Patients
This study has been registered in China Clinical Trials Registry (http://www.chictr.org.cn) with the registration number of chiCTR1800019966. This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai Pulmonary Hospital, School of Medicine, Tongji University, and all subjects signed an informed consent.
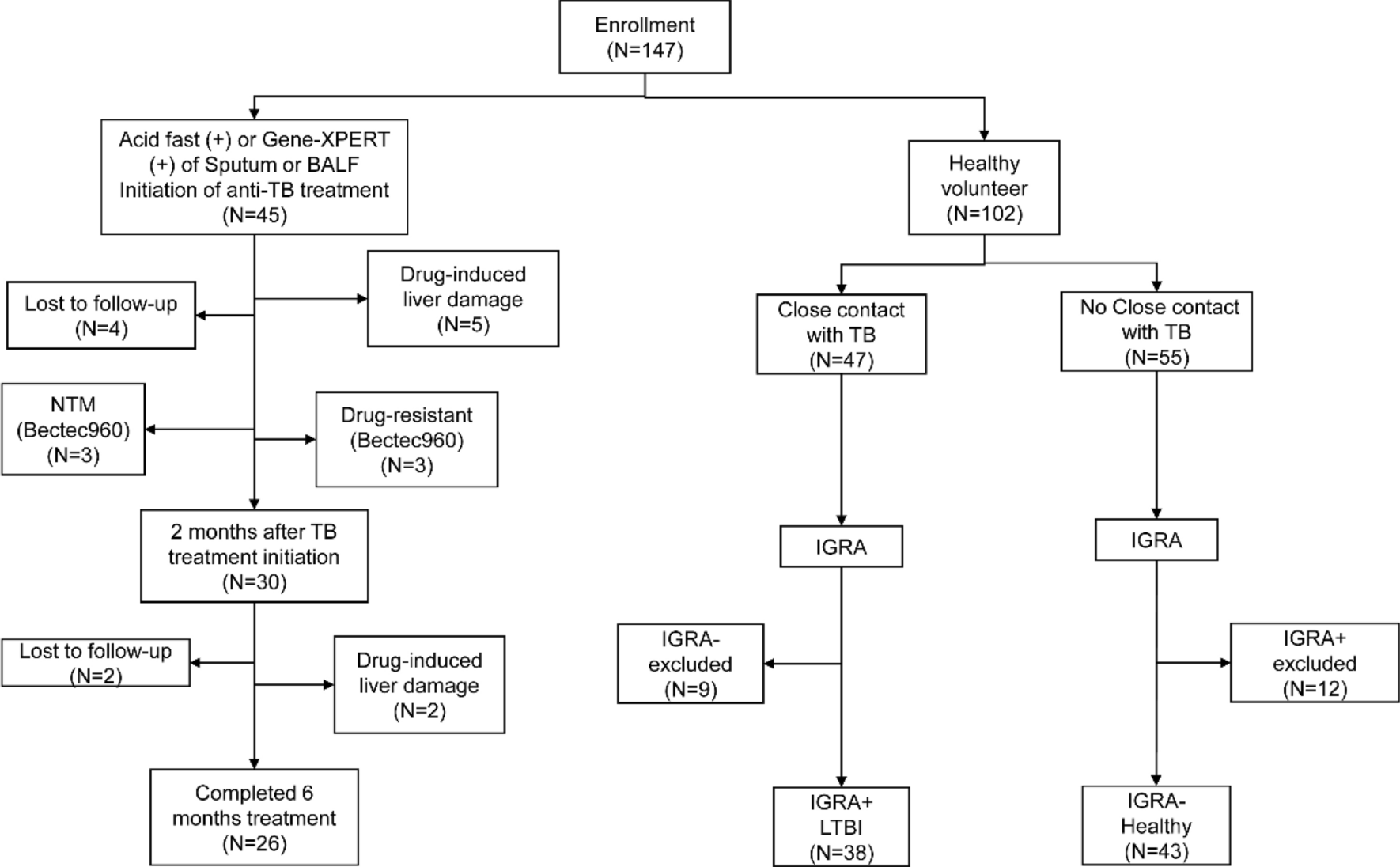
PTB patients, LTBI and healthy control were enrolled at Shanghai Pulmonary Hospital, Shanghai Pulmonary Hospital, School of Medicine, Tongji University from January 2021 to December 2021. The inclusion criteria of PTB patients were (1) newly diagnosed active PTB patients; (2) aged 18–70 years old. The diagnosis criteria of PTB included (1) no previous history of TB; (2) with typical clinical symptoms of TB, such as low-grade fever in the afternoon, night sweats, fatigue, and weight loss; (3) positive in interferon gamma release assay (IGRA) test; (4) positive bacteriological test for TB in sputum, bronchoscopy lavage fluid or lesion tissue, including positive in acid-fast staining and Bectec960 test, or positive in Gene-XPERT test; (5) the lesion site showed typical pathological manifestations of TB, including epithelioid cells, Langhans giant cells, and caseous necrosis; (6) chest CT examination support the diagnosis of PTB; (7) systemic and local anti-TB chemotherapy was effective and (8) other lung diseases were excluded. Among these criteria, the first and fourth ones must be satisfied.
