
記住我

The primary goal of this study is to test the hypothesis that the Na+, K+, and water content in the skin, is altered in PA, the prototype of salt-dependent hypertension. We will also test the hypothesis that these alterations are corrected by surgical cure of PA. Additional goals are to determine if there is more Na+ and less K+ deposition in PA patients as compared to hypertensive patients without PA, and to healthy normotensive controls and if these changes are associated with altered expression of Tonicity-responsive Enhancer Binding Protein (TonEBP, NFAT5) mRNA copy number, taken as an index of tissue osmotic stress. Besides TonEBP expression, also its cellular localization (cytoplasmic or nuclear), and the resulting protein expression will be assessed. To this end, molecules involved in the VEGF-C/VEGFR3/ERK-AKT pathway will be quantified as indicators of enhanced neo-lympho-angiogenesis [5].
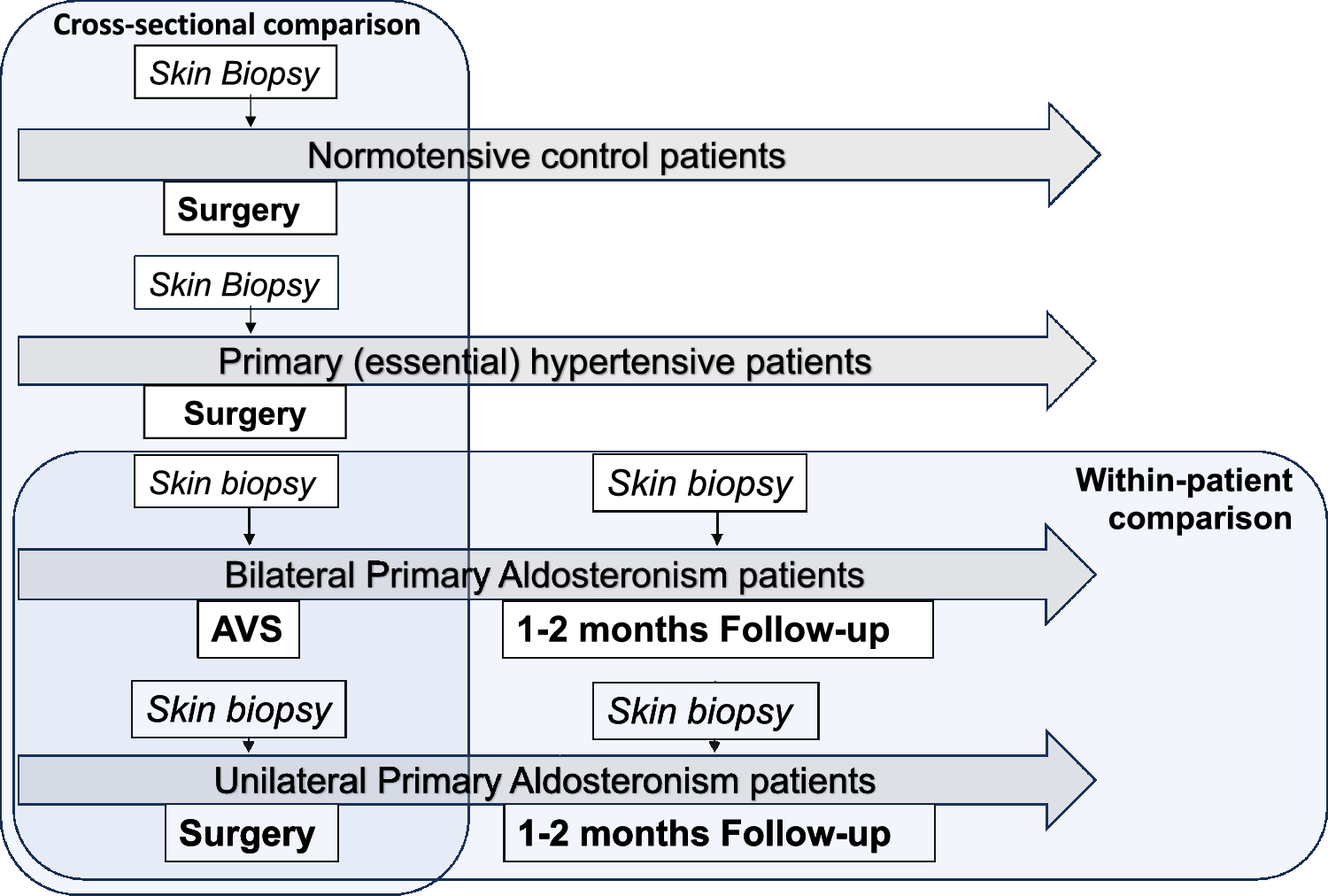
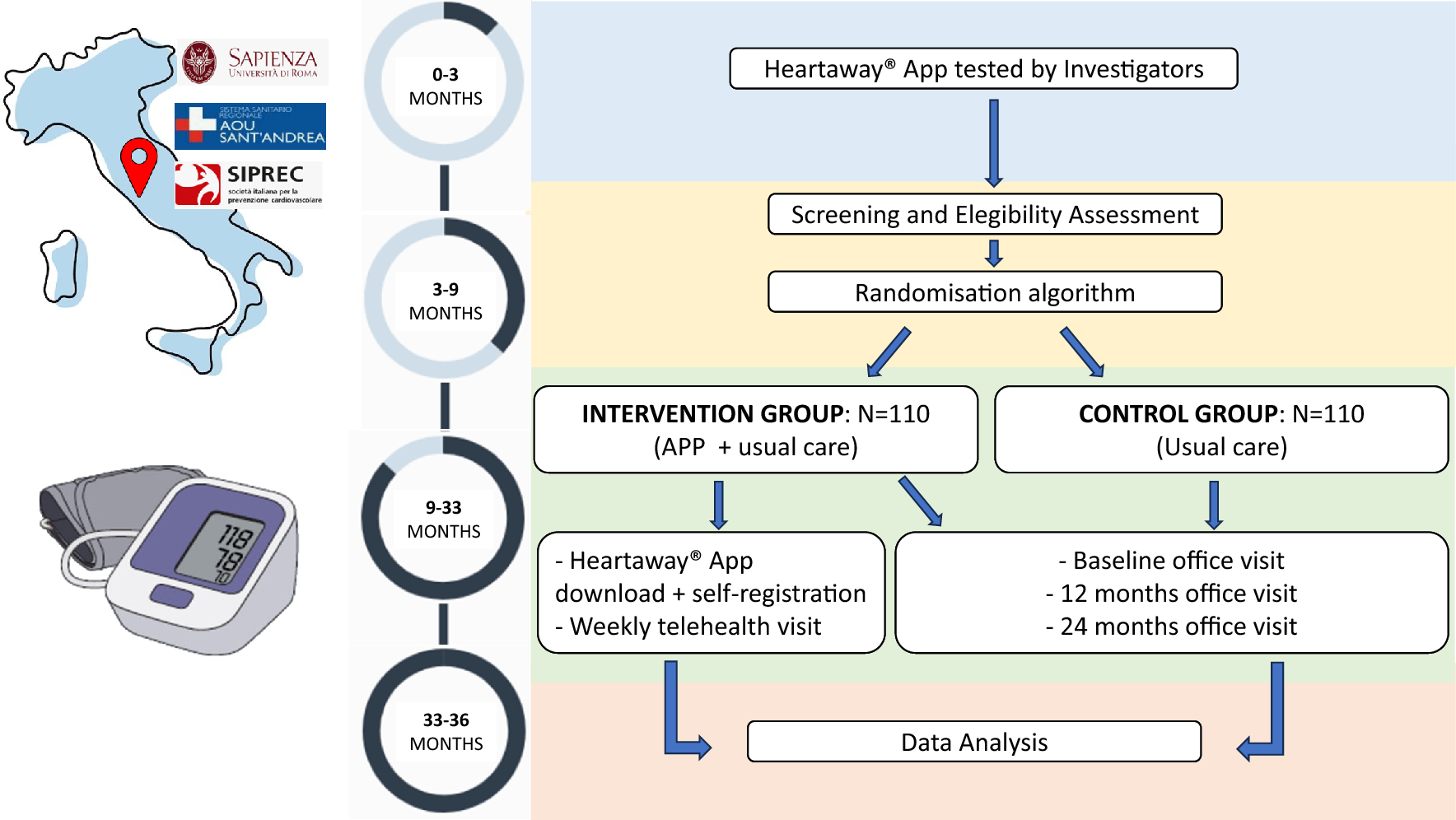
2.2 Study DesignThis study was conceived as a within-patient prospective observational clinical study. Its schematic layout is shown in Fig. 1 along with its primary endpoints. Four study arms will be considered: (1) PA group 1: conclusive diagnosis of unilateral PA (uPA); (2) PA group 2: presumed diagnosis of bilateral PA (bilPA) [7]; (3) PH Group 3: primary (essential) hypertension (PH); (4) Group 4: normotensive control patients undergoing surgery for benign conditions other than cardiovascular disease.
