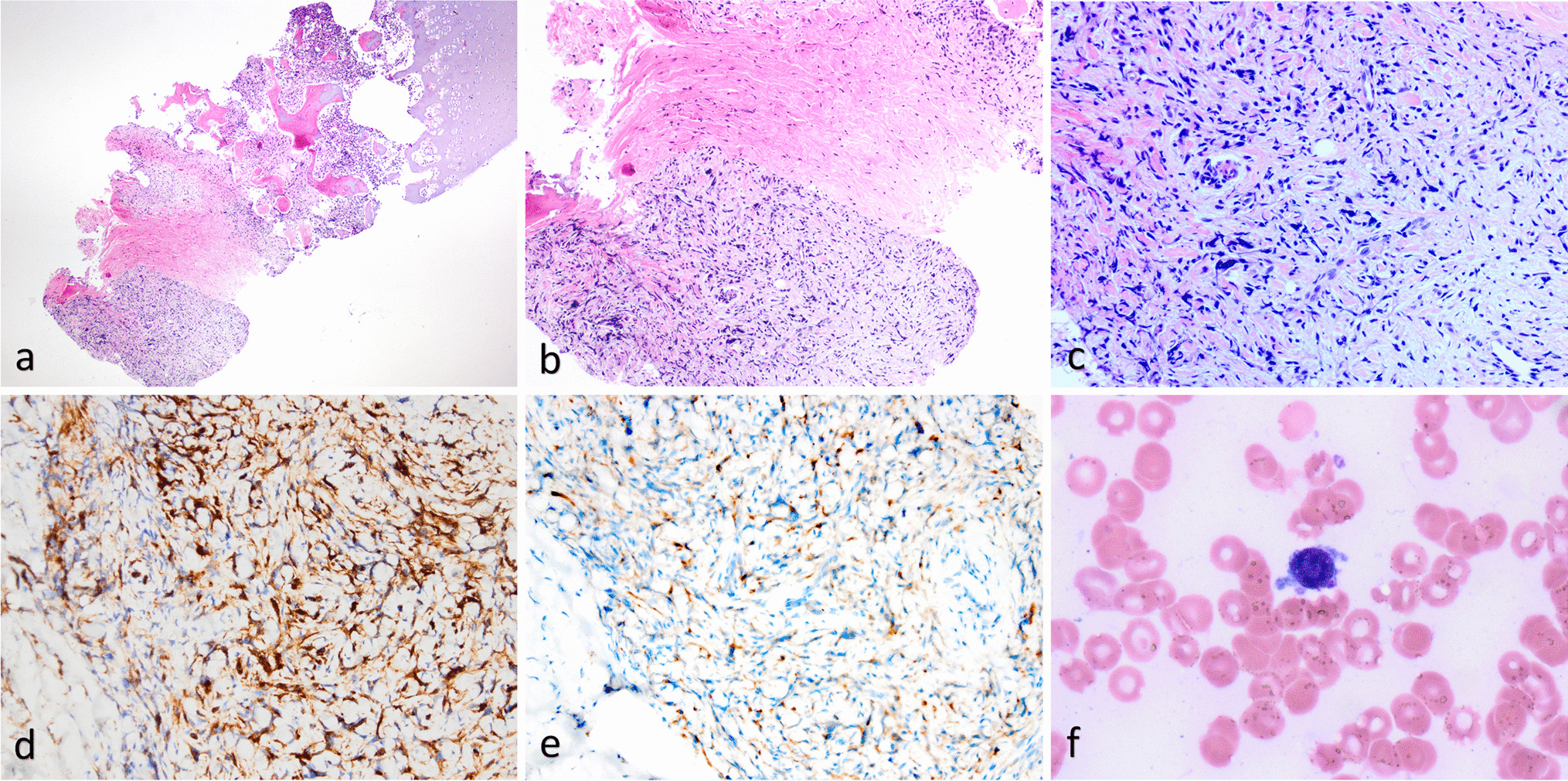
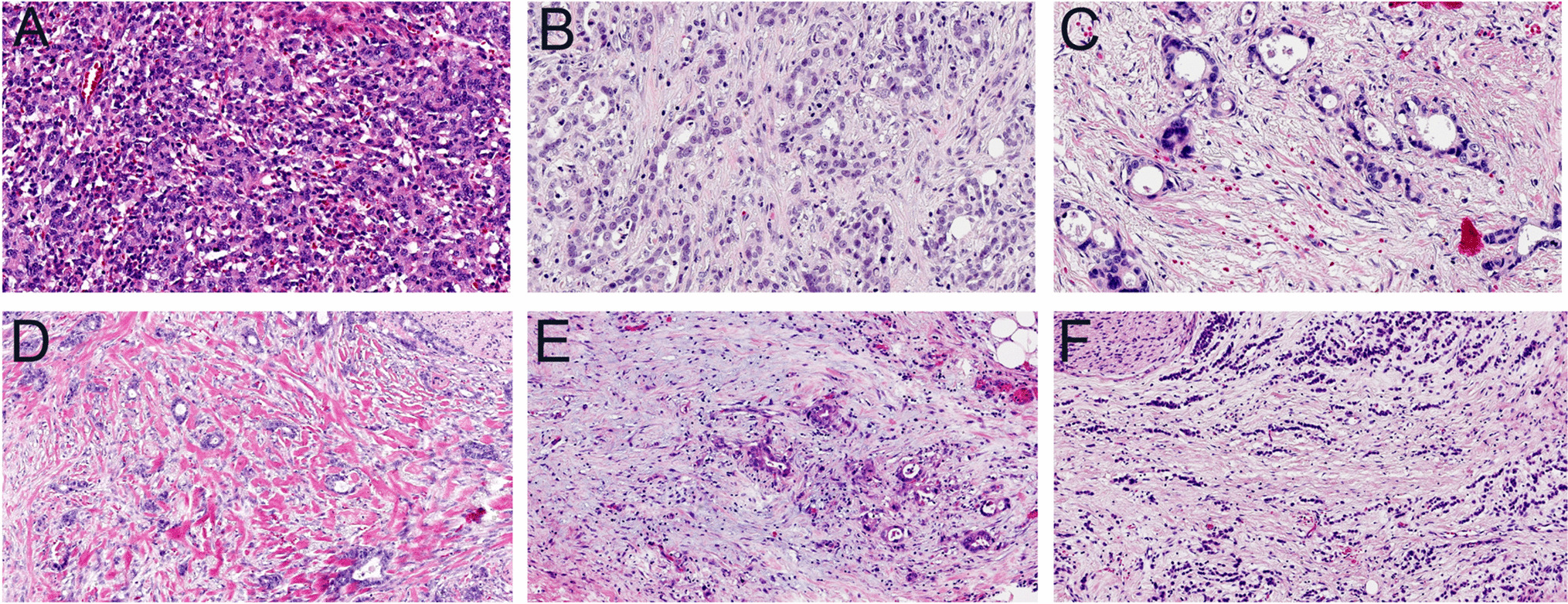
SC-SCC is a rare variant that represents approximately 1–2% of all SCCs [6]. Most cases present as polypoid and pedunculated lesions, and, according to our study, in a significant proportion of cases, they may have a histologic appearance that closely resembles granulation tissue, thus requiring careful differential diagnosis.
In the larynx, benign lesions with granulation tissue appearance are relatively common and are altogether designated as vocal cord granulomas [9]. These lesions are found in association with gastroesophageal reflux, intubation trauma, and vocal abuse [9]. Vocal cord granuloma may affect one or both vocal cords, and in most cases, it is located in the posterior portion at the vocal process of the arytenoid, and less frequently in the middle third or the anterior portion [9]. In the present series, SC-SCC showed a different localization, with lesions mainly involving the anterior and mid vocal cord, while the vocal process of the arytenoid was never involved, and no case showed bilateral involvement. Histologically, vocal process granuloma is a polypoid lesion with a hyperplastic or ulcerated epithelial surface. The core of the lesion is represented by granulation tissue with acute and chronic inflammatory cells, abundant capillary vessels, and fibrotic changes, that become predominant with the aging of the lesion [10,11,12]. The distinction from SC-SCC may be difficult, and it is based on the absence of squamous dysplasia or carcinoma in situ of the overlying epithelium, as well as on the absence of nests of invasive conventional SCC or atypical cells within the core of the lesion.
