Diffuse midline glioma (DMG) is the sole tumor type for which grading is determined through a combination of molecular profiling and histopathological alterations. These tumors are commonly located in midline structures such as the thalamus, brainstem, and spinal cord [6]. Less common sites include the third ventricle, hypothalamus, pineal region, and cerebellar hemispheres [7].The patients in this study were primarily located in the thalamus, brainstem, and spinal cord, consistent with the literature reports. The clinical manifestations of DMG primarily depend on the location of the tumor. The clinical manifestations of the patients in this study included blurred vision, limb weakness, strabismus, headache, and dizziness, which are consistent with the literature reports [8].
In the diagnosis of the patient cohort under study, the criteria included radiological evidence of diffuse infiltrative growth centered on midline structures. The determination of H3K27M mutation status was conducted using immunohistochemistry (IHC), which facilitates the identification of mutations, particularly in the diagnosis of H3K27M-mutant diffuse midline gliomas. Multiple studies have reported a significant correlation between the expression of the H3K27M protein and the presence of H3K27M mutations [9]. The histopathological spectrum of DMG with H3K27M alterations is broad, primarily characterized by astrocytic differentiation. It can manifest in any form ranging from WHO grade 2 diffuse astrocytoma to WHO grade 4 glioblastoma multiforme (GBM), or multiple forms can coexist in different regions. There is no significant difference in the histological grade distribution between adult and pediatric patients [10, 11].Solely relying on histopathological grading to predict patient prognosis has its limitations. In our study group, the histopathological types of tumors included diffuse astrocytoma (WHO grade 2, 9 cases), anaplastic astrocytoma (WHO grade 