
記住我


To the Editor: Tumor immune microenvironment plays a key role in breast cancer development and progression, which determines the long-term survival of breast cancer patients. Recent data have revealed that the application of cancer immunotherapy has some limitations, including generating weak immune responses due to inadequate delivery of immunostimulants to the immune cells.[1] Thus, current clinical efforts are primarily focused on developing immune-based chemotherapy that can convert non-responders to responders.[2] Immunogenic cell death (ICD) is a form of regulated cell death that is sufficient to activate an adaptive immune response. ICD can be usually triggered by certain chemotherapeutic drugs, oncolytic viruses, physicochemical therapies, and radiotherapy.[3] Notably, a significant advantage of ICD, as a class of biomarkers, is that it integrates several immune-related pathways including danger signaling and T cell infiltration/activity. Some studies conducted to ascertain the prognostic value of ICD parameters have yielded contradictory results, which might be because of a limited number of patients and restricted ICD parameters. In this study, significant ICD-related biomarkers were identified and ICD-related signatures were derived to estimate the infiltration of immune cells, response to immunotherapy, and prognosis in breast cancer. Besides, a nomogram based on the independent clinicopathological factors and ICD risk scores was constructed for predicting the long-term survival of breast cancer patients, which may help in improving the clinical management of breast cancer patients.
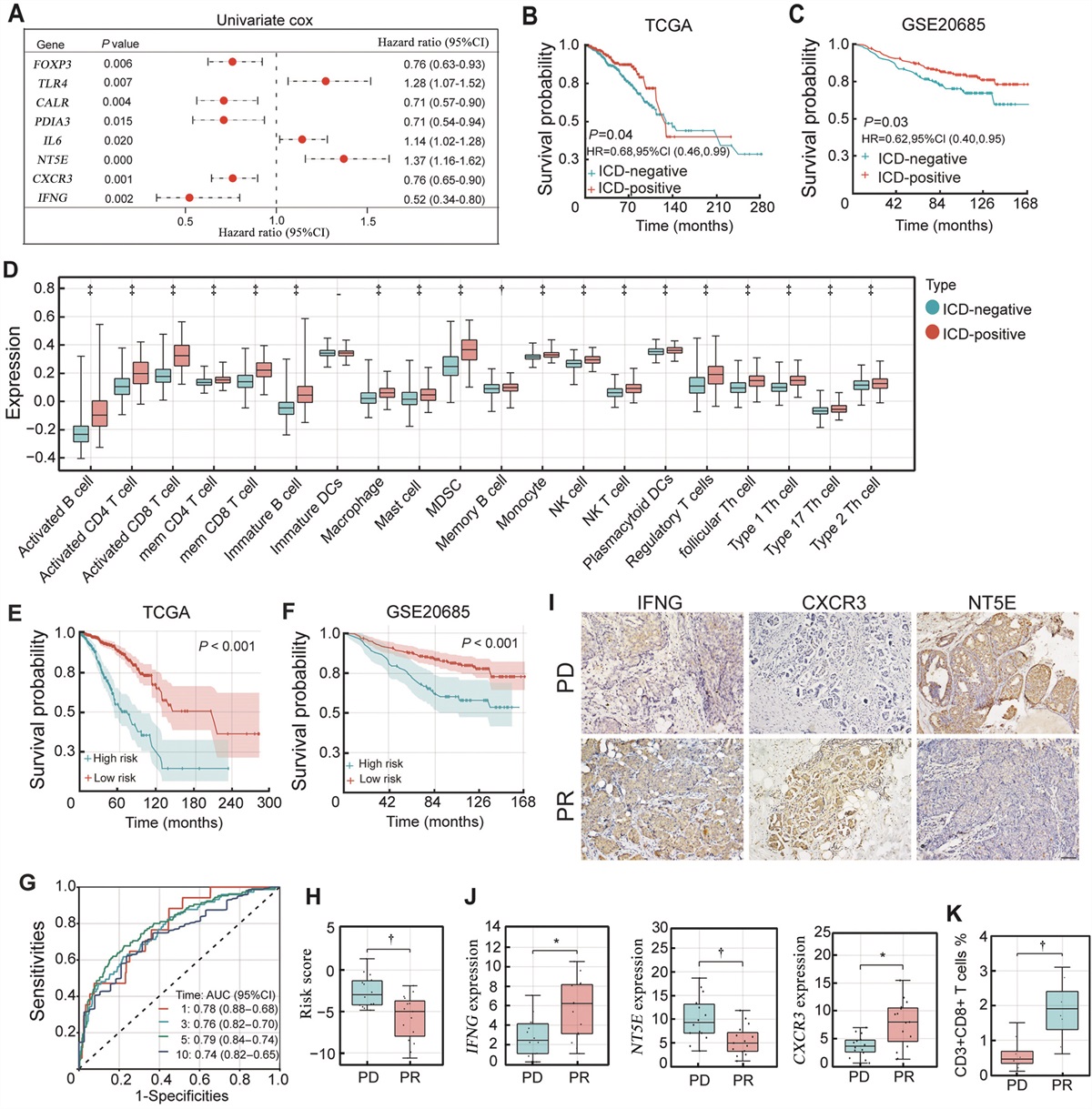
We initially analyzed the expression of 34 reported ICD associated genes in 1050 breast cancer patients from The Cancer Genome Atlas (TCGA) database.[4] We found that 26 ICD-related genes were significantly differentially expressed ([log2FoldChange] >2, P <0.05) in breast cancers [Supplementary Figure 1A, https://links.lww.com/CM9/B743]. We further indicated that FOXP3, CALR, PDIA3, CXCR3, and IFNG were favorable prognostic factors, while TLR4, IL6, and NT5E were associated with poor survival in breast cancer by univariate Cox analysis [Figure 1A]. Further, the protein expression levels of these genes were also performed on the Human Protein Atlas, which revealed remarkably different expression levels in breast cancer tissues [Supplementary Figure 1B, https://links.lww.com/CM9/B743]. Based on these findings, ICD-related clusters in breast cancer were then determined by consensus clustering [Supplementary Figure 1C, https://links.lww.com/CM9/B743]. Overall, cluster C2 (ICD-positive) showed higher expression levels of favorable ICD-related genes, whereas, cluster C1 (ICD-negative) exhibited higher expression levels of unfavorable ICD factors [Supplementary Figure 1D, https://links.lww.com/CM9/B743]. The ICD-positive cluster showed a significantly improved overall survival (OS) compared to the ICD-negative cluster both in the TCGA (P = 0.04, hazard ratio [HR] 0.68, 95% confidence interval [CI] [0.46, 0.99]) and GSE20685 (P = 0.03, HR 0.62, 95% CI [0.40, 0.95]) [Figures 1B,C], highlighting the prognostic value of these ICD-related genes.
 Figure 1:
