
記住我





Obesity, diabetes, and CKD are highly prevalent, commonly co-occur, and substantially increase cardiovascular disease morbidity and mortality. The mechanisms of these four disease states also are closely intertwined, with multidirectional relationships, shared risk factors, and common therapeutic targets. Given the complex interactions among these diseases, the American Heart Association (AHA) recently proposed a new integrated health disorder, the cardiovascular-kidney-metabolic (CKM) syndrome, defined as a health disorder attributable to connections among obesity, diabetes, CKD, and cardiovascular disease.1,2
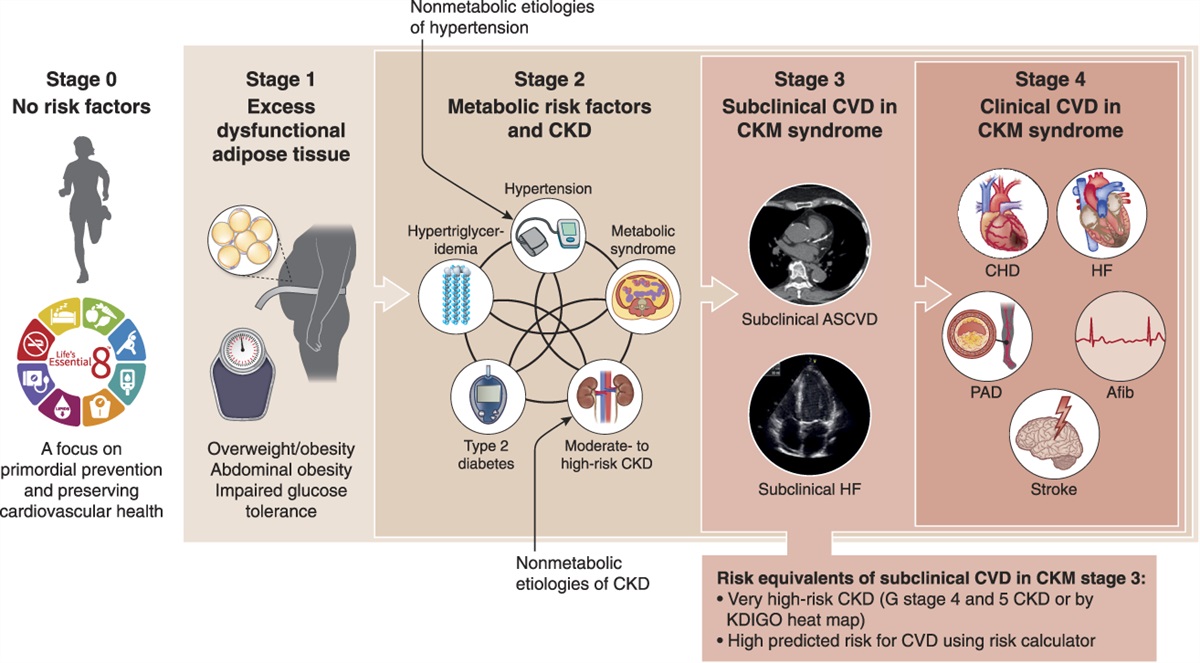
The CKM framework aims to move beyond individual risk factor management, proposing a new integrated systemic staging system for those at risk for, and with, existing cardiovascular disease (Figure 1). This staging system is designed to better reflect the pathophysiology, spectrum of risk, and opportunities for prevention and care optimization within the CKM syndrome. Stage 0 includes individuals who are not overweight/obese and do not have metabolic risk factors (e.g., hypertension, hypertriglyceridemia), CKD, or subclinical/clinical cardiovascular disease. Stage 1 includes individuals who have excess and/or dysfunctional adiposity, as manifested by high body mass index, waist circumference, or fasting blood sugar. Individuals in this stage do not have other metabolic risk factors or CKD. Stage 2 includes individuals with metabolic risk factors (hypertriglyceridemia, hypertension, diabetes) or CKD. Stage 3 includes individuals with subclinical atherosclerotic cardiovascular disease (atherosclerosis or coronary artery calcium) or subclinical heart failure (elevated cardiac biomarkers or echocardiographic parameters) among individuals with excess/dysfunctional adiposity, metabolic risk factors, or CKD. Risk equivalents for subclinical cardiovascular disease include stage G4 or G5 CKD. Finally, stage 4 CKM includes individuals with clinical cardiovascular disease (coronary heart disease, heart failure, stroke, peripheral artery disease, atrial fibrillation) among individuals with excess/dysfunctional adiposity, metabolic risk factors, or CKD.1,2
 Figure 1: Stages of the American Heart Association CKM health syndrome. Reprinted from ref. 1 with permission. AFib, atrial fibrillation; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; CKM, cardiovascular-kidney-metabolic; CVD, cardiovascular disease; HF, heart failure; KDIGO, Kidney Disease Improving Global Outcomes; PAD, peripheral arterial disease.