In the tongue, which is the second most frequent site affected by SC-SCC in our series, the initial clinical impression was granulation tissue or lobular capillary hemangioma (pyogenic granuloma). The latter presents as a polypoid lesion with epithelial collarette and often ulcerated surface, and lobular arrangement of the proliferating vessels. Each lobule presents a central large vein encircled by several capillaries. Cellularity is often high, and mitotic activity may be brisk, but atypia is absent both in the residual surface epithelium and within the lesion.
SC-SCC with granulation tissue-like appearance must also be distinguished from inflammatory myofibroblastic tumor (IMT). This is a polypoid proliferation of fibroblasts and myofibroblasts accompanied by an inflammatory infiltrate of plasma cells, lymphocytes, and eosinophils, that may involve different mucosal sites in the head and neck. The differential diagnosis with SC-SCC is based on the absence of invasive or in situ SCC component. The immunohistochemical profile may show some overlap with that of SCC, including positivity for cytokeratins, actins, and desmin. However, IMT is also positive for ALK1 [13, 14] while in the present study all tested SC-SCC were negative. In addition, IMT harbors ALK gene rearrangements in 50–70% of cases, that may be useful in the differential diagnosis [15]. In recent studies, genuine IMTs of the head and neck are virtually all ALK-positive and/ or rearranged [16].
The presence of a prominent vascular component associated with atypical cells in granulation tissue-like SC-SCC brings into the differential diagnosis the possibility of a malignant vascular neoplasm, mainly Kaposi sarcoma and angiosarcomas. Involvement of head and neck mucosal sites is rare in Kaposi sarcoma and is almost exclusively observed in HIV patients [17,18,19]. Immunohistochemical positivity for HHV8 is the key diagnostic feature. Angiosarcoma is rare at mucosal sites of the head and neck and involves more frequently the oral cavity and the sinonasal tract, while the larynx is only exceptionally involved, often after previous radiotherapy [20,21,22,23]. The distinctive features include absence of carcinoma (in situ or invasive) and presence of tortuous and anastomosing vascular channels lined by atypical endothelial cells, which are positive for CD34, CD31, and ERG.
In this diagnostic setting, immunohistochemistry may be helpful, but it should be considered that in SC-SCC cytokeratin expression is usually decreased with the loss of epithelial differentiation, and in some cases cytokeratin expression may be lost entirely [6, 7]. Among cytokeratin markers, CK18 proved most valuable in “keratin-shy” cases [6]. Antibodies to p63 and p40 are widely used in the identification of poorly differentiated SCC and sarcomatoid carcinomas in a variety of organs, including head and neck sites [24, 25]. P53 positivity and gene mutations have been reported in SC-SCC in both the epithelial and spindle cell components [26]. In our series we observed aberrant immunohistochemical expression of TP53 in all the cases, whereas all benign lesions (granulation tissue polyps) revealed regular expression. Although the sensitivity and specificity of p53 immunostaining in this context must be further investigated, our study indicates that p53 aberrant expression could be a strong support in the diagnosis of granulation-tissue like SC-SCC, helping in the distinction from benign mimickers.
In summary, we describe the clinicopathologic features of a series of 17 cases of head and neck SC-SCC with granulation tissue-like appearance. This histologic pattern may be explained by the presence of ulcer of the surface epithelium that induces marked inflammation and proliferation of capillaries. Such changes may be so intense and diffuse to obscure the underlying neoplastic component, and thus careful differential diagnosis with benign lesions, including granulomas and vascular lesions, is mandatory. These tumors are often initially misdiagnosed, and in case of recurrence of a granulation tissue polyp of the upper aerodigestive tract mucosa, the possibility of a granulation tissue-like SC-SCC should be considered. Immunohistochemistry often cannot identify epithelial differentiation, but this should not preclude the diagnosis of SC-SCC, especially if there is evidence of dysplasia or carcinoma in situ of the adjacent surface epithelium. Evaluation of p53 immunohistochemical expression may be a most useful adjunct to distinguish these carcinomas from benign mimickers.


留言 (0)