Figure 1: (A) Forest plot of the univariate Cox regression analyses of 26 ICD-related genes in breast cancer. (B,C) Kaplan–Meier curves of OS in ICD-negative and ICD-positive clusters from TCGA cohort (B) or GSE20685 (C). (D) The differential expression of 22 immune cells in two ICD subtypes analyzed by ssGSEA. (E,F) Kaplan–Meier curves of high or low risk breast cancer patients in TCGA (E) and GSE20685 (F) cohort. (G) Time-dependent ROC analysis for assessing the predictive significance of ICD-related signature. (H) The ICD-related risk score of PD and PR breast cancer patients after combined immunotherapy. (I) The immunostaining of IFNG, CXCR3, and NT5E in PD and PR patients, respectively. The scale bar was 200 μm. (J) The expression intensity of IFNG, CXCR3, and NT5E was quantified. (K) The infiltration proportion of CD3+ CD8+ T cells in tumor tissues. *P <0.05, †P <0.01, ‡P <0.001. ICD: Immunogenic cell death; OS: Overall survival; PD: Progressive disease; PR: Partial response; ssGSEA: Single-sample gene set enrichment analysis.
A total of 681 differentially expressed genes (DEGs) were obtained between the two clusters ([log2FoldChange] >2, P <0.05) [Supplementary Figures 2A,B, https://links.lww.com/CM9/B743]. The Gene Ontology (GO) enrichment and Kyoto Encyclopedia of Genes and Genomes (KEGG) analyses were conducted to determine the biochemical functions of the upregulated genes [Supplementary Figures 2C,D, https://links.lww.com/CM9/B743]. The terms were most significantly enriched in the regulation of the immune system, including cytokine receptor interaction, regulation of T cell activation, and T cell receptor signaling. Gene Set Enrichment Analysis (GSEA) analysis indicated that pathways associated with immunity, including lymphocyte activation, adaptive immune response, and T cell activation, were differentially activated in two clusters [Supplementary Figure 2E, https://links.lww.com/CM9/B743]. These findings indicated that the improved prognosis in the ICD-positive subtype might be attributed to a more active immune microenvironment.
Thus, the compositions of tumor immune microenvironment of two ICD subtypes were compared using the ESTIMATE approach. The ICD-positive subtype revealed a remarkably lower tumor purity and a significantly higher immune score [Supplementary Figure 3A, https://links.lww.com/CM9/B743]. Further, the different immune infiltration characteristics were determined in two ICD subtypes using the CIBERSORT approach [Supplementary Figure 3B, https://links.lww.com/CM9/B743]. Particularly, the ICD-positive patients exhibited a significantly higher percentage of activated cluster of differentiation (CD)8+ T cells, activated CD4+ T cells, natural killer (NK) cells, dendritic cells (DCs), and M0 and M1 macrophages [Figure 1D and Supplementary Figure 3C, https://links.lww.com/CM9/B743]. Despite increased myeloid-derived suppressor cells (MDSC) and regulator T cell (Treg) infiltration in ICD-positive patients, it was reported that the balance between effector T cells (Teff) and regulator T cells and the relative proportion are more crucial in determining the outcome of an immune response.[5] More importantly, the key immune checkpoints were significantly upregulated in ICD-positive patients [Supplementary Figure 3D, https://links.lww.com/CM9/B743]. These results highlighted that the ICD-positive subtype was associated with the immune-hot phenotype, while the ICD-negative subtype favored the immune-cold phenotype.
