Agreement between intermittent glucose concentrations and continuous glucose monitoring in at-risk newborns
Neonatal hypoglycemia (NH) is the most common metabolic disturbance affecting newborns, and has been linked with poor academic performance [1]. Many knowledge gaps persist regarding its definition, long-term impact, screening and management, and proper measurement and monitoring of glucose concentrations [2].
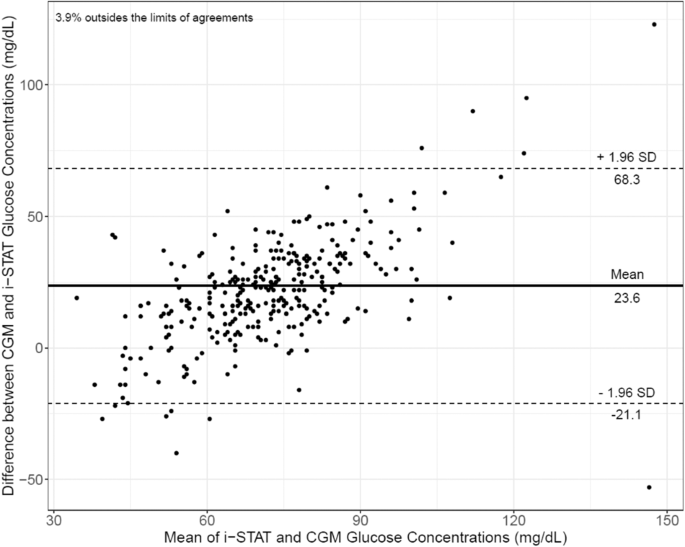
Current hypoglycemia screening involves intermittent glucose measurement using point-of-care (POC) glucometers. Samples are obtained every few hours per NH screening protocols. Additional painful needle sticks are performed for (1) laboratory confirmation of low POC values, (2) serial pre-prandial testing, and (3) placement of intravenous catheters for parenteral treatment of NH. Continuous glucose monitoring (CGM), in contrast, holds promise as a less painful method of evaluating glucose concentrations continuously in order to identify dysglycemia and improve family-centered care and parental satisfaction. It requires only one needle stick during CGM sensor placement and reports interstitial glucose concentrations every 5 min. Repeated and prolonged hypoglycemia as well as glycemic instability are associated with adverse neurological outcomes; [2] these episodes cannot be fully evaluated with current intermittent POC technology. Thus, CGM has the potential for increased detection of these potentially harmful episodes, which will enable timely treatment. The single center REACT feasibility pilot trial evaluating the use of CGM in very preterm infants reported low bias (−4.9 mg/dL, 95% CI −6.3 to −3.4 mg/dL, n = 20) when the CGM was calibrated every 12 h [3, 4]. An agreement study of glucose concentrations between CGM (that does not require calibration) and intermittent values in at-risk late preterm and term newborns, who represent the majority of newborns with hypoglycemia, however, is lacking. Thus, our pilot study aimed to assess the accuracy of CGM in at-risk newborns.


留言 (0)