Study Design
In this hospital registry study, we analyzed surgical cases performed between January 2010 and June 2020 at Beth Israel Deaconess Medical Center (BIDMC) in Boston, MA, USA. Data were obtained from several hospital databases, and were subsequently de-identified and merged into a data repository. The local institutional review board reviewed the study and determined that the study met the criteria for exempt status, and the requirement for informed consent was waived (protocol numbers: #2022P000709 and #2022P001059). This study was conducted in accordance with the Helsinki Declaration of 1964 and its later amendments. This manuscript adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [7].
Study Population
Adult patients who underwent surgery or interventional procedures under general anesthesia and received fentanyl, morphine, or hydromorphone intraoperatively were considered for inclusion. We excluded patients with American Society of Anesthesiologists (ASA) physical status classification > IV, those undergoing cardiac surgeries, and those kept intubated after the procedure. For each of the opioids, a single cohort was created. Cases with missing data for confounding variables were excluded, adopting a complete-case method approach.
Product Waste Description
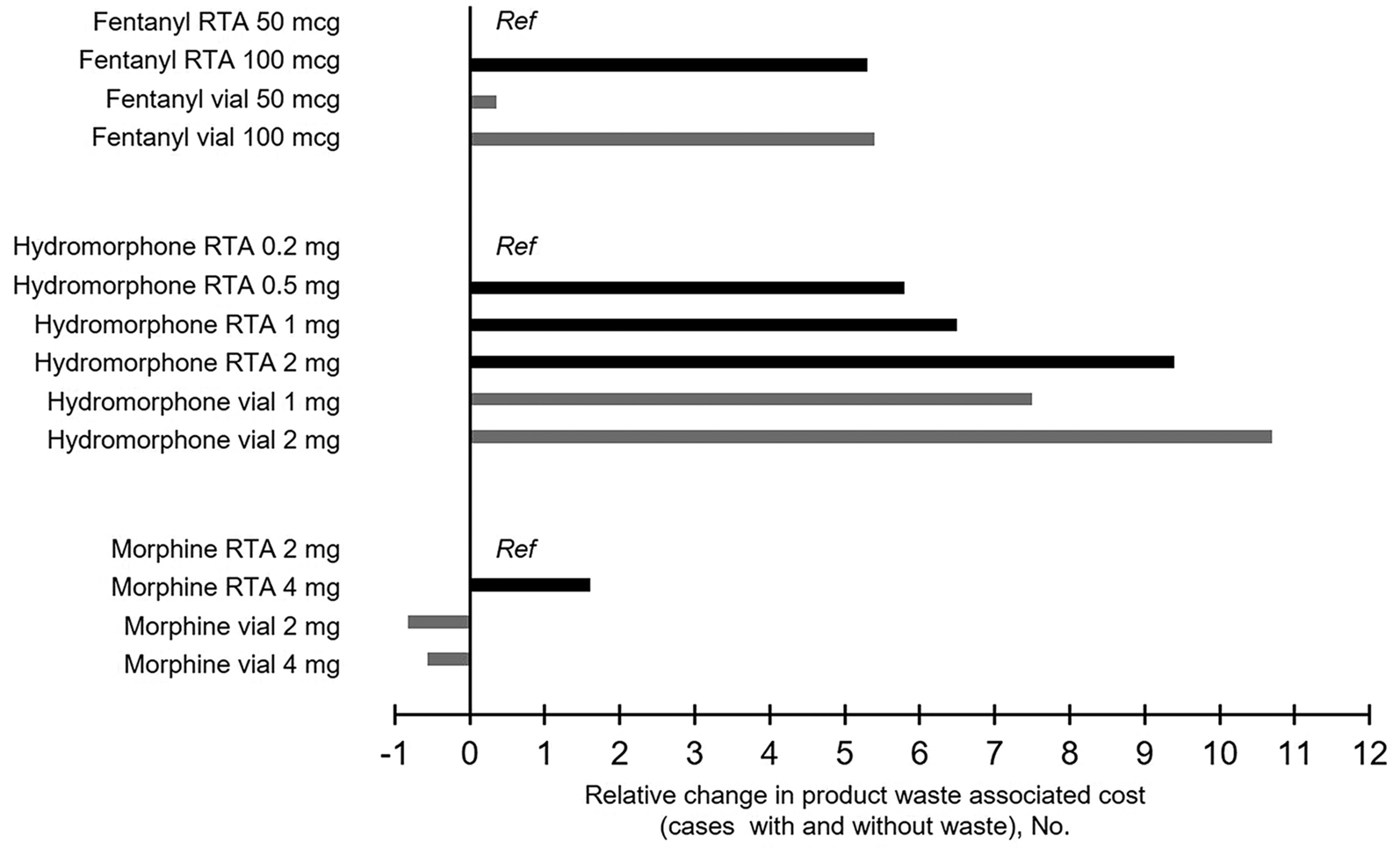
Data on opioids administered intraoperatively to patients undergoing general anesthesia were retrospectively collected from January 2010 to June 2020. In addition, data on actual intraoperative opioid product waste were available from the hospital controlled substance dispensing system records (Omnicell, Mountain View, CA, USA) between June 5, 2020, and June 15, 2022. Hypothetical estimates of intraoperative opioid product waste were calculated based on available ready-to-administer (RTA) syringe sizes as the difference between the syringe size (or multiples of the syringe size) and the actual dose of opioid administered. Specifically, RTA syringe sizes of 50 mcg and 100 mcg were used for fentanyl; 0.2 mg, 0.5 mg, 1 mg, and 2 mg for hydromorphone; and 2 mg and 4 mg for morphine. Hypothetical estimates of product waste