Fig. 1
The scheme illustrates the study design and the Groups of patients who will be recruited for the within-patient and cross-sectional comparison of electrolytes, water and NFAT5 (TonEBP) content in the skin. AVS adrenal veins sampling, uPA unilateral primary aldosteronism, bPA bilateral primary aldosteronism, PHT primary (essential) hypertension, NT normotensive patients
In Group 1, to investigate the effect of uPA cure, the Na+, K+, and water skin content in the biopsy obtained during adrenalectomy will be within-patient compared to that obtained one month after adrenalectomy. In Group 2 comprising bilPA patients, the first biopsy obtained during AVS (adrenal vein sampling) will be compared to that obtained after one month of continued medical treatment with an unchanged dose of canrenone. The hypertensive patients in Group 3 and the normotensive patients in Group 4 will be used for a cross-sectional comparison of electrolytes, water and mRNA content with the PA patients in Groups 1 and 2.
All procedures will be performed according to good clinical practice and to the Declaration of Helsinki and the study will start after approval of the Ethics Committee of the University of Padova.
2.3 Inclusion CriteriaWe will recruit consecutive consenting patients, aged from 18 to 75 years, with known arterial hypertension and/or treatment with antihypertensive drugs, as confirmed by daytime ambulatory BP monitoring (ABPM) or home blood pressure measurement. For ABPM the cutoff values will be < 130/80 mmHg; for home BP they will be ≥ 140 mmHg for systolic and/or ≥ 90 mmHg for diastolic.
PA will be diagnosed according to current guidelines [6] based on plasma aldosterone concentration (PAC) > 15 ng/dL and aldosterone/renin ratio greater (ARR) than 20.6 ng/mIU, while on a 100–300 mEq daily Na+ intake, as verified by 24-h urinary Na+ excretion. To achieve wash-out of interfering drugs, PAC and renin will be measured after drug treatment switch. PA will be diagnosed as unilateral (uPA) or bilateral (bilPA) based on adrenal vein sampling, as described [8] .
The uPA patients will be treated with adrenalectomy of the culprit adrenal gland and reassessed at follow-up after surgical cure and MRA withdrawal. Normalization of PAC and the ARR will be used to confirm biochemical cure. The bilPA patients will also be reassessed at follow-up while they will continue MRA treatment (Fig. 1).
Primary (essential) hypertension patients forming the PH Group will be enrolled after exclusion of PA or any other secondary form of hypertension, as described in detail [9].
Consenting healthy patients of similar age with normal arterial blood pressure values and no use of any anti-hypertensive drugs will be recruited.
2.4 Exclusion CriteriaThe main exclusion criteria will be: (1) history of allergy/intolerance to local anesthesia; (2) refusal of the patient to undergo skin biopsy; (3) refusal of the patient to undergo AVS, and/or contraindications to the general anesthesia (required for laparoscopic adrenalectomy) and/or to undergo adrenalectomy, if indicated; (4) cortisol–aldosterone co-secreting adenoma or any forms of secondary HT other than PA. Additional exclusion criteria are listed in Table 1.
Table 1 Main and additional exclusion criteria2.5 Skin Biopsy ProcedureIn the patients with PA, the skin biopsy will be performed either during AVS or during adrenalectomy (in Group 1, uPA), and repeated one-month after surgery or continued MRA treatment (in Group 2 bilPA) patients. In the PH patients (Group 3 PH) and in the normotensive control patients (Group 4) the skin biopsy will be done only once during surgery for benign diseases (Fig. 2).
Fig. 2
The cartoon illustrates the skin biopsy specimen collection and their subsequent different storage strategy for each sample, before analysis of electrolytes, water and NFAT5 (TonEBP) content. AAS atomic absorption spectrometry, ddPCR droplet digital polymerase chain reaction
Skin biopsies will be obtained using a disposable sterile biopsy punch (KAI MEDICAL BP-40F, ø 4 mm) at the beginning of the procedure with the utmost care to prevent contamination with Na+ and K+ containing agents. To this end, we will use chlorhexidine and alcohol-based solution (such as NEOXINAL and FARVICETT, Nuova Farmec Srl) to ensure the sterilization of the surgical field. As local anesthetic for the biopsies at follow-up in the outpatient setting, a lidocaine-based cream containing no Na+ or K+ (LMX4 cream, Lidocaine 4%, Ferndale Pharmaceuticals Ltd) will be used. It will be removed with a swift sweep with Na+/K+-free 70% alcohol wipes before performing the procedure.