3, 12 cases), and GBM (WHO grade 4, 24 cases). Some patients did not receive specific histopathological subtyping due to variations in pathological standards across different regions. Upon univariate and multivariate analysis, the histopathological type did not significantly impact prognosis, with no statistical significance observed.
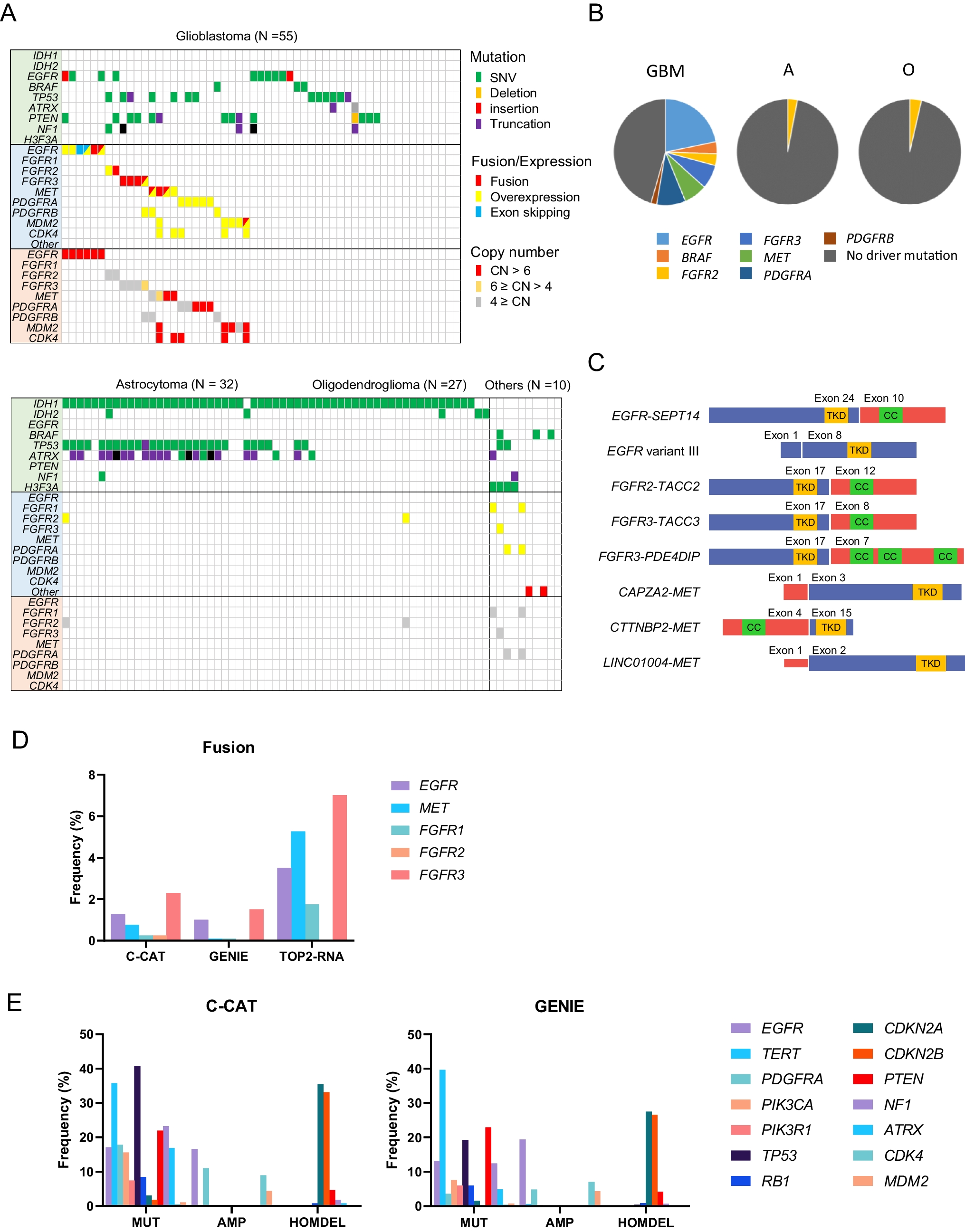
The treatment of gliomas has entered the era of molecular profiling, with pivotal genomic studies highlighting the significance of molecular markers such as IDH mutations, 1p/19q codeletion, MGMT promoter methylation, ATRX mutations, TERT promoter mutations, PTEN mutations, and TP53 mutations and so on. These studies have revealed that diffuse intrinsic pontine gliomas (DIPGs) are driven by somatic mutations in the histone H3 gene, defining subgroups with distinct biological and clinical phenotypes and prognoses. Various indicators have differential impacts on the prognosis of gliomas [12]. The Ki67 index serves as an indicator of tumor proliferation rate. In the context of DMG, although the prognostic utility of conventional histological grading alone is limited, the Ki-67 index has demonstrated prognostic value, with similar findings reported in other gliomas [13, 14]. Studies have shown a strong correlation between higher Ki-67 indices and larger tumor volumes in glioblastoma multiforme [15]. Furthermore, elevated Ki-67 indices in DMG are associated with a higher frequency of hypermutated alleles, which in turn correlates with poorer survival rates [16]. In our study, patients were stratified based on a median Ki67 index of 27%, with those exhibiting higher indices tending to have shorter survival periods, although this did not reach statistical significance. These findings suggest that DMGs exhibit considerable heterogeneity, with a multitude of prognostic factors influencing outcomes. Further research is warranted to refine potential markers for study.