Figure 1: Stages of the American Heart Association CKM health syndrome. Reprinted from ref. 1 with permission. AFib, atrial fibrillation; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; CKM, cardiovascular-kidney-metabolic; CVD, cardiovascular disease; HF, heart failure; KDIGO, Kidney Disease Improving Global Outcomes; PAD, peripheral arterial disease.Nephrologists have a substantial role in caring for individuals across CKM stages. What does this new framework mean for nephrology and care of kidney disease patients?
Earlier Detection of CKDCardiovascular disease risk factors, including CKD, are often silent and undetected until clinically apparent disease is present. This new staging system emphasizes early detection of cardiovascular disease risk factors, including CKD. The CKM staging recommends assessment of both eGFR and the urine albumin-creatinine ratio in at-risk individuals, defined as those with obesity, hypertriglyceridemia>135 mg/dl, metabolic syndrome, diabetes, hypertension (stage 1 or higher), and those with clinical cardiovascular disease. Notably, this framework calls for albuminuria assessment in CKM stage 1, defined by obesity or dysfunctional adiposity without CKD. We hope that this AHA CKM framework raises awareness of kidney health and promotes screening for kidney disease among primary care and other subspecialty clinicians who are seeing these patients early in the course of disease, as measurement of urinary albumin-to-creatinine ratio (UACR) has remained dismally low despite previous guideline recommendations.3 We also hope that this accelerates implementation of CKD screening more broadly in the United States, including a more expansive recommendation for kidney disease screening as currently being considered by the US Preventative Services Task Force. Earlier detection and screening for CKD using both eGFR and UACR in individuals at even low or moderate risk may substantially delay or prevent progression of CKD, increase life-years and quality of life, and reduce health care costs.4,5
Kidney Disease across the LifespanKidney disease is not just a disease affecting older adults. As the incidence of metabolic diseases and obesity increases in younger individuals and children, greater guidance is needed on how and when to screen for complications such as CKD. The CKM proposes screening for CKD in early life (age <21 years) with risk factors such as obesity, hypertriglyceridemia, diabetes, or hypertension. Earlier detection of CKD in younger individuals could have substantial impact on lifetime survival and quality of life.6
Focus on CKD Severity, Including Patients Treated with DialysisUntil now, outside of nephrology guidelines, CKD has largely been treated as a single entity, with less attention to patients with kidney failure treated with dialysis. With the CKM framework, individuals with CKD stage G4 and G5 by the Kidney Disease Improving Global Outcomes staging system are considered risk equivalents for subclinical cardiovascular disease, resulting in a designation of at least stage 3 CKM. In stage 4 CKM, patients with kidney failure treated with dialysis are separated from those without kidney failure because of the substantial cardiovascular risk and the unique approaches to risk factor management and treatment (in the context of a lack of quality data to guide treatment decisions).
Consideration of Kidney Function in Guideline-Directed Medical TherapyGuideline-directed medical therapy therapies, such as renin-angiotensin-aldosterone inhibitors, mineralocorticoid receptor antagonists, sodium-glucose cotransporter-2 inhibitors, and glucagon-like peptide-1 receptor agonists, remain underutilized in patients with or at risk for cardiovascular disease and CKD despite strong evidence that they improve cardiovascular disease outcomes and slow the progression of CKD.7 There remain substantial barriers in initiation of these medications (in part due to social determinants of health [SDOH]), with patients who are most likely to benefit being less likely to receive these therapies.8 In addition, some of these therapies may have short-term hemodynamic effects on kidney function or have higher rates of adverse effects in individuals with CKD, which can lead to premature discontinuation of these therapies. The CKM treatment approach encourages initiation and continuation of these important therapies in patients with CKD, which is a current barrier in implementation and extends beyond nephrology. There is a critical need for trials to evaluate implementation strategies to increase uptake of guideline-directed medical therapy in patients with CKD, including the pace of initiation and titration.