were also predicted for the following vial sizes: fentanyl 50 mcg and 100 mcg; hydromorphone 1 mg and 2 mg; morphine 2 mg and 4 mg. We calculated costs associated with product waste, defined as the sum of the cost of the wasted syringe or vial and the cost of skilled labor needed to discard the product. A loss of provider time of 76.2 s to report the waste for syringes was assumed [4]. An additional time of 60 s was assumed to report the waste for vials and to account for the time for vial drawing up. The cost of provider time was calculated on a median hourly wage for nurse anesthetists of $94.04, as estimated by the US Bureau of Labor Statistics [8]. The cost of medications is the average wholesale price (AWP) in the USA and is expressed as US dollars ($) [9].
Identification of Independent Predictors of Opioid WasteConfounder Model and Outcome Measure
Based on literature review and clinical plausibility, the following variables were evaluated as predictors of intraoperative opioid waste: age, sex, ethnicity and race, ideal body weight, ASA physical status, Charlson Comorbidity Index (CCI) [10], score for prediction of postoperative respiratory complications (SPORC) [11], admission type, source of admission, outpatient use of opioids within 90 days before surgery, year of surgery, duration of anesthesia, emergency surgery, anesthesia technique, and age-adjusted minimum alveolar concentration; use of succinylcholine, non-depolarizing neuromuscular blocking agents, neostigmine, or sugammadex; total volume of intravenous fluids, red blood cell transfusions, vasopressor requirements, and duration of intraoperative hypotension (minutes of mean arterial pressure below 55 mmHg). Further, number of opioids used, individual opioids administered, and use of remifentanil were included, as well as the use of non-opioid adjuvants, such as premedication with oral acetaminophen and/or gabapentinoids, and intraoperative use of ketamine, lidocaine, non-steroidal anti-inflammatory drugs (NSAIDs), magnesium, esmolol, or dexmedetomidine. Lastly, the provider type (i.e., nurse anesthetist, resident, or attending anesthesiologist) was included.