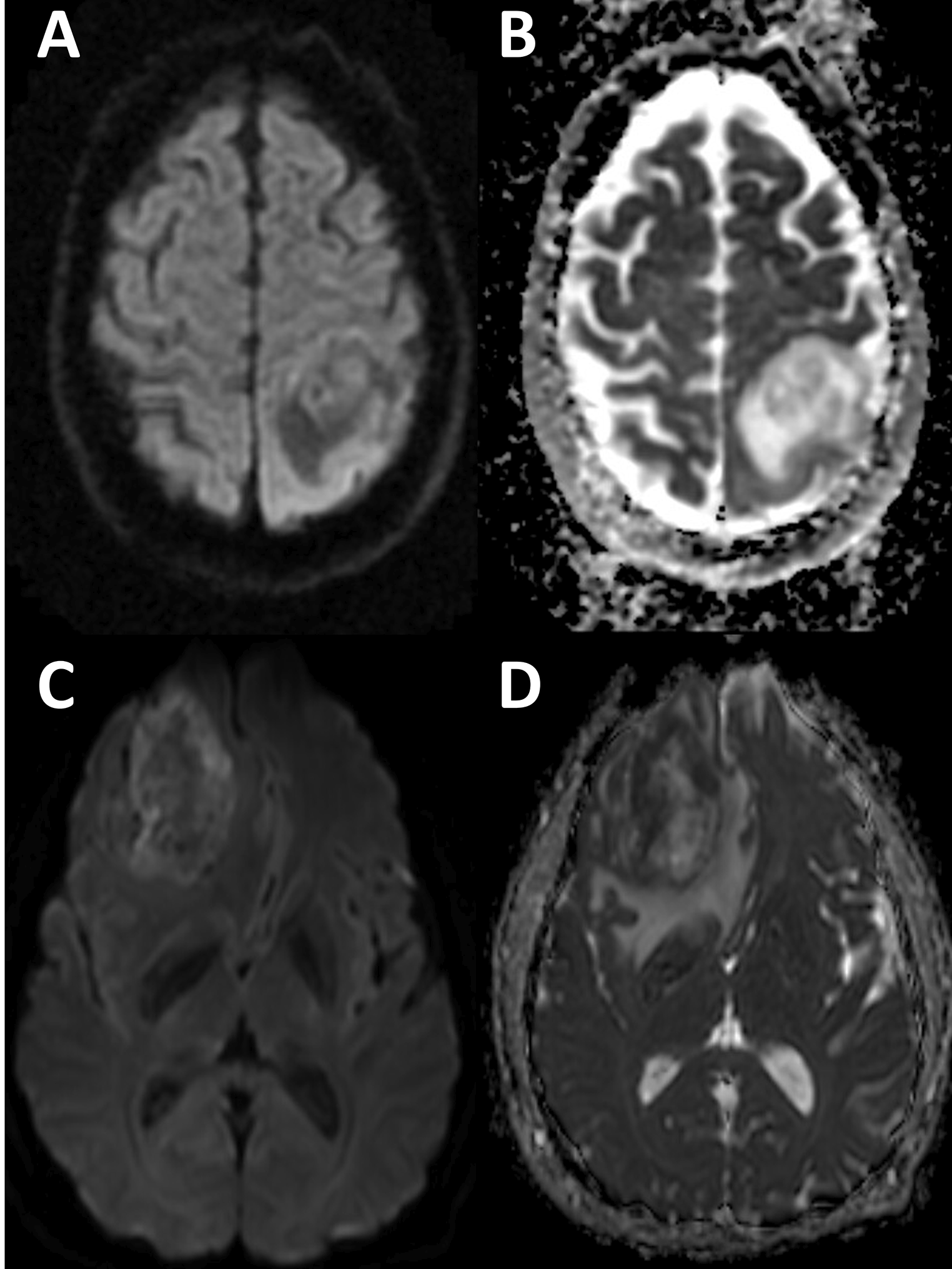
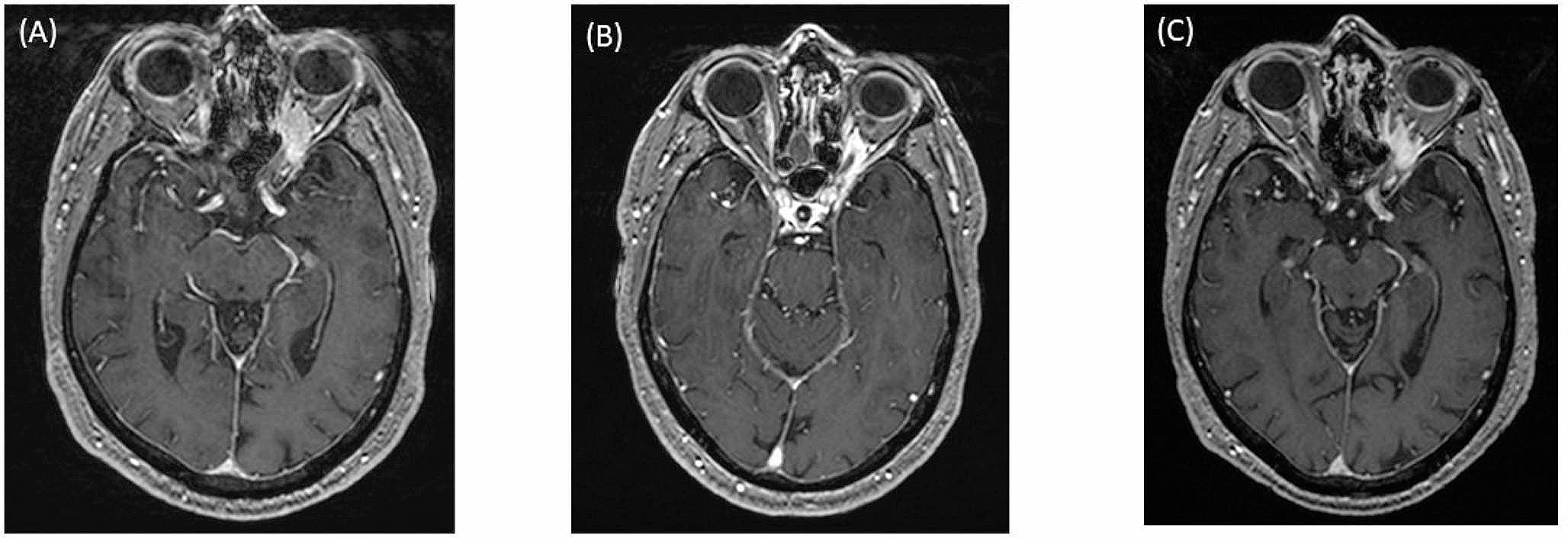
Patients with DMG typically exhibit radiological features characterized by diffuse infiltrative growth, accompanied by varying degrees of enhancement, edema, necrosis, and hemorrhage. The imaging characteristics of adult DMG have yielded divergent results across several studies [17,18,19,20]. To date, no distinct structural imaging features have been identified, which may be attributed to their lower incidence and the recent recognition of DMG as a separate entity [20]. The highly variable appearances on MRI are largely due to the heterogeneity of tissue pathology, which in turn reflects the histopathological diversity of DMG [19]. The radiological findings in our cohort are consistent with those reported in the literature, with no unique imaging features observed.
Surgical resection is a critical initial treatment modality for gliomas, with higher rates of resection correlating with increased survival [21,22,23]. Liu et al. [24] collected data from 529 patients with brainstem gliomas and found that the group with complete resection had the highest overall survival rate. In the subgroup of children with low-grade brainstem gliomas (BSG), those who underwent complete resection had a significantly higher survival rate compared to those who did not. However, in adults with low-grade BSG and children with high-grade BSG, the survival rates were higher in the complete resection group, but the differences were not statistically significant. Clinical studies indicate that patients with focal low-grade brainstem and dorsally exophytic tumors may benefit from surgical resection [25]. Ius et al. [26] reported that the incidence of complications following biopsy and surgical resection for high-grade brainstem gliomas was 10.5% and 35.5%, respectively, p = 0.009, indicating a statistically significant difference. For patients with DMG, due to the location of the lesion in the midline structures of the brain and spinal cord, the difficulty of surgical resection makes the impact of the extent of tumor removal on prognosis unclear. Karemann and colleagues assessed 85 pediatric patients with DMG and found that the extent of resection was not associated with prognosis [27]. The HERBY trial, which included 42 patients with thalamic DMGs, demonstrated an association between maximal tumor debulking or near-total resection and extended overall survival [28]. The aforementioned studies highlight the impact of anatomical location on the completeness of surgical resection and the probability of postoperative complications, both of which may influence the prognosis of DMG patients. Further refined research is necessary to screen and select patients suitable for surgery to ascertain the role of surgical intervention in the treatment of DMGs. In this cohort, the extent of surgical resection was not fully documented, only biopsy and surgical procedures were stratified for analysis, with no statistical difference observed.