New Risk Score for Cardiovascular Disease That Includes Kidney FunctionPrevious cardiovascular disease risk scores have not typically included eGFR and albuminuria as prediction variables. The new CKM Predicting Risk of CVD EVENTs (PREVENT) prediction model includes traditional cardiovascular disease risk factors (age, total cholesterol, non-HDL and HDL cholesterol, systolic BP, diabetes, current smoking, hypertension medications, and statins) and eGFR as predictors, with additional models tailored for high-risk individuals with inclusion of UACR when available.9,10 If this new model gets implemented into practice, this would prompt earlier and wider measurement of eGFR and UACR. In addition, the new PREVENT model predicts total cardiovascular disease, including risk of heart failure in addition to atherosclerotic cardiovascular disease. This is an important addition for patients with CKD in whom the excess rates of heart failure are comparable with (or even exceed) that of atherosclerotic cardiovascular disease. Furthermore, this new risk equation does not include race as a variable, therefore aligning with the most recent race-free eGFR equations.
Social Determinants of HealthSDOHs are highly prevalent in patients with CKD and are strongly linked with higher risk of CKD and cardiovascular disease. However, there remain significant gaps in identifying SDOHs in our patients. The CKM PREVENT risk score proposes additional models that incorporate SDOHs and a social deprivation index. This is a step forward in recognizing the shared importance of SDOHs with biological risk factors; hopefully that will lead to more systematic interventions.
Patient EducationMany people with kidney disease are unaware of their diagnosis; this may be due to lack of symptoms or ineffective communication and education. This new CKM framework may help start important conversations about kidney health (e.g., prevention and treatment) in individuals at risk or with CKD from health care professionals outside of nephrology.
Interdisciplinary Care ModelsThe AHA CKM framework encourages value-based approaches to interdisciplinary care to reduce the fragmentation and inequitable access to therapies that may occur in individuals with overlapping CKM conditions. The CKM statement suggests that the interdisciplinary CKM team would be supported by a coordinator and includes representation from primary care, cardiology, nephrology, endocrinology, pharmacy, and nursing, as well as care navigators, social workers, or community health workers. In addition, targeted referrals to subspecialists to activate additional expertise are recommended to higher-risk patients with CKM syndrome. The principles espoused here are appropriate; however, marked shifts in health care models, particularly in the United States where payers seldom take multiyear perspectives, would need to occur for the financial aspects of a CKM value-based care model to be implemented widely.
Next Steps: Putting the AHA CKM into PracticeThe AHA's CKM framework places kidney health in the center of this new syndrome, bringing attention to the often-overlooked public health impact of kidney disease. This is an important advance for the nephrology community and provides a new opportunity to forge strong partnerships with other clinicians to advance the care of patients with or at risk of CKD by integrating care for kidney disease, cardiovascular disease, diabetes, obesity, and other metabolic risk factors. We are hopeful that this new framework will lead to changes in guidelines to implement broader screening for CKD, greater implementation of newer kidney and cardiovascular disease protective therapies among patients with CKD, and motivate greater propagation of collaborative care models. Furthermore, we hope that the CKM framework accelerates research in the field, including greater investigation of etiologies of CKD in patients with metabolic disease and cardiovascular disease to guide disease-specific treatments; research across the spectrum of CKD severity (including dialysis patients); and broader inclusion of patients with CKD in cardiovascular disease clinical trials.