We defined occurrence of product waste as the discrepancy between the actual dose administered and an aliquot (or the combination of multiple available aliquots) of 50 mcg for fentanyl, 1 mg for hydromorphone, and 4 mg for morphine, which represents the current syringe sizes at BIDMC.
Statistical Analyses
A multivariable logistic regression model was built to assess independent predictors of intraoperative opioid waste. Stepwise elimination was performed for variables with a P value > 0.01, and bootstrapping with 1000 replications was used to confirm the appropriate identification of predictors. The relative importance of each predictor was assessed through dominance analysis [12].
Intraoperative Opioid Dose and Clinical Adverse OutcomesExposure and Outcome Measures
The primary exposure was the intraoperative opioid dose, categorized as follows: fentanyl > 0–50 mcg, > 50–100 mcg, and > 100 mcg; hydromorphone > 0–0.5 mg, > 0.5–1 mg, and > 1 mg; and morphine > 0–2 mg, > 2–4 mg, and > 4 mg. Opioid categories were chosen according to available RTA syringes or their clinically reasonable combinations. In patients receiving more than one opioid, the total doses of the additional opioids were considered as confounders.
Outcomes were defined in accordance with NCC MERP categories [6]. The primary outcome was the occurrence of any safety events that resulted in temporary harm to the patient and required intervention, including post-extubation desaturation, postoperative nausea or vomiting needing rescue treatment in the post-anesthesia care unit (PACU), and postoperative somnolence or sedation needing nursing observation or administration of naloxone (Category E). The secondary outcomes were defined as (a) harm to the patient that required hospitalization, investigated only in outpatients, represented by delayed discharge from post-anesthesia care unit (length of stay ≥ 120 min), unplanned admission (booked outpatients who required unplanned admission), or delayed discharge from hospital (length of stay > 75th percentile), and readmission within 30 days after hospital discharge (Category F); (b) permanent patient harm, including cardiac arrest and stroke within 7 days postoperatively (Category G); and (c) need for interventions necessary to sustain life: unplanned intubation or intensive care unit admission (all-cause) within 7 days postoperatively (Category H).
Confounder Model
All analyses were adjusted for a priori-defined confounding variables based on literature review and clinical plausibility. These variables included patient demographics such as age, sex, body mass index, and ASA physical status, as well as comorbidities, including chronic heart failure, preoperative drug abuse, obstructive and restrictive lung disease, obstructive sleep apnea, and smoking status. Further, the CCI [10] and SPORC [11] were considered as confounding variables. Case-specific confounders, such as surgical specialty, emergency status, duration of surgery, work relative value units, and year of surgery, were included. Analyses were further adjusted for intraoperative and anesthesia-related factors, including the use of adjunct analgesic or sedative medications (ketamine, dexmedetomidine, regional anesthesia), age-adjusted mean alveolar concentration of inhalational anesthetics, use of neuromuscular blocking agents (non-depolarizing agents and succinylcholine), reversal agents (neostigmine and sugammadex), total volume of intravenous fluids administered, red blood cell transfusions, vasopressor requirements, duration of intraoperative hypotension (minutes of mean arterial pressure < 55 mmHg), ventilation parameters (fraction of inspired oxygen, positive end-expiratory pressure, peak inspiratory pressure, tidal volume), number of anti-emetic medications, and Apfel score [13].
Exploratory Analysis
In an exploratory intent, we investigated the association between the amount of opioids wasted and the primary outcome (Category E).
Statistical Analyses
In the primary analysis, we assessed the association between the categorized dose of each opioid agent and the primary outcome. A multivariable logistic regression model adjusted for the previously mentioned confounders was used. Statistical models, study endpoints, and confounding variables were defined a priori. Potential multicollinearity between confounding variables and the primary exposure was assessed using the variable inflation factor and coefficients of correlation matrix. Continuous confounding variables were categorized into quintiles or clinically relevant categories. All the analyses were performed using Stata software (version 16.0, StataCorp LLC, College Station, TX, USA).


留言 (0)