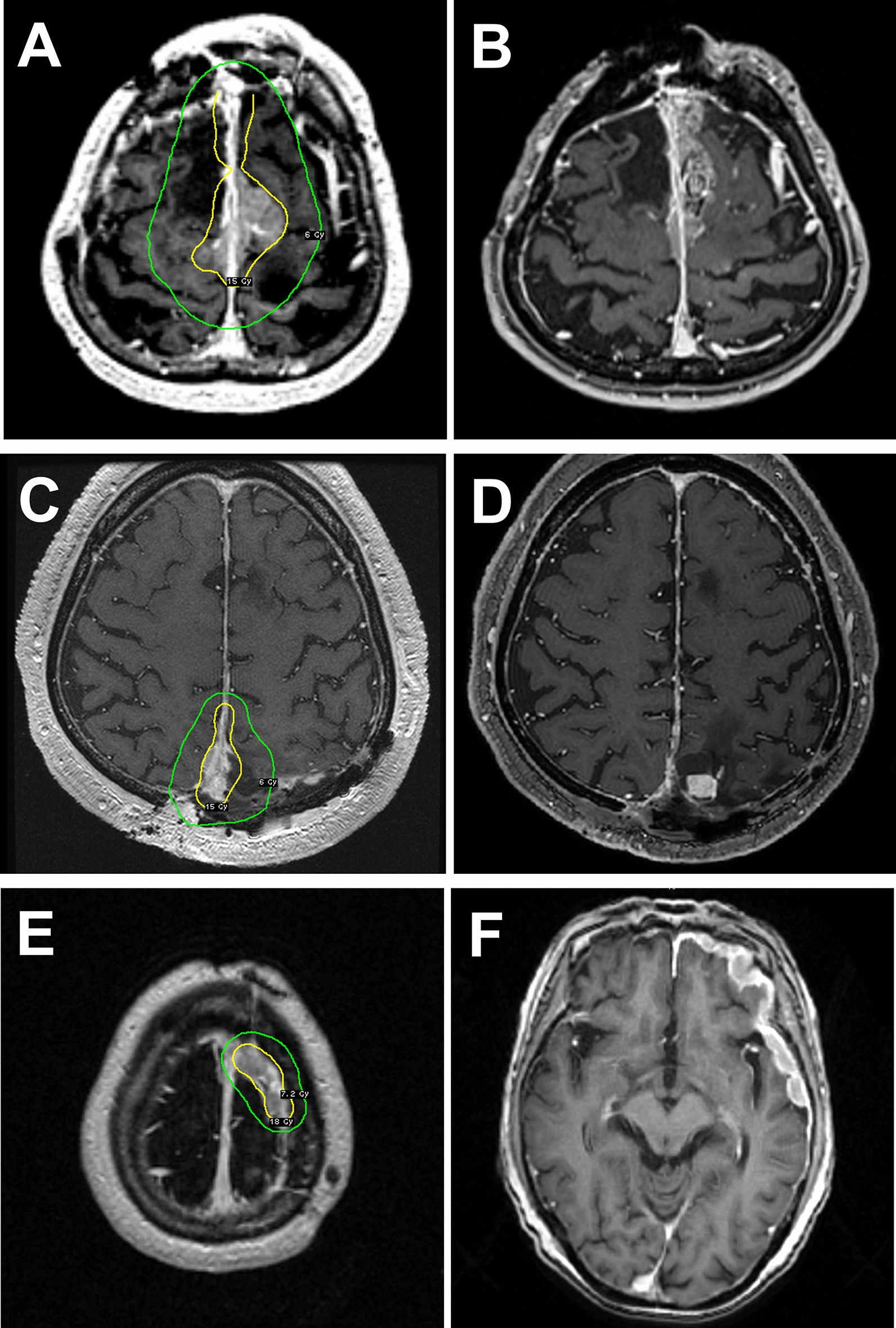
When complete surgical resection is not feasible, conventional high-dose fractionated radiotherapy and temozolomide chemotherapy are the primary treatment options [29, 30]. However, comparisons of different treatment regimens in children and adults, such as concurrent chemoradiotherapy, post-radiotherapy chemotherapy, radiotherapy alone, or chemotherapy alone, have not demonstrated statistically significant advantages [17, 29, 31]. Therefore, treatment approaches should be tailored to each individual case [29]. The overall prognosis for DMG is poor, and improving the survival of patients with DMG is an increasingly researched topic. Radiotherapy remains the mainstay of treatment and its efficacy is well-established. A study by Othman Bin-Alamer et al. [32] found that the survival time of patients who received radiotherapy was significantly longer than those who did not, with a P < 0.019. Given the importance of radiotherapy in the treatment of DMG, it is essential to investigate prognostic factors associated with it.