In order to further investigate the clinical significance of ICD clusters, we established a prognostic signature using the eight ICD genes that were shown to be related to prognosis in two ICD clusters. We analyzed 1050 breast cancer patients with baseline characteristics from TCGA and constructed a prognostic signature using Lasso-penalized Cox analysis [Supplementary Figure 4A, https://links.lww.com/CM9/B743]. The risk-score model was developed based on the following algorithm: Risk score = 0.2525 × NT5E + 0.0559 × TLR4 + 0.0313 × IL6 + (–0.0366) × PDIA3 + (–0.2950) × IFNG + (–0.0475) × CALR + (–0.1770) × CXCR3. The results revealed that the number of deaths in the high-risk cohort was much greater than in the low-risk cohort [Supplementary Figure 4B, https://links.lww.com/CM9/B743]. The patients in the high-risk cohort had a significantly poorer OS than the patients in the low-risk cohort (P <0.01) [Figures 1E,F]. The area under curves (AUCs) for 1-year, 3-year, 5-year, and 10-year OS were 0.78, 0.76, 0.79, and 0.74, respectively [Figure 1G]. Furthermore, the ICD risk signature could serve as an independent prognostic factor for breast cancer patients [Supplementary Figure 4C, https://links.lww.com/CM9/B743]. Based on these findings, a nomogram was further constructed to predict 1-year, 3-year, 5-year, and 10-year OS of breast cancer patients [Supplementary Figure 4D, https://links.lww.com/CM9/B743]. A combination of ICD risk signature and conventional clinical parameters could effectively better predict the long-term survival of breast cancer patients.
We further verified the clinical significance of ICD-signature in 29 metastatic breast cancer patients treated with immunotherapy in our clinical trial [Supplementary Figure 5A, https://links.lww.com/CM9/B743]. It is noteworthy that the patients with progressive disease (PD) exhibited significantly higher risk score, compared with patients with partial response (PR) [Figure 1H]. The patients with PR consistently manifested a remarkably higher expression of IFNG and CXCR3, the major favorable factors in ICD-related signatures. On the contrary, a high expression of NT5E, the major risk factor, was observed in patients with PD [Figures 1I,J]. Meanwhile, it was demonstrated that the PR patients, with lower ICD-related risk scores, displayed an increased infiltration of CD3+ CD8+ T cells, which were associated with an immune hot phenotype and a better response to immunotherapy [Figure 1K and Supplementary Figure 5B, https://links.lww.com/CM9/B743]. Briefly, these results indicated that the ICD-related risk signature could predict the immune infiltration and immunotherapy response in breast cancer patients.
In this study, an ICD-related risk signature was constructed and validated for predicting the immune microenvironment, immunotherapy response, and prognosis in breast cancers. Further, the nomogram prognostic model combined the ICD risk signature with the conventional clinicopathological parameters such as the TNM stage, thereby improving the prognostic performance in the long-term survival of breast cancer patients. Our results highlighted the crucial role of ICD in breast cancer immunotherapy, and provided a novel stratification and prognostic model for clinical management.
Conflicts of interestNone.
Ethical approvalThe patients involved in open-source data (TCGA and GEO public datasets) have given consent and the authors have obtained ethical approval. The clinical patients included in this study were informed of the research, together with written consent being obtained. Ethical review was granted by the Ethics Committee of the National Cancer Center (No. NCT04389073).
References 1. Bahreyni A, Mohamud Y, Luo H. Emerging nanomedicines for effective breast cancer immunotherapy. J Nanobiotechnology 2020;18: 180. doi: 10.1186/s12951-020-00741-z. 2. Emens LA. Breast cancer immunotherapy: Facts and hopes. Clin Cancer Res 2018;24: 511–520. doi: 10.1158/1078-0432.Ccr-16-3001. 3. Galluzzi L, Vitale I, Aaronson SA, Abrams JM, Adam D, Agostinis P, et al. Molecular mechanisms of cell death: Recommendations of the nomenclature committee on cell death 2018. Cell Death Differ 2018;25: 486–541. doi: 10.1038/s41418-017-0012-4. 4. Garg AD, De Ruysscher D, Agostinis P. Immunological metagene signatures derived from immunogenic cancer cell death associate with improved survival of patients with lung, breast or ovarian malignancies: A large-scale meta-analysis. Oncoimmunology 2016;5: e1069938. doi: 10.1080/2162402x.2015.1069938. 5. Hariyanto AD, Permata TBM, Gondhowiardjo SA. Role of CD4(+)CD25(+)FOXP3(+) T(Reg) cells on tumor immunity. Immunol Med 2022;45: 94–107. doi: 10.1080/25785826.2021.1975228.
留言 (0)