimental uncertainty, the higher tG of the BAROS score suggests that the increase in this index is delayed of about 1 month compared to %EWL and %TBWL, while the decrease in BAROS seems to slightly precede that of the weight parameters. As the BAROS score includes both %EWL and parameters of patients’ well-being, this evidence may be probably due to the patient’s need to personally experience physical improvement before achieving greater psychological well-being and awareness of quality-of-life improvement. Further, the BAROS score seems to decrease before weight loss parameters. In this regard, we hypothesize that patients may experience psychological discomfort caused by the saturation phase of physical improvements in terms of weight. However, the data presented do not allow us to verify this hypothesis. Some studies have already described the relationship between endoscopic bariatric treatments and improvement in quality of life. A metanalysis by Gadd et al. including studies on several bariatric endoscopic techniques showed that they may improve short-term quality of life and mental health alongside weight loss [22]. With a specific view on ESG, Mehta et al. showed a continuous positive association between the maximum weight loss achieved after ESG and the improvement in quality of life assessed with several validated questionnaires [23]. Further, Fiorillo et al. evaluated the Gastrointestinal Quality of Life index in a matched cohort study comparing ESG and laparoscopic sleeve gastrectomy (LSG), showing that despite the inferior weight loss (%EWL 39.9% ESG vs. 54.9% LSG, p = 0.01), ESG was associated with better quality of life compared with LSG, with definite advantage for the gastrointestinal symptoms [24]. In this regard, several observational studies and metanalysis comparing ESG and surgical restrictive interventions, mainly LSG, confirmed that restrictive surgery is superior to ESG in terms of weight loss, though ESG showed a better safety profile [25,26,27,28]. A such, the lower invasiveness and the favorable safety profile are strong points of the ESG, making it more acceptable than its surgical counterpart.
As obesity is a complex multifactorial disease, the results of bariatric treatments, including gastric suturing, may vary considerably between patients. As such, the identification of success predictors may have a relevant impact on clinical practice. Our analysis failed to find baseline characteristics that may predict success.
First, the patient’s gender does not seem to impact ESG outcomes, despite significantly higher age, BMI, and prevalence of comorbidities in the male cohort, as typically observed in bariatric cohorts [29]. The presence of comorbidities such as diabetes, hyperinsulinemia, hypertension, or OSAS were similar between the good and poor responders. Similarly, smoking habits and menopause in women do not appear to be indicative of potential predictive value. This is not bad news as both these conditions have been related to weight changes in the general populations, while seem to not affect outcomes of ESG. Previous studies reported that younger age is a predictor for better weight loss, probably because young people are more able to change their dietary and behavioral habits [9, 14, 15]. However, our analysis suggests that the initial stages witness greater weight loss among the younger population, while a largely similar trend emerges between younger and older patients in the long run. This evidence confirms what was reported in a previous study, supporting the use of ESG as a valid therapeutic strategy also in elder patients with obesity [30].
Although our analysis did not allow us to find a basal predictor, we observed a statistically significant difference in terms of %EWL between good and poor responders at 1 month (33% (25–41%) vs. 26% (22–36%), p = 0.040). Further, as no cases of stenosis or persistent vomiting occurred after ESG, the impact of these events on weight loss can be ruled out. Hence, the %EWL at 1 month may serve as a very early predictor of success at 24 months after ESG, with acceptable reliability (Fig. 4). The absolute difference in terms of %EWL between the two groups present a small overall effect size, consistent with the onset of a weight loss process that will then unfold over several months. This initial small effect size corresponds to a wide interquartile range associated with the substantial inter-individual variability among different subjects, a bottleneck that our study shares with similar investigations. Nevertheless, the substantial sample size in our study allows us to achieve statistically significant differences, both in Fig. 4 and in the AUC value. Furthermore, the statistically significant correlation shown between weight loss in the first month and the long-term value is notable. This data confirms that reported by Sharaiha et al. [13]. However, our analysis is reinforced by setting the success threshold above 25% to achieve more statistical power and allowed us to estimate a novel threshold of 1 month %EWL to detect patients at “risk of failure” in the long term, which is particularly relevant to optimize post-operative care. According to our estimation, patients not reaching the %EWL threshold of 31.7% at 1 month after ESG may be identified as at risk of poor results in the long term. For instance, these patients may benefit from additional treatments such as pharmacological drugs, including GLP-1 analogs, psychological support, or even repeating ESG [31, 32].
This study is limited by the retrospective design, the lack of a control group, and the single-center nature limiting generalization of data and intrinsically characterized by a potential selection bias. Further, our analysis is not extended beyond 2 years and would need long-term confirmation (at least 3 and 5 years) when a proportion of patients may experience weight regain due to the chronic relapsing nature of obesity. Despite the pretty long period of recruitment, only a limited percentage of patients reached long-term follow-up, preventing us from having sufficient statistical power to perform a proper analysis beyond 2 years of follow-up. Indeed, loss of follow-up is a common and big issue in routine clinical practice, especially in patients with obesity, and this is difficult to overcome. Despite of that, the analysis was conducted on a pretty large number of patients for a monocentric study and allowed us to find a simple and easy-to-use parameter such as the %EWL at 1 month to modulate the post-operative management from an early stage. Certainly, our findings should be verified and validated in future ad hoc designed prospective multicenter studies. Further, with a view to a personalized medicine, other potential factors that may predict ESG outcomes should be investigated, such as the hormonal profiles and the intestinal microbiome, whose modulation could be integrated the endoscopic treatment of obesity.


留言 (0)