In their comprehensive description of the characteristics of DMG, Carlos et al. [33] reported a generally poor overall survival for the condition, with a median survival duration of 9–12 months in children and 9–19 months in adults. Studies comparing prognostic differences between the two age groups indicate that pediatric patients have nearly identical poor outcomes [34] or even worse prognoses [29] when compared to adults. DMG is common in children and adolescents but can also occur in middle-aged and elderly individuals, with no significant gender differences [34]. Literature reports indicate that the average age at diagnosis ranges from 25 to 39.1 years [35,36,37]. In a survival analysis conducted by Yao et al. [38] on 33 patients with DMG, it was observed that survival duration increased with age. Notably, patients older than 45 years exhibited a significantly better prognosis than those younger than 19 years (P = 0.001). However, Cox regression analysis did not confirm this result as statistically significant. The age range of the patients in this study was 6–56 years, with a noticeable trend across all age groups. After stratifying by the median age of 32 years, both univariate and multivariate analyses were conducted, all of which were statistically significant. This suggests that age is an independent prognostic factor for patients undergoing radiation therapy for DMG.
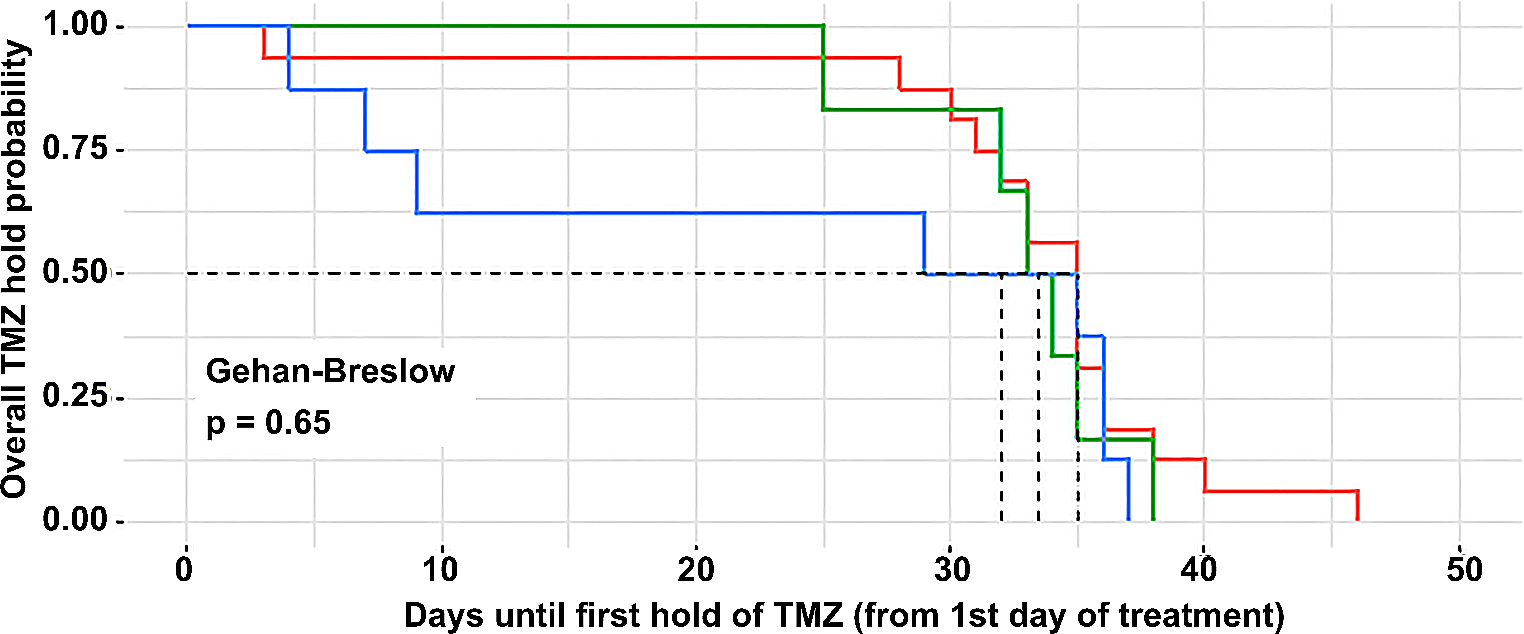
The therapeutic efficacy of the chemotherapeutic agent temozolomide in the treatment of glioblastoma continues to emerge, as exemplified by a clinical study conducted by the European Organisation for Research and Treatment of Cancer (EORTC). Stupp R and colleagues [39, 40] analyzed data from 573 patients with glioblastoma, finding that the median survival was significantly longer in the group receiving concurrent radiotherapy and chemotherapy (14.6 months) compared to the radiotherapy-only group (12.1 months). This has led to an increasing number of scholars advocating for the use of temozolomide in the treatment of glioblastoma. However, research by Julia R et al. [41] on the concurrent chemoradiotherapy with temozolomide in pediatric patients with diffuse intrinsic pontine glioma did not yield meaningful results. Temozolomide has also been employed as a first-line treatment for diffuse midline glioma (DMG), yet its efficacy has been suboptimal in several studies [29,30,31]. TMZ not only exerts cytotoxic effects but also possesses a variety of immunomodulatory functions. It can activate compensatory release of cytokines, lower the activation threshold and proliferation of