The collected skin samples will be cut into pieces and stored as follows: the first two samples will be immediately put in a cryo-vial and frozen in liquid nitrogen for electrolyte measurement and biomolecular analysis respectively, while the third piece will be fixed in formalin for histologic analysis (Fig. 2).
We will use physical-chemical methods to measure the Na+, K+, and water content in the skin of patients with PA, primary (essential) hypertension HT patients (PH Group) and in normotensive patients (Control Group). To these aims, all frozen samples will be handled and cut in a cold lab chamber (4 °C) in order to ensure that the samples will be of comparable size before weighting. During this process the cryo-vials (containing the skin samples) will be kept and immediately put back in thermo-insulated cryogenic store boxes containing dry ice to minimize the water loss caused by exposition to open air. They will be then weighed to determine total (WET) weight and then desiccated at 90 °C for 72 h to determine the dry weight (DW). In a set of preliminary experiments, it was previously found that after this period the sample weight remains practically unchanged. Estimated water content will be calculated as difference between total WET and DW.
The measurement of Na+ and K+ in the skin will be carried out as follows: homogenates of dry skin will be suspended overnight in 1N nitric acid to displace Na+ and K+. The supernatant will then be diluted as needed to achieve a concentration that allows analyzing through atomic adsorption spectro-photometer (SpectrAA 50/55 Varian, Agilent), in the proper working range of the machine. Reading of the samples will be done by lamp and wavelength specific to each different element [10].
NFAT5 (TonEBP) mRNA copy number will be assessed by droplet digital PCR (Bio-Rad Laboratories, Segrate, Italy) using the following primers: For: 5′-GAA GTG GAC ATT GAA GGC ACT-3′; Rev: 5′-CTG GCT TCG ACA TCA GCA TT-3′. This technique has already been shown to furnish highly reproducible results as it is based on the absolute count of the gene target abundance, taking advantage of the Poisson statistic that estimates, within the positive droplets (the ones where at least one copy of the target gene is present), the starting copy number of our target gene in terms of copies/µl input sample.
2.6 Potential Confounders2.6.1 Age and SexConsistently with previous animal studies [11], investigation with 23Na-MRI of a cohort entailing 57 patients with HT and 56 normotensive controls [12] reported the skin Na+ to be age- and sex-dependent in all ethnic groups, regardless of the hypertensive or normotensive status, with highest values found in old males. Hence, it seems to be of paramount importance to perform an age- and sex-matched propensity score analysis [13] for these variables (see later).
2.7 DrugsConsidering that antihypertensive drugs, particularly diuretics and blockers of the renin-angiotensin system (RAS), can lower Na+ content in the skin [12], wash-out of possible interfering drugs will be accomplished before studying the patients [14] This will not be applied to the patients diagnosed with PA, who will receive canrenone, for two main reasons: (1) canrenone was shown not to affect the RAS in a prospective study of PA patients [15]; (2) it is necessary to achieve normokalemia and control of the high BP values, e.g. optimal clinical conditions, before the uPA patients are submitted to adrenalectomy[14].
2.8 Sample Size Calculation and Statistical AnalysisBased on the results of a pilot study, which showed a SD of 0.0018 for the Na+/dry weight content in the skin biopsies, we have calculated that 30 surgically treated PA patients and 10 patients with hypertension without PA will be needed to allow detection of a 20% difference between group at a 0.05 alpha (type 1) error with a power of 84% (type II beta error = 16%) using a 2-sided unpaired t-test. Based on the same assumption, we estimated that with use of a paired t-test 15 surgically treated PA patients will be necessary to allow detection of a 20% difference in the Na+/dry weight content in the skin biopsies between baseline and post-surgery, to achieve a statistical power > 95%.
Since this is an observational study prone to the untoward potential effect of confounders on the study endpoints, propensity score matching will be used to minimize the chances of bias when comparing results between uPA and bilPA and between PA patients and PH patients and normotensive patients [13].
留言 (0)