DisclosuresN. Bansal reports consultancy for AstraZeneca, advisory or leadership role as an Kidney360 Associate Editor and an UpToDate Section Editor, and advisory or leadership role for American College of Physicians. M. Sarnak reports consultancy on the Steering Committee of Trials Funded by Akebia, consultancy for Boehringer Ingelheim (attended an Advisory Board), and research funding from NIH. M. Sarnak's spouse reports employment with and ownership interest in Eli Lilly. D. Weiner reports employment with Tufts Medical Center Physicians Organization; research funding from Bayer (site PI), Cara (site PI), and Vertex (site PI), with all compensation paid to Tufts MC; advisory or leadership role as Co Editor-in-Chief of NKF Primer on Kidney Diseases 8th Edition, Editor-in-Chief of Kidney Medicine, Medical Director of Clinical Research for Dialysis Clinic Inc., Member of ASN Quality and Policy Committees and ASN representative to KCP, and Member of Scientific Advisory Board for National Kidney Foundation; and other interests or relationships as Member of Safety and Clinical Events Committee for “A Prospective, Multi-Center, Open-Label Assessment of Efficacy and Safety of Quanta SC+ for Home Hemodialysis” Trial (Avania CRO) and Member of Adjudications Committee for ProKidney REACT Trial (WCG Clinical CRO).
FundingNone.
AcknowledgmentsThe content of this article reflects the personal experience and views of the author(s) and should not be considered medical advice or recommendation. The content does not reflect the views or opinions of the American Society of Nephrology (ASN) or JASN. Responsibility for the information and views expressed herein lies entirely with the author(s).
Author ContributionsConceptualization: Nisha Bansal, Mark Sarnak, Daniel Weiner.
Writing – original draft: Nisha Bansal.
Writing – review & editing: Nisha Bansal, Mark Sarnak, Daniel Weiner.
References 1. Ndumele CE, Rangaswami J, Chow SL, et al.; American Heart Association. Cardiovascular-kidney-metabolic health: a presidential advisory from the American Heart Association. Circulation. 2023;148(20):1606–1635. doi:10.1161/cir.0000000000001184 2. Ndumele CE, Neeland IJ, Tuttle KR, et al.; American Heart Association. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation. 2023;148(20):1636–1664. doi:10.1161/cir.0000000000001186 3. Chu CD, Xia F, Du Y, et al. Estimated prevalence and testing for albuminuria in US adults at risk for chronic kidney disease. JAMA Netw Open. 2023;6(7):e2326230. doi:10.1001/jamanetworkopen.2023.26230 4. Cusick MM, Tisdale RL, Chertow GM, Owens DK, Goldhaber-Fiebert JD. Population-wide screening for chronic kidney disease: a cost-effectiveness analysis. Ann Intern Med. 2023;176(6):788–797. doi:10.7326/m22-3228 5. Garcia Sanchez JJ, James G, Carrero JJ, et al. Health care resource utilization and related costs of patients with CKD from the United States: a report from the discover CKD retrospective cohort. Kidney Int Rep. 2023;8(4):785–795. doi:10.1016/j.ekir.2023.01.037 6. Kula AJ, Prince DK, Katz R, Bansal N. Mortality burden and life-years lost across the age spectrum for adults living with CKD. Kidney360. 2023;4(5):615–621. doi:10.34067/kid.0000000000000097 7. Neuen BL, Heerspink HJL, Vart P, et al. Estimated lifetime cardiovascular, kidney and mortality benefits of combination treatment with SGLT2 inhibitors, GLP-1 receptor agonists, and non-steroidal MRA compared with conventional care in patients with type 2 diabetes and albuminuria. Circulation. 2024;149(6):450–462. doi:10.1161/circulationaha.123.067584 8. Lamprea-Montealegre JA, Madden E, Tummalapalli SL, et al. Prescription patterns of cardiovascular- and kidney-protective therapies among patients with type 2 diabetes and chronic kidney disease. Diabetes Care. 2022;45(12):2900–2906. doi:10.2337/dc22-0614 9. Khan SS, Coresh J, Pencina MJ, et al.; American Heart Association. Novel prediction equations for absolute risk assessment of total cardiovascular disease incorporating cardiovascular-kidney-metabolic health: a scientific statement from the American Heart Association. Circulation. 2023;148(24):1982–2004. doi:10.1161/cir.0000000000001191 10. Khan SS, Matsushita K, Sang Y, et al.; Chronic Kidney Disease Prognosis Consortium and the American Heart Association Cardiovascular-Kidney-Metabolic Science Advisory Group. Development and validation of the American Heart Association's PREVENT equations. Circulation. 2024;149(6):430–449. doi:10.1161/circulationaha.123.067626
留言 (0)