T cells, thereby eliciting a more robust immune response. Despite the potential benefits of chemotherapy, the therapeutic efficacy is limited due to the integrity of the blood-brain barrier (BBB) in most cases of DMG [30, 32]. Compared to radiotherapy alone, TMZ has not demonstrated improvement in tumor burden or overall survival, and is associated with an increased risk of side effects and toxicity. In the absence of other suitable chemotherapy options, TMZ may be considered as a first-line chemotherapeutic regimen for DMG patients during and post-radiotherapy. In our study, patients who received concurrent temozolomide chemotherapy during radiotherapy had mild and tolerable side effects, but no survival advantage was demonstrated. This may be related to the retrospective nature of the study and an imbalance in case selection. Whether it can provide value for patients with higher histopathological grades requires further research with a larger sample size.
Our study has certain limitations. Firstly, due to the accessibility of medical records, patient imaging and surgical data were incomplete. The inclusion of patients from various institutions, which have differing levels of recognition and understanding of DMG, as well as disparities in molecular pathology capabilities, resulted in incomplete acquisition of certain molecular markers, precluding their evaluation. Future work will involve the standardization of assessment criteria for a more in-depth analysis. We plan to standardize the assessment criteria for a more in-depth analysis in the future. Additionally, the small number of cases necessitates the expansion of the sample size for a more thorough investigation.
Preliminary research indicates that patient age significantly impacts the survival rate of those undergoing radiotherapy for DMG. Other factors did not appear to confer a survival benefit for patients with DMG. At present, radiotherapy remains the primary treatment modality for DMG. Future research is needed to explore alternative radiotherapy approaches or the use of sensitizing agents to enhance the efficacy of radiotherapy. Currently, there is a burgeoning body of basic and translational research on DMG, providing insights into pathology, disease mechanisms, and novel treatment strategies that may inform clinical trials. These advances hold promise for improving the poor prognosis of DMG patients through combination therapies. We aim to increase the sample size and refine patient categorization to provide reference indicators for the formulation of clinical treatment plans, offering new hope for patients with DMG.

留言 (0)