The exclusion criteria were: (1) patients with primary or secondary immunodeficiency, including acquired immune deficiency syndrome (AIDS) patients, long-term use of hormones and patients with autoimmune diseases; (2) diabetic patients; (3) patients with viral hepatitis; (4) patients received anti-TB chemotherapy; (5) Bectec960 test suggesting non-tuberculous mycobacteria (NTM) infection; (6) Bectec960 test suggesting drug resistance.
In addition, LTBI participants and healthy individuals were enrolled as controls. The LTBI participants were enrolled from the close contacts of newly diagnosed TB patients who are IGRA positive and have no clinical evidence of active TB disease. The healthy controls were IGRA-negative healthy volunteers.
Treatment
PTB patients received standard primary anti-TB regimen 2HREZ/4HR [9,10,11,12]. If drug-induced liver injury occurs during the treatment, the drug therapy was stopped and the treatment plan was adjusted.
The acid-fast stain and BECTEC MGIT 960 culture were performed on sputum before and every month after treatment. Computed tomography (CT), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) were examined before treatment, and at 2 and 6 months after treatment. Blood with heparin anticoagulant were extracted, stimulated with TB-specific antigen ESAT-6/CFP-10 for 16 h. The red blood cells were lysed, and then stained with fluorescent antibodies. The IFN-γ/CD4/CD38/CD27 expression were further analyzed using flow cytometry.
CT scan
Lung high-resolution CT scanning were performed with Philips Brilliance iCT256 slice CT scanner (Philips, USA) with patients in a supine position. Scanning parameters were set as follows: tube voltage 120 kV, tube current 50–300 mA, collimator width 128 × 0.625 mm, screw pitch 0.758, matrix 512 × 512, slice thickness 1 mm, spacing 0.5 mm, and field of view 350 mm.
Chest CT severity score
The severity score of lung lesions on chest CT was evaluated by two experienced radiologists from Shanghai Pulmonary Hospital following previous studies [13, 14] according to the distribution of lesions and the extent of involvement. The scores of the two physicians were added up to obtain the CT lung lesion severity score of a patient. Scores were performed before treatment, 2 months after treatment, and at the end of treatment.
ESAT-6/CFP-10 stimulation
Whole blood with heparin anticoagulant was added with 10 μg/ml ESAT-6/CFP-10 polypeptide antigen within 4 h after collection. Golgi transport inhibitor brefeldin A (10 μg/ml, Biolegend, USA) was then added. After mixing, the sample was incubated for 16 h at 37 °C, 5% CO2. Subsequently, 2.5 ml of erythrocyte lysate and fixative (3% diethylene glycol, 2% formaldehyde and 0.75% methanol) was added and incubated at room temperature (25 °C) for 10 min. The cells were centrifuged at 600×g for 5 min, the supernatant was discarded, and 375 µl PerFix-nc (Beckman Coulter, USA) was added. IFN-γ-FITC, CD4-PE, CD3-ECD, CD27-PE-Cy5.5 and CD38-Pe-Cy7 were added and incubated in the dark for 45 min. Then, phosphate buffered saline (PBS) was added and centrifuged at 600×g for 5 min. The supernatant was discarded. The IFN-γ/CD4/CD38/CD27 expression were analyzed using flow cytometry (Beckman Coulter DxFLEX, Beckman Coulter, USA) and data were analyzed by using FlowJo V10 (BD Bioscience, San Jose, CA, USA).
Statistical analysis
Statistical analysis was performed using GraphPad Prism 6 (GraphPad Software Inc., San Diego, CA, USA). Differences between paired baseline, and 2-month samples and 6-month samples were analyzed using a Wilcoxon matched-paired rank test or a Kruskal–Wallis when applicable. Receiver operator characteristic (ROC) curve analysis was used to test the ability of frequencies of CD27−, CD38+, and CD27−CD38+ distinguish treated and untreated PTB. A two-sided P < 0.05 was considered statistically significant